

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Patients complained of repeated epiphora need to evaluate nasolacrimal drainage system because the commonest cause of epiphora is nasolacrimal duct obstruction (NLDO). The location of obstruction or stenosis can be precisely located if there are obvious causes of obstruction like previous trauma, infection, inflammatory diseases such as sarcoidosis and Wegener's granulomatosis, or malignancy [12]. However, most cases of NLDO are associated with unknown origins, so many recent studies used computed tomography (CT) imaging to evaluate periocular pathology and nasolacrimal drainage system [345]. They recommend CT as a diagnostic tool for NLDO when cause of obstruction is uncertain [678].
Treatment of NLDO is mainly dependent on surgical managements which include external or endonasal dacryocystorhinostomy (DCR), balloon catheter dilatation, and silicone intubation. Endonasal DCR became a widely used standard procedure performed for NLDO because of advancements in local anesthesia, and the vastly improved visibility in the operative field provided by endoscopy. A facial incision which can hamper the pumping action of orbicularis oculi muscle is not required in endonasal DCR and it has shorter recovery period than external DCR [9].
We believe that thorough clinical assessments, including taking history of any nasal or sinus disorders, doing regurgitation test, syringing of lacrimal sac, and contrast dacryocystography (DCG), NLDO can be evaluated enough. Also, additional preoperative nasal endoscopy may ensure the appropriate lacrimal operation. So, CT is usually not recommended if there is certainty of patient's diagnosis.
Although CT is not routine evaluation for watery eyes, drainage-limiting factors such as bony abnormalities, mucosal edema, retention of secretions, and obstructive masses are readily identified on CT which makes it a good diagnostic tool. For these reason, otolaryngologists who undertake functional endoscopic sinus surgery almost routinely obtain a CT scan before undertaking surgery in order to evaluate the exact bony structures and the mucous membranes of patients. There are many published reports of abnormalities in lacrimal sacs, orbital walls, and sinuses, which could affect the final results of endonasal DCR [710111213]. Even though the incidence of abnormal anatomic findings is rare, knowing the exact state of nearby structures of the lacrimal drainage system can reduce surprises during the surgery and it is useful to ensure proper treatments to the patients.
Still there has been no recent studies about usefulness of preoperative CT on patients with NLDO since Francis et al. [6] reported on the value of CT imaging in patients with symptoms of lacrimal drainage obstruction. Therefore, we evaluated the role of preoperational CT in patients with NLDO.
Materials and Methods
We retrospectively reviewed the medical records and CT results on 218 patients who complained of tearing symptoms with NLDO who were planned to undergo DCR surgery between January 2014 and December 2014. All patients were recruited from Kim's Eye Hospital's outpatient clinic, and diagnosis of NLDO was made clinically by doing conventional probing, syringing and confirmed by DCG with contrast. DCG was done in all patients and they were examined of puncta, ocular surface, tear film and CT to rule out any eyelid malposition, disease of the eyelid margin, bony or soft tissue abnormalities. A history of sinonasal disease, previous sinus or facial surgery, allergic rhinitis and trauma were obtained. Patients were routinely followed up at 1 week, 1 month, 3 months, 6 months, and 12 months postoperatively. The patency of nasolacrimal duct (NLD) was assessed by doing syringing of lacrimal passage on every follow ups. No additional procedures were performed during this period.
A total of 218 patients underwent supine axial imaging using a Siemens Somatom Spirit dual-slice CT scanner (Siemens, Munich, Germany) with images obtained at 1.0-mm intervals. All patients' CT images were interpreted by radiologist and reviewed by three masked observers for presence of air within the nasolacrimal drainage system and other abnormalities around orbit. The NLD was classified as full opacity, partial opacity, and no opacity. The term "no opacity" was used if air in the lacrimal sac and NLD was seen in continuity on contiguous slices.
We analyzed patient demographics and radiologic characteristics on CT scans, including the abnormalities of orbit, sinus and other facial structures. Patients with abnormal findings assessed by preoperative CT were prescribed management and treatment according to each abnormality. All patients with abnormal findings assessed by preoperative CT were further reviewed.
