

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Traumatic rupture of an extraocular muscle is rare. Few cases of superior oblique muscle tendon rupture have been reported. Therefore, management modalities are largely anecdotal. We report a case of reattachment of a ruptured superior oblique muscle tendon to sclera to correct initial torsional diplopia.
Case Report
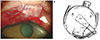
A 54 year-old man was referred to the outpatient clinic having been injured in his right eye by the hook of a clothes hanger while falling. Swelling and