

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Scleral buckling (SB) has been considered the standard of care for rhegmatogenous retinal detachment (RRD). Use of vitrectomy has historically been limited to complicated retinal detachment cases [1], including those with vitreous hemorrhage, posteriorly located retinal breaks, giant retinal tears and severe proliferative vitreoretinopathy. Although vitrectomy was frequently performed with SB, previous studies showed vitrectomy alone was as effective as vitrectomy with SB [2,3]. Growing evidence has expanded the indication for vitrectomy in RRD, such as in uncomplicated RRD without proliferative vitreoretinopathy or giant retinal tears [4,5].
A few randomized clinical trials have attempted to compare the outcomes of vitrectomy and SB in RRD in order to provide guidelines regarding indications for each technique [6,7,8]. Grey areas, however, still remain, necessitating a surgeon's judgment. The decision of which surgical technique to use depends on a variety of factors, including the location and number of retinal breaks, lens status, the patient's compliance and the surgeon's preference. Surveys have been used to study vitreoretinal surgeons' RRD surgery preferences [9,10]. Vitrectomy, however, was not included as an option in previous studies, because the primary objective of these studies was to evaluate the popularity of PR.
We assumed that recent improvements in instruments and sutureless vitrectomy would increase a surgeon's preference for vitrectomy in primary RRD repairs. We conducted a survey of the preferences for primary RRD surgery among Korean vitreoretinal specialists in 2001 and reported our results then [11]. In this current study, we re-surveyed the practice patterns of vitreoretinal specialists for the repair of RRD in Korea in 2013, and analyzed changing trends in RRD surgery by comparing the results from the two surveys.
Materials and Methods
Survey
In 2013, a survey was conducted among the 219 members of Korean Retina Society via e-mail and post containing the same two scenarios and six questions as the previous survey that was administered in 2001 [11]. The primary scenario was adopted from studies performed in 1990 and 1997 in the USA [9,10].
1) The primary scenario
You are a 48-year-old ophthalmologist with a visual acuity of 20 / 20 in both eyes, emmetropia, and no known systemic or ophthalmic diseases. Localized RRD in your right eye developed with two small horseshoe tears at 11:30, and the macula was on, without signs of proliferative vitreoretinopathy (Fig. 1A).
Question 1: The first question asked was "What kind of surgical method would you like to have performed on you?" To further specify the preferences of surgical method, the following clinical variables were added to the primary scenario. Question 2: In addition to the primary scenario, what if there is lattice degeneration, combined with a horseshoe tear at 6 o'clock, in an attached retina, and a family history of rhegmatogenous retinal detachment? Question 3: In addition to the primary scenario, what if there is a mild vitreous hemorrhage, and decreased visual acuity of 20 / 50? Question 4: In addition to the primary scenario, what if your refraction is -3.00 sphere in both eyes? Question 5: In addition to the primary scenario, what if you underwent a successful SB procedure in the other eye 15 years prior?
2) The second scenario
The second scenario was a case of pseudophakic RRD that developed two weeks prior in a 61-year-old woman who presented with decreased vision in her right eye. Her best corrected visual acuity was counting fingers in the right eye, and 20 / 20 in the left. On the ophthalmic exam, her right eye was pseudophakic, and there was total retinal detachment with lattice degeneration, accompanied by a horseshoe tear, and a retinal hole near 11:30. The inferior fundus was partially obscured by posterior capsular opacity (Fig. 1B). The following question was presented: what kind of surgical method would you choose if this patient came to your clinic? (question 6).
Throughout these questionnaires, respondents were asked to choose one treatment among SB, PR, vitrectomy, or other, and were allowed to write specific procedures when they selected 'other.'
Also, we asked the surgeon's years since vitreoretinal fellowship and his or her average percentage of patients with vitreoretinal disease in their clinic. With these data, career index was obtained for each respondent. Career index was defined as years after fellowship multiplied by average percentage of patients with vitreoretinal diseases in their clinic, which was divided by 100. There were 27 members who participated in the surveys for both 2001 and 2013. Subgroup analysis was performed to evaluate changes in their answers to the questionnaires over the 12-year period.
