

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The identification of significant refractive errors in children remains a diagnostic dilemma among ophthalmologists. Detection and correction of refractive errors in children is very important for preventing irreversible vision loss secondary to suppression of a blurred or unfocused retinal images (amblyopia), and to eliminate any visual impairment which is harmful to the child's normal functioning in daily life [1]. Amblyopia is the most frequent visual disorder in children that can lead to permanent visual reduction, and it can be prevented if children at risk receive optical correction before maturation of the visual pathways during the 5th and 6th years of life [2,3,4]. Thus, it may be valuable to identify and correct high refractive errors as early as possible. However, even for an experienced ophthalmologist, assessment of refractive errors in the pediatric population can be challenging [5]. There has been an effort to develop tools that can be used easily in busy clinics and provide a 'gold standard' for retinoscopy measurements [5]. Handheld autorefractors have become more important in recent years because of an increasing trust by patients in sophisticated mechanical devices [5].
The present study was undertaken to compare the sensitivity for refractive errors between cycloplegic retinoscopy (CR), a table-top autorefractometer, and a handheld autorefractometer in a pediatric population under 12 years old, and to investigate the possible effect of cycloplegia on such measurements. Another purpose was to investigate whether the refractometer method meets the needs for cycloplegia in the measurement of refractive errors.
Materials and Methods
Sequential patients visiting the outpatient ophthalmology clinic of a state hospital between January and May 2014 were asked to participate. Written informed consent was obtained from all parents or care givers. Ethics committee approval was granted for the study. A total of 112 eyes of 112 patients (comprising 56 boys and 56 girls) aged 2 to 12 years (mean ± standard deviation [SD], 6.78 ± 2.61) who were scheduled to have a comprehensive orthoptic and ophthalmic examination with CR were included.
The main criterion for patient exclusion was the presence of a systemic disease or additional ocular pathology other than a refractive error. Patients who had diseases that could affect ophthalmic measurements such as corneal diseases, pterygium, cataracts, vitreous opacities, retinal diseases, strabismus or nystagmus; those who had eccentric fixation; and those unwilling to participate were not included in the study. Any patient who had a prior eye operation for any reason or who were not compliant during the measurements were also excluded from the study.
Detailed eye examination involving the anterior and posterior segment, cover test, and central fixation examination was performed on each patient. In addition, the refractive errors of all the eyes were measured without cycloplegia using a Canon RK-F1 (Canon USA Inc., Lake Success, NY, USA), Retinomax K-plus 3 (Righton, Tokyo, Japan), respectively. One drop of 1% cyclopentolate (Sikloplejin; Abdi Ibrahim, Istanbul, Turkey) was instilled into both eyes of each patient. The application of 1% cyclopentolate was repeated 5 minutes later. The presence of light activation was checked in the pupillae of the patients 45 minutes after the last drop. No pupillary activity was observed in any of the patients. Measurements were repeated using two refractokeratometers. When cycloplegia was complete, streak retinoscopy was performed in all subjects by one examiner using handheld corrective lenses. The investigator was blinded to the patient's prior refractive history and the results found with the handheld and tabletop autorefractokeratometers.
Refraction measurements with each device were performed by two investigators, and retinoscopy was performed by another investigator. All of the measurements were repeated at least three times and the average values of the obtained results were recorded in order to be used in the study.
The measurements generated in the study were categorized into two groups, noncycloplegic and cycloplegic. The spherical, cylindrical, cylindrical axis, spherical equivalent (SE), and radius of corneal curvature (R1, R2) values obtained in both groups using both of the devices and CR were statistically compared. The following formulas were used for the calculation of the SE in diopters (D) and axis values [6]:
SE (D) = sphere (D) + [cylinder (D)/2]
Jackson cross-cylinder at axis 0° (J0) = (-[cylinder (D)/2] cos[2 X axis])
Jackson cross-cylinder at axis 45° (J45) = (-[cylinder (D)/2] sin[2 X axis])
Handheld automated refraction (Retinomax K-plus 3)
The automated refraction measurement was carried out with the Retinomax K-Plus 3 at a distance of about 5 cm from the patient. The Retinomax is an autorefractor and keratometer that measures the refractive status and keratometry monocularly, and uses a fogging mechanism to control accommodation. It provides up to eight measured values and gives a single representative reading for each eye. It has a measurement range of -18 to +22 D for spheres and 12 D for cylinders.