We also reviewed the differences of CT imaging between eyes which found to have obstruction (which DCR were performed) and eyes which showed no obstruction (which are the contralateral eyes of patients who undergo unilateral DCR). Statistical analyses were performed with the commercially available software package SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). Differences in values between eyes with NLDO and eyes without NLDO were analyzed using linear by linear association. A p-value less than 0.05 was considered significant.
Results
CT was performed on 218 patients (average age, 58.2 ± 11.9 years; range, 14 to 83 years). There were 52 men (23.9%) and 166 women (76.1%). Of these 218 patients, 196 (89.9%) had endonasal DCR, 14 (6.4%) declined surgery, and 8 (3.7%) were inoperable due to abnormal CT findings. For the 196 patients who received endonasal DCR, 54 (27.6%) had right side DCR, 55 (28.1%) had left side DCR, and 87 (44.4%) had bilateral DCR. Patient demographics are summarized in Table 1.
Endonasal DCR was performed on 283 NLDs of 196 patients. Postoperative success was evaluated by syringing and examination of rhinostomy site which was good passage with patent opening. A total 184 (93.9%) of 196 patients were fully satisfied. In 9 cases (4.6%), minimal block was seen with clear fluid regurgitation and to some extent their symptom was relieved. However, three patients (1.5%) with mucoid regurgitation or complete block were not relieved of their symptoms and needed further intervention.
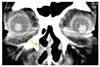
The most common abnormal CT finding was soft tissue opacity, which showed no air and it reflects mucosal thickening whining the NLD and retention of secretions (Fig. 1A-1D). CT scans of 196 individuals who underwent DCR were reviewed in the coronal and axial plane by three independent reviewers for the soft tissue opacity. Because not all the patients underwent bilateral DCR, 392 NLDs include 283 obstructed NLDs (87 bilateral : 54 left : 55 right) which underwent DCR and 109 non-obstructed NLDs (54 left : 55 right) which didn't undergo DCR. Two hundred forty-three (85.9%) of 283 obstructed NLDs showed full opacity, 19 (6.7%) NLDs showed partial opacity, and 21 (7.4%) NLDs showed no opacity. Eighty-nine (81.7%) of 109 non-obstructed NLDs showed full opacity, 10 (9.2%) NLDs showed partial opacity, and 10 (9.2%) NLDs showed no opacity (Table 2). Patients with tearing problems showed higher incidence of soft tissue opacity in NLDs but there were no statistical differences between two groups (p = 0.362).
The second most common abnormal CT finding was chronic rhinosinusitis (CRS), which included maxillary sinusitis and ethmoidal sinusitis. There were 39 (17.8%) of 218 patients whose CT results showed either maxillary sinusitis or ethmoidal sinusitis. Of these, 31 (14.2%) showed maxillary sinusitis, 18 (8.3%) showed ethmoidal sinusitis, and 10 (4.6%) showed both. When patients with rhinosinusitis underwent surgery, they routinely received preoperative and postoperative antibiotics. They were checked more often at our clinic after endonasal DCR.
We observed 32 cases (14.7%) of periocular inflammation, which included dacryocystitis and periorbital cellulitis without lacrimal sac inflammation; 23 patients (10.6%) had dacryocystitis, and 9 (4.1%) had periorbital cellulitis without lacrimal sac inflammation. Other abnormal CT findings were septal deviations, previous fractures, masses, and structural abnormalities of nasal cavity. Twenty-six cases (11.9%) had septal deviation and were referred to otolaryngologists before undertaking surgery. Of these 26 patients, 18 had severe deviation which required septoplasty before DCR and eight had mild deviation which underwent DCR without septoplasty. In 16 cases (7.3%), we found previous fractures; 15 patients had orbital wall fractures and one patient had a nasal bone fracture. All of the fractures were old events and had no effect on proceeding to surgical intervention for these patients. In seven patients, masses were found on CT; five (2.3%) had paranasal sinus masses, one had a lid mass, and one had a zygoma mass.
Nasal abnormalities were found in four cases. They were two cases of mucocele, one of nasal polyp, and one of trauma-induced nasal deformity. Details of the abnormal CT findings and number of patients are summarized in Table 3.
Two cases of 196 DCRs developed acute rhinosinusitis within the first 5 days following DCR and both had a past history of CRS that had been asymptomatic at the time of surgery. They were treated with a 1 to 3 week course of oxymetazoline hydrochloride nasal spray and oral ofloxacin three times daily.
Case 1
One patient came to our clinic complaining of epiphora and had a history of nasal trauma at young age. When examining his nose, his right nostril was completely obstructed by mucosa, and thus could not be examined further. His CT showed membranous obstruction of his right nostril (Fig. 2), which required ear, nose, and throat surgery to open the obstructed nasal cavity before performing DCR.
Case 2
One patient with a tearing problem for 2 to 3 months came to our clinic. Syringing revealed no abnormalities. Since his DCG showed irregular passages of dye, we recommended a CT examination. His CT results revealed that his right maxillary sinus and ethmoid soft tissue was filled with irregular bony disruptions, and he was referred to a tertiary hospital for assessment of possible inverted papilloma (Fig. 3A and 3B).
Case 3
We assessed a 58-year-old male patient who presented with epiphora, anosmia, eyelid swelling, and pain in both eyes. He had no relevant medical history, and syringing revealed no abnormalities. However, an irregularly marginated soft tissue mass was found in his ethmoid. This mass extended to the medial walls of the orbit, the sphenoid sinus, and the intra-cranial area on both sides. The radiologist suspected neuroblastoma of the olfactory nerves. Thus, if we had not performed preoperative CT, we may have missed the mass until we encountered it during endonasal DCR (Fig. 4A and 4B).
Case 4
A 47-year-old male patient with epiphora, swelling, and pain in right eye. The CT image in the coronal plane shows severe right ethmoiditis and maxillary sinusitis (Fig. 5).
Discussion
Many studies have used CT to evaluate nasolacrimal drainage system anatomy and it's relation with drainage, because CT imaging is useful in evaluation of periocular pathology with detailed imaging in short scan time [3456]. We performed CT on the 218 patients who complained of tearing symptoms; 125 abnormal findings (57.3%) were detected some of which led to changes in the management and treatment plans. Considering the studies with more than 50 cases, success rate varies from 77% to 99% [14]. In our study, success rate of endonasal DCR was 93.9% which is higher than many previous studies. Even though advancement of surgical methods and surgical instruments has increased success rate of endonasal DCR, there can be many intraoperative and postoperative complications. We suppose that preoperative imaging examination can provide information in assessing and preventing such complications.
To the best of our knowledge, no previous study has evaluated the detailed characteristics of nasolacrimal drainage system within a population of individuals previously diagnosed with NLDO. In this study, many eyes with or without epiphora showed opacity in NLD and there were no difference in the incidence of opacity between patient with or without NLDO (p = 0.362). Previous studies reported that opaque NLDs were detected in large population which suggested that opaque NLD could be normal finding [515]. Loftus et al. [5] also mentioned that statistically there was no relationship between NLD opacification and ipsilateral sinus disease. Loftus et al. [5] reported 72% of NLD opacity and Czyz et al. [4] reported 70% of NLD opacity in normal population. In our study, 81.8% of non-obstructed NLD patients showed NLD opacity and 85.8% of obstructed NLD patients showed NLD opacity which was slightly higher than previous studies. Czyz et al. [4] reported that air was found to be present more fully in the upright-position group as compared with the supine-position group. High rates of opacity in this study may be due to the position of patients in performing CT. Further research is needed on this matter.
In our study, seven patients (3.2%) showed masses in the CT images and had to change treatments. Previously, there were many reports of masses found around orbit and nasal sinuses [17101112 13]. Lee et al. [7] reported a case of lacrimal sac tumor discovered in patients with persistent epiphora following DCR and mentioned usefulness of using CT which made it possible to diagnosis relatively early, and were able to obtain rapid, satisfactory treatment. In addition, Jung et al. [11] reported oncocytic carcinoma in patients with NLDO. A tumor originating from the lacrimal sac is rare, but half of the cases of lacrimal sac tumors are malignant, with a high mortality rate, indicating a need for precaution [16]. The most common presenting signs and symptoms of lacrimal sac neoplasms in adults are epiphora (53%), recurrent dacryocystitis (38%), and/or lacrimal sac mass (36%), which are similar to the symptoms seen in patients with NLDO [6]. Further, tumors originating from around the orbits and paranasal sinuses can cause epiphora. Because recent DCRs are performed using sinus endoscopes, it is more difficult to find tumors in these cases than when conventional DCRs are performed. Thus, knowing the exact state of nearby structures of the lacrimal drainage system is important and CT is useful to rule out secondary cause of NLDO and planning for surgical intervention.
Since endonasal DCR is widely used, it is important to examine the nasal cavity in order to inspect the turbinates, and to exclude nasal pathologic characteristics that could adversely affect the surgical outcomes. In addition, having enough space for surgery is important to obtain good surgical outcomes. For that reason, the 26 patients who showed septal deviation were referred to ear, nose, and throat specialists, and 18 patients who showed severe septal deviation underwent septoplasty before DCR. The eight patients with mild septal deviation underwent DCR without septoplasty.
Preoperative inflammation is an important factor affecting surgical outcomes and complication rates. Shams and Selva [17] mentioned that CRS may be a risk factor for the development of postoperative acute rhinosinusitis. Our study had 71 patients with presurgical inflammation, 39 with CRS and 32 with periocular inflammation, including periocular cellulitis and dacryocystitis. Three patients were referred to a tertiary hospital because of severe inflammation that required urgent systemic antibiotics, or because they had concurrent systemic disease (Fig. 5). Other patients, with only mild inflammation, did undergo surgery, but received preoperative and postoperative antibiotics. Patients with pus in lacrimal sac were further examined with bacterial and fungus culture. Also patients with inflammation were checked more often at outpatient clinic after endonasal DCR. In our study, acute postoperative rhinosinusitis was found in two patients (6.9%) who had a history of CRS but no symptom at the time of surgery; this occurrence rate was slightly higher than that reported by Shams and Selva [17]. Considering all cases of DCR, occurrence rate was 2.0% and it is similar to the previous reports [1819]. CT of the paranasal sinuses should be obtained in evaluating patients with CRS or recurrent acute rhinosinusitis because it offers an objective method for monitoring recurrent or chronic disease [2021].
By detecting the aforementioned abnormalities using CT, we could provide proper care and management for our patients. The patients with abnormal CT finding received treatments tailored to their needs. In addition, 37 patients needed consultation for other departments, and subsequently had radical changes in both management and treatment.
The cause of acquired lacrimal drainage obstruction may be primary or secondary. Primary acquired NLDO results from inflammation of unknown origin, but secondary acquired NLDO may results from a wide variety of causes like infection, trauma, inflammation, and neoplasm. CT as a diagnostic tool offers many advantages. It allows surgeons to more effectively and safely plan surgical treatment, especially in the presence of fractures, tumors, nasal sinus abnormalities, or other inflammations near the lacrimal drainage system. Although more proximal obstructions may be difficult to view, CT is regarded as a safe, efficient means to assist in the diagnosis of paranasal sinus pathology. Moreover, it provides patients with detailed diagnoses and prognoses, and helps them make informed treatment decisions. Finally, it can help determine if there are other, treatable causes of patients' NLDOs. Due to preoperative CT, we could prevent surprises and complications which could happen during or after DCR. Also by using prophylactic antibiotics and frequent follow-up of patients with inflammation which were detected by CT, there were only two of 218 outbreaks of acute postoperative rhinosinusitis.
Thus, preoperative CT imaging is a useful assessment tool of nasolacrimal drainage and nearby anatomical structures especially if patients have previous history of CRS or suspicious of secondary NLDO. This information will be helpful in creating plans of NLDO treatment and management.







 XML Download
XML Download