Statistical analysis
All the procedures were categorized into four surgical methods: SB, pneumatic retinopexy (PR), vitrectomy, and the combination method (Combi), which is a combination of SB or encircling and vitrectomy. For example, SB with cryotherapy or laser treatment was regarded as SB, and vitrectomy with silicone oil or gas injection as vitrectomy. The chi-square test and Fisher's exact test, with a permutation method for multiple comparisons, were used to analyze the shift in the proportion of surgical procedures used between 2001 and 2013. The respondents were divided into younger/older generation and inexperienced/experienced surgeons by median years post fellowship and median value of career index, respectively. Then, their answers for each question were compared. Asymptotic marginal-homogeneity tests were used to analyze changes in responses in the subgroups of respondents who participated in both surveys.
Results
Out of a total of 219 investigators who received the questionnaire, 133 (60.7%) members responded, compared with 46 (79.3%) in 2001. Mean years since fellowship was longer in 2013 (mean ± standard deviation, 12.9 ± 8.3) than in 2001 (10.0 ± 7.0, p = 0.024). The proportion (%) of patients with vitreoretinal disease was similar between both surveys (78.9 ± 2.4 in 2001 vs. 79 ± 2.2 in 2013, p = 0.973). There was no significant difference in career index between the two surveys (8.3 ± 6.9 in 2001 vs. 10.3 ± 7.7 in 2013, p = 0.091).
For the primary scenario, 74.4% chose SB, 15.8% chose PR and 9.8% chose vitrectomy in 2013. In the analysis of the proportional change of each technique between the 2001 and 2013 surveys, the proportion of PR decreased significantly (34.8% in 2001 vs. 15.8% in 2013), compared to the proportional change of SB (p = 0.043) and vitrectomy (p = 0.006) (Table 1 and Fig. 2A). The majority of respondents selected SB both in 2001 (84.8%) and 2013 (75.9%) when taking into account a family history of retinal detachment and lattice degeneration, accompanied by a horseshoe tear in an attached retina. Significant changes in techniques falling under the 'other' category were not detected between the results of 2001 and 2013 (Table 1 and Fig. 2B). The addition of a mild vitreous hemorrhage, however, with decreased visual acuity to the level of 20 / 50, changed the preference of surgical method significantly (Table 1 and Fig. 2C). Preference for SB was decreased from 76.1% to 46.6%, and that for vitrectomy increased from 17.4% to 45.1%. The proportional change between these two methods was significant (p = 0.001). SB was consistently the most preferred surgical method in both 2001 and 2013, when a history of myopia or successful SB on the fellow eye was considered (Table 1, Fig. 2D and 2E). Preference for vitrectomy over SB, however, increased with the presence of myopia (p = 0.044) and PR (p = 0.024). The popularity of vitrectomy compared to PR increased significantly when factoring in a history of successful SB (p = 0.044).
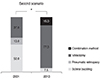
In 2001, 50.0% preferred SB, 37.0% preferred vitrectomy, and 13.0% preferred PR for the second scenario. These results changed drastically in 2013 (Table 1 and Fig. 3): 77.4% selected vitrectomy and 15.1% selected Combi as the choice of treatment, while only 7.5% preferred SB and no one chose PR. A proportionate increase in vitrectomy (p < 0.001) and Combi (p = 0.001), compared to SB, was statistically significant.
The career index ranged from 0.75 to 40 among the 2013 participants. For the analysis, participants were divided into two groups by the median value (8.0) of career index. Those with a career index less than or equal to 8.0 (less experienced group, n = 67) and those with a career index greater than the median (experienced group, n = 66) did not show significant differences in their choice of treatment to all six questions (Table 2). Also, when they were divided into two groups (younger group, n = 67 vs. older group, n = 66) by the median years after fellowship, their surgical method preferences still did not differ significantly.
Twenty-seven members replied to the same questionnaire in both 2001 and 2013. Changes in their answers for each question were analyzed using the year of survey as the variable. The 27 members had significant changes to their preferences for questions 2, 3 and 6 (Table 3). In 2013, they favored vitrectomy more often (questions 2, 3, and 6) and showed a decreased preference for SB (questions 3 and 6), and for PR (question 6), compared to 2001. Specifically, for question 6, total RRD with pseudophakia, 13 members selected SB in 2001, but in 2013, eight of them changed their choice to vitrectomy, one to Combi, and only four members adhered to SB. Likewise, all of the 11 members who selected PR in 2001 changed their choice to vitrectomy.
Discussion
In this study, we investigated the changing trends in managing primary RRD in Korea, using two surveys with identical questionnaires administered about a decade apart. In 2013, more members of Korean Retina Society selected vitrectomy for treating primary RRD with the presence of myopia, mild vitreous hemorrhage and a history of successful SB on the other eye, compared to 2001. Furthermore, significant intra-respondent change was also found among the 27 members who participated in both surveys. The popularity of PR has noticeably decreased. The most prominent and significant change was that most members in 2013 chose primary vitrectomy in the second scenario, which involved a pseudophakic, macula-off RRD case with media opacity, whereas in 2001, the majority chose SB in the same case.
This study demonstrated the growing trend toward vitrectomy as the preferred primary surgical method for primary RRD. Previous studies conducted in other countries have also suggested the increasing popularity of vitrectomy [12,13]. Minihan et al. [12] retrospectively compared RRD surgeries, performed 20 years apart, in a single center located in London, UK. They reported that 63% of patients with primary RRD were treated by vitrectomy in 1999; in contrast, only one case was managed by vitrectomy in 1979 and 1980. As there were extremely few cases in 1979 and 1980, a comparison of surgeries selected for RRD, with different clinical complexities, was not possible. Another study was a bi-center study that retrospectively investigated RRD surgeries performed in 2007 and 2008 in Vienna, Austria and New York, USA [13]. Although the authors attempted to assess the influence of Scleral Buckling versus Primary Vitrectomy in Rhegmatogenous Retinal Detachment study findings [6], the study period of only two years was not long enough to evaluate changes in general trends.
Recent mechanical and technical advances, such as sutureless small gauge vitrectomy with high cutting rates, wide-angle viewing systems, and the introduction of perfluorocarbon liquid have provided better views, easy removal of media opacity and intraoperative retinal reattachment with fewer complications, compared to techniques of the past decade. Also, under the current training system, retinal surgeons are given more exposure to, and are consequently more comfortable with vitrectomy than SB, as the indications for vitrectomy have been expanded to include various vitreoretinal diseases other than RRD, such as diabetic retinopathy and epiretinal membrane, whereas SB is limited to RRD cases.
Especially in cases of RRD with pseudophakia, vitrectomy was twice as popular. For question 6, 77.5% of respondents selected vitrectomy in 2013. When combined with the 15% that chose the Combi, a total of 92.5% answered that they would perform vitrectomy as the primary surgery. Since the first survey was conducted in 2001, several studies supporting vitrectomy as the primary treatment modality in pseudophakic RRD have been reported [6,7,8]. A multicenter randomized study by Heimann et al. [6] compared the results of SB and vitrectomy in primary RRD. Their results indicated that SB resulted in better visual outcomes than vitrectomy in phakic RRD; however, vitrectomy achieved a superior anatomical success rate and similar final visual acuity in pseudophakic/aphakic RRD. This evidence may have influenced the preference for vitrectomy in the case of pseudophakic RRD noted in the current survey.
Popularity of PR decreased in most cases, including in the case of uncomplicated primary RRD that was traditionally regarded as a good indication [14,15]. Although PR has advantages over vitrectomy and SB, such as a short duration of operation, cost-effectiveness and availability as an outpatient-based procedure, disadvantages of this procedure are that it necessitates a second retinopexy procedure, such as laser photocoagulation, and requires maintaining the correct position after the procedure for at least several days. Moreover, missed or new breaks [16], limited indication [17] and higher probability of needing a second operation [18], decreased its popularity.
Besides the reasons described above, the increase of vitrectomy and decrease of PR may also be attributable to the national health care system called the National Health Insurance Program of South Korea. This system offers universal coverage for all citizens in South Korea, and health care providers are reimbursed on a fee-for-service basis. In tertiary hospitals of South Korea, the fee for vitrectomy is approximately double that for SB and quintuple for PR. Therefore, the possibility that this payment system may affect surgeons' decisions regarding surgical method cannot be excluded. Nonetheless questions regarding the primary scenario were based on the assumption that, "if RRD happened on your eye..." so that respondents would answer based on their medical and scientific background solely, and ignore economic incentives.
This study has several limitations. First, there was a selection bias of respondents, because 20.7% and 39.3% of members did not reply to the survey in 2001 and 2013, respectively. In addition, the cases presented for the first scenario were either primary uncomplicated RRD or RRD combined with only a few clinical variables; however, in a real clinical situation, surgeons commonly encounter combinations of multiple clinical variables in an eye with RRD. Finally, the preference of contemporary colleagues does not provide any evidence supporting one specific surgical modality over the other, and must be interpreted cautiously.
In conclusion, preference for vitrectomy in primary RRD has increased drastically among the members of the Korean Retina Society, especially when combined with myopia, media opacity and pseudophakia, over the course of the last decade.





 XML Download
XML Download