

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Myopathic ptosis can occur in some muscle diseases such as mitochondrial myopathies, oculopharyngeal muscular dystrophy, oculopharyngodistal myopathy or myotonic dystrophy [1,2,3,4] (Fig. 1). Patients with myopathic ptosis have common clinical characteristics. Levator function is low. Muscular weakness may be present in extraocular muscles and any other muscle group in the body [5]. Management of myopathic ptosis is challenging due to weak Bell's phenomenon and risk of postoperative lagophthalmos [5], although the efficacy of frontalis suspension surgery has been reported in some studies [1,6,7]. In this study, we report the results of levator resection in patients with myopathic ptosis and discuss the effect of levator function and Bell's phenomenon on success and corneal complication rates.
Materials and Methods
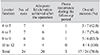
The medical records of consecutive patients who underwent levator resection surgery performed for myopathic ptosis between October 2009 and March 2013 were reviewed. Indications for surgery were ptosis obscuring the visual axis and margin-reflex distance (MRD) ≤2 mm. All patients had myopathic disease confirmed by the neurology clinic, and other possible causes of ptosis were excluded. Patients were informed about the potential risks and complications of the surgery. Cases with a history of previous lid surgery, and those with follow-up of fewer than six months were excluded from the study. In all patients, levator muscle function was measured, and Bell's phenomenon was graded (Table 1).
Surgeries were performed under local anesthesia. A skin crease incision was created in the upper lid to expose the tarsal plate. A dissection between the orbicularis muscle and septum was performed, and a transverse incision was made to open the septum. Preaponeurotic fat pad was retracted. The levator muscle was exposed, and the levator and Müller's muscle were detached together from the underlying conjunctiva as far as possible until the retractor complex was moderately free. A 6-0 polyglactin suture was placed in the center of the retractor complex and attached to the tarsal plate with a temporary knot to adjust the height of the lid. The goal was to achieve a lid level just high enough to leave the pupillary axis clear without compromising corneal closure. After a satisfactory level was achieved, a medial and a lateral suture were placed. Finally, the skin crease was formed, and the skin closed with 6-0 polyglactin sutures. Antibiotic ointments were prescribed for the surgical wound, and artificial tear ointments and eye drops for the prevention of exposure keratopathy after surgery. Antibiotic ointment was tapered after one week, and artificial eye drops and ointments were tapered if there was no finding of corneal exposure. Follow-up visits were scheduled on the first day, first week, second week, first month, and monthly for the first year, and yearly thereafter. All patients were instructed to come to the clinic if the eye became red or painful, or if visual acuity decreased. Surgical success was defined as clear pupillary axis when the patient voluntarily opened his eye and MRD ≥3 mm. We analyzed the effect of levator function and Bell's phenomenon on the rates of success and corneal complication. Tenets of Helsinki were followed in the study and all patients gave informed consent.
Results
This series included six male and six female patients. The mean age of the patients was 38.6 years (range, 27 to 68 years). All patients had bilateral myopathic ptosis and levator function between 4 and 12 mm. We performed bilateral levator resection surgery in all patients. Fat infiltration of levator muscle was observed in most of the patients (Fig. 2). The mean follow-up time was 14.8 months (range, 6 to 36 months). No patient was overcorrected. Adequate lid elevation was achieved after the operation in 20 eyes (Fig. 3). In three patients with 4 to 5 mm levator function and one with 6 to 7 mm levator function, we were unable to achieve a lid level high enough to leave the pupillary axis clear without compromising corneal closure. Ptosis recurred in three out of 20 eyes during the follow-up period after adequate lid elevation had been achieved. Our overall success rate was 70.8% (Table 2). In three eyes with poor Bell's phenomenon, corneal irritation and punctate epitheliopathy that required artificial eye drops and ointments developed in the early postoperative period. Postoperative lagophthalmos decreased with time, and symptoms resolved completely within two months. We did not observe any corneal problem in patients with moderate or good Bell's phenomenon (Table 3). We did not need to perform levator recession or any other revision surgery for lagophthalmos in any of the patients after levator resection. In three eyes for which levator resection was not successful, we performed frontalis suspension surgery using a silicone rod. In one eye with poor Bell's phenomenon, a corneal abscess developed, and we had to remove the silicone rod.
Discussion
Involvement of the levator muscle may lead to ptosis in some myopathic diseases, and myopathic ptosis must be differentiated from desmogenic, aponeurotic, neurogenic, mechanical, and traumatic forms of ptosis [5]. Many organ systems may be involved in myopathic diseases, and some life-threatening complications may occur such as heart block, encephalopathy, lactic acidosis, dysphagia, cardiomyopathy, and weakness in any muscle group [2,3,4]. Diseases leading to myopathic ptosis include a heterogeneous group of disorders, and different genetic mutations and inheritance patterns were reported even for the same diseases [8]. For example, chronic progressive external ophthalmoplegia (CPEO), a mitochondrial myopathy, may be caused by a sporadic single large-scale deletion in mtDNA, by a mtDNA point mutation inherited in matrilineal succession, or by a nuclear gene defect inherited autosomally [8,9]. However, myopathic disorders have some common ophthalmologic clinical features: myopathic ptosis, reduced levator function, ophthalmoplegia, poor Bell's phenomenon, frontalis and orbicularis muscle weakness, and poor lid closure [5]. Therefore, we included all these patients in a "myopathic ptosis" group and reported our experience.
In congenital ptosis surgery, 4 mm levator function is generally accepted as a cut-off point, and levator resection is performed for values greater than 4 mm to achieve an eyelid position 1 or 2 mm below the superior limbus [10,11,12]. However in myopathic ptosis, we only intend to clear the visual axis, and the procedure of choice for the correction of ptosis is controversial. Ahn et al. [1] suggested performing frontalis sling surgery using silicone rod in CPEO. The elasticity of the silicone rod is an advantage for patients with a minimal or absent Bell's phenomenon; however, the orbicularis muscle must be strong enough to overcome the traction force of the silicone rod to allow the lids to be closed. Also frontalis-muscle function is important in elevation of the lid in patients with a silicone rod. In myopathic patients, levator function needed for an effective levator resection surgery is also controversial. Lane and Collin [13] performed levator advancement in patients with levator function greater than 4 mm. However, Wong et al. [5] performed levator resection if a patient's levator function was greater than 7 mm. In our study group, levator function was between 4 and 12 mm. We divided patients into four groups according to levator function, and the success rate was 42.8% in the 4 to 5 mm levator function group; the success rate increased to 100% in the 10 to 12 mm levator function group. Overall success rate was 70.8% in the study group and 82.3% in patients with levator function greater than 5 mm. In three patients with 4 to 5 mm levator function and one with 6 to 7 mm levator function, an increasing amount of levator resection compromised the corneal closure during surgery, so we were unable to achieve a lid level high enough to leave the pupillary axis clear. According to our results, levator resection is effective in myopathic patients, and the success rate of surgery increases in patients with higher levator function.
Myopathic patients are susceptible to corneal exposure keratopathy after ptosis surgery. In our study group three eyes with poor Bell's phenomenon developed corneal irritation and punctate epitheliopathy that required artificial eye drops and ointments in the early postoperative period; symptoms resolved completely within 2 months. We did not notice any corneal problems in patients with moderate and good Bell's phenomenon. One of the three eyes that underwent frontalis suspension surgery using a silicone rod had a corneal abscess, and we had to remove the silicone rod. Wong et al. [5] performed brow suspension or levator advancement with resection in 50 eyes of 25 patients and reported corneal desiccation in four patients, two of whom needed a revision surgery to decrease lagophthalmos. Ahn et al. [1] performed frontalis suspension surgery using a silicone rod in seven CPEO patients and reported keratopathy in five of them. Ptosis surgery carries some risks for corneal exposure in all patients with myopathic ptosis; however, levator resection seems to be a safer procedure, especially in patients with moderate or good Bell's phenomenon.
In our group of patients, adequate lid elevation was achieved after the operation in 20 eyes, and ptosis recurred in three of them during the follow-up period. Rodrigue and Molgat [14] reported a recurrence rate of 13% after a minimum of 9 years of follow-up in oculopharyngeal muscular dystrophy patients after levator resection. Some authors use slings due to the progressive nature of myopathies; however, ptosis recurrence, regardless of the sling material and indication, is the major problem after frontalis suspension surgery, and recurrence rates between 0% and 100% have been reported [15,16]. There is no evidence that demonstrates higher recurrence with levator resection surgery than with frontalis sling surgery. Patients must be informed about the progressive nature of the disease and the probability of recurrence even after a successful surgical result.
Our results suggest that levator resection surgery may be attempted before frontalis sling surgery to decrease postoperative complications in patients with myopathic ptosis and levator function greater than 5 mm.





 XML Download
XML Download