Tabletop RK-F1
For measurements with the Canon RK-F1, the forehead of the patients was placed onto the forehead part of the device. The RK-F1 autorefractometer detects light reflected from the patient's fundus to which infrared rays are directed. A microcomputer within the machine deduces the objective refraction in terms of sphere, cylinder, and axis, and then automatically displays this information corrected for a 12 mm vertex distance. It completes its objective final measurement in only 1 to 10 seconds. The machine can measure a sphere from -30 to +20 D and a cylinder of 10 D.
Statistical analysis
The descriptive statistics are reported as a mean, SD, and minimum and maximum for continuous data; the number of cases and percentages were used for nominal variables. Regarding the clinical measurements, reliability among Canon, Retinomax devices, and CR was evaluated by Bland-Altman analysis. This method uses graphing to assess whether there is agreement between two measurements. In the current study, agreement between the mean measurements of clinical parameters obtained by the two devices was evaluated. Graphs of the differences between measurements obtained by each measurement against means were plotted (Bland-Altman plots). The limits of agreement were calculated as the mean difference in measurements obtained by each observation ±1.96 X SD of the differences. Bland-Altman plots were performed by using MedCalc (demo ver. 11.1.1.0; MedCalc software, Broekstraat 52, B-9030 Mariakerke, Belgium).
Results
Data were collected from 120 children. Eight patients were excluded due to visually significant media opacities (3), no parental consent (3), and withdrawal of parental consent (2). The mean age of the study participants was 6.78 ± 2.61 years (range, 2 to 12 years).
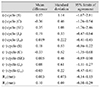
The mean spherical equivalent as measured by the Retinomax K-plus 3 and Canon RK-F1 without cycloplegia was 0.06 ± 2.54 and 0.41 ± 2.20 D, respectively. The mean spherical equivalent as measured after cycloplegia by Retinomax K-plus 3, Canon RK-F1 and CR was 1.57 ± 2.48, 1.57 ± 2.55, and 1.73 ± 2.64 D, respectively. The mean SE obtained from the Retinomax K-plus 3 (0.06 D) was significantly less hyperopic than that from the Canon RK-F1 (0.41 D) (p = 0.004) before cycloplegia, while no significant difference was noted after cycloplegia (Table 1). There were statistically significant differences between the cycloplegic and noncycloplegic spherical powers and the spherical equivalent values determined by each device. However, the response to cycloplegia was not significant for the cylindrical and keratometer values. The J0 and J45 for each device was not significantly affected by cycloplegia.
The 95% limits of agreement for the SE without cycloplegia between the Retinomax K-plus 3 and Canon RK-F1 was larger (range, -1.76 to 2.46 D) than for the SE with cycloplegia (range, -0.89 to 0.90 D). The 95% limits of agreement for the cylindirical power without cycloplegia between the Retinomax K-plus 3 and Canon RK-F1 was larger (range, -1.67 to 2.81 D) than for the cylindrical power with cycloplegia (range, -0.86 to 1.22 D). Good agreement was found between the Retinomax K-plus 3 and Canon RK-F1 with a mean difference of 0.19 ± 0.33 and 0.019 ± 0.222 for J0 and J45 without cycloplegia, respectively. The 95% limits of agreement without cycloplegia between the Retinomax K-plus 3 and Canon RK-F1 for the J0 was smaller (range, -0.47 to 0.84 D) than for the J0 with cycloplegia (range, -1.11 to 1.27 D); for the J45 it was similar (range, -0.41 to 0.45 D) to the J45 with cycloplegia (range, -0.47 to 0.41 D). Good agreement was found between the Retinomax K-plus 3 and Canon RK-F1 with a mean difference of 0.003 ± 0.073 D and 0.01 ± 0.09 D for R1 and R2 without cycloplegia, respectively (Table 1).
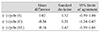
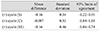
The mean difference between the Canon RK-F1 with cycloplegia and CR was 0.02 ± 0.52 D for the spherical power, -0.34 ± 0.51 D for the cylinder, and -0.16 ± 0.42 D for the spherical equivalent (Table 2). Good agreement was found between the Retinomax K-plus 3 with cycloplegia and CR with a mean difference of -0.16 ± 0.54, -0.007 ± 0.53, and -0.16 ± 0.46 D for the spherical power, the spherical equivalent and the cylindirical power, respectively (Table 3). For the spherical equivalent, the 95% limit of agreement was comparable between the Canon RK-F1 with cycloplegia and CR (-0.99 to 0.68), and the Retinomax K-plus 3 with cycloplegia and CR (-1.06 to 0.74).
When the Bland-Altman analysis was performed to compare spherical equivalent values before and after cycloplegia measured with the Retinomax K-plus 3, the Canon RK-F1 and CR, almost all of the differences between the measurements remained within the range of ±2 SD, on average. Also this analysis was used to compare J0 and J45 values before and after cycloplegia measured with the Retinomax K-plus 3 and Canon RK-F1, and almost all of the differences between the measurements also remained within the range of ±2 SD, on average. A comparison of R1 and R2 values measured with the Retinomax K-plus 3 and Canon RK-F1 revealed that almost all of the differences between the measurements remained within the range of ±2 SD on average.
Discussion
In the current study, the difference between three refraction methods was assessed in children, which will provide insight into the reliability of autorefractor measurements and contribute to the limited amount of information available on the performance of the Retinomax K plus 3. In this study, all measurements were done by three different examiners to decrease potential bias. A potentially weak point of studies investigating both eyes of subjects is a possible intercorrelation of both eyes, since refraction is often similar in both eyes. Only one eye of the subjects was analyzed to avoid this statistical problem. Also, the current study differs from other studies by comparing R1 and R2 values in conjunction with refractive measurements.
It has been stated that accommodation has a prominent effect on refraction in younger children [2,3]. Each of the various available methods, including autorefractors, used to screen children for amblyogenic factors have advantages and disadvantages [7,8,9,10]. There is no consensus as to which method is the most likely to detect children at risk for vision loss from amblyogenic factors. The development of new technology will certainly improve the sensitivity and specificity of autorefraction and other screening techniques. Various autorefractor models, including the Retinomax, have been studied and their reliability and validity has been reported in the literature [8,9,10]. The Retinomax has been studied in pediatric subjects owing to its potential usefulness in screening because of its portability [8].
The Retinomax autorefractor is a monocular refractor that uses a fogging technique. In several studies, this autorefractor was found to be a reliable instrument compared with other autorefractors and retinoscopy [11,12,13]. Being a handheld, easy to use device, it was also tested for early screening of refractive errors in infants, in a preschool population at risk, and preschool children [14].
In the present study, the Retinomax "quick" measuring mode was not used because fluctuations of the spherical component could be judged much better in the "normal" measuring mode. This mode displayed up to eight valid measurements collected consecutively, and this gave a better endpoint for completing the refractive assessment. In the "quick" measuring mode, there would not have been an objective estimate of the technical quality of the refractive measurement. On the other hand, some reports suggest using the "quick" measuring mode of the Retinomax autorefractor for refractive screening especially for the preschool ages [5,15].
This study evaluated the accuracy of the autorefractors by comparing them with CR. Good agreement was found between the Canon RK-F1 with cycloplegia and CR with a mean difference of 0.02 ± 0.52, -0.34 ± 0.51, and -0.16 ± 0.42 D for the spherical power, SE, and the cylindirical power, respectively. The cylindrical power and SE after cycloplegia measured with the Retinomax K-plus 3 was 0.007 ± 0.53 and 0.16 ± 0.46 units, respectively, which was lower than the measurement with CR. However, good agreement was found between the Retinomax K-plus 3 and CR. Retinoscopy has been used as the most accurate technique for determining refractive status [16]. However, some studies have shown that retinoscopy measurements are not an appropriate 'gold standard' for evaluating measurements of refractive error. Harvey et al. [17] showed that the reproducibility of CR was lower than that of autorefraction with the Retinomax K1 in 36 preschool children. Although skilled retinoscopists can provide reliable and valid measures of refractive error in children, retinoscopy might be subject to interobserver variation.
The performance of the Retinomax has been reviewed often, but only a few studies have made a comparison with CR. Harvey et al. [17] reported that the Retinomax provided an average of approximately 0.25 D less negative or more positive measures of refractive error than retinoscopy. They also compared their data to other reports and found that the Retinomax is concordant with retinoscopy and subjective refinement in young children to a degree that is comparable with other autorefractors (Humphrey and Nidek). Wesemann and Dick [12] also showed that the measurement accuracy of the handheld autorefractor in children is high under cycloplegia. In contrast, Prabakaran et al. [18] showed that the SE from the handheld autorefractor was significantly more minus compared to that of streak retinoscopy. Moreover, the autorefractor significantly overestimated the amount of astigmatism. The current study found a good agreement between the Retinomax K-plus 3 after cycloplegia and CR.
A comparison between autorefractors in the current study showed good correlation between the handheld Retinomax K plus 3 and the table-mounted Canon RK-F1 autorefractor for SE and cylindirical power (Table 1). These findings are consistent with other studies involving cyclopleged children and young adults where little difference was noted in spherical, cylinder, or axis measurements between the Retinomax and table mounted autorefractors [12,19].
Variability in the measurements may also occur given the inconsistency of co-operation, alignment, and fixation in these very young children. Interestingly, in our study, although good agreement was found between the Canon RK-F1, Retinomax K-plus 3 and CR for the spherical power, the spherical equivalent, and the cylindirical power, there was a wide spread of SE and astigmatism differences ranging from -1.06 to 0.74 D for SE, and from -1.34 to +1.03 D for astigmatism (Tables 2 and 3). This supports the argument that autorefractors, although useful as a guide and screening tool, may not be accurate enough for determining which children require spectacle prescriptions. Also in a study comparing the spherical equivalent of autorefraction to subjective refraction, the difference was less than or equal to ±0.50 D between 70% and 74% of the time [20].
Non-cycloplegic screening offers advantages since it increases compliance and participation rates, is more rapid, and avoids the side effects associated with cycloplegia. Some authors found the Retinomax useful for noncycloplegic screening for refractive errors [15]. In the present study, cycloplegia decreased the tendency for autorefractors to overestimate myopia, and achieved results more closely resembling the values determined by CR (Tables 1 and 2). It is well understood that autorefraction in a noncyclopleged state may result in the overdiagnosis and treatment of myopia, with the measurements being prone to greater variability [16,19,21]. However, with cycloplegia, the variation seen with autorefraction measurements diminishes to a clinically insignificant level. It is therefore recommended that automatic refractors like the Canon RK-F1 be used with great caution when determining manifest refractions, especially in younger patients in whom accommodation is more active than in older patients, because significant instrument myopia may be induced by the device or real hyperopia may be missed. A cycloplegic refraction in these eyes would afford accurate baseline refractive data as a guideline for clinical prescription.
In the current study the accuracy of the handheld autorefractor is comparable to a conventional tabletop autorefractor in agreement with previous studies [10,22]. As it is also applicable in some problematic cases such as small children on whom objective refraction data can not be obtained with ordinary autorefractors, it seems to be a valuable addition to the existing set of ophthalmic refraction devices. In a different study, the handheld autorefractor Retinomax was comparable to photoscreening as a screening device. The experiences of the authors from that study with non-cycloplegic screening of preschool children for refractive anomalies indicated definite usefulness and reasonable accuracy of the Retinomax for detecting myopia, astigmatism, and hyperopia [15].
The present study also demonstrated good agreement for R1 and R2 values between the Retinomax K-plus 3 and Canon RK-F1. The results of this study indicated that the retinomax K-plus 3 is suitable for use in the study of astigmatism in early childhood.
This study contributes to the limited amount of information available on the performance of the Retinomax K-plus 3. Before introducing the Retinomax K-plus 3 as an accurate screener, it is important to be aware of its possible uses and limitations.
Over the past few decades, autorefraction has become an important part of routine eye care and clinical trials [19,20]. The Retinomax K-plus 3 has the added benefit of mobility and conforming to subject positioning, rather than requiring that a subject be positioned on a chin-rest, which is difficult for some very young children. The Retinomax K-plus 3 appears to be an appropriate and convenient instrument to use for pediatric vision screening. It may also still serve as an alternative tool for use in large-scale refraction studies involving very young children.
 XML Download
XML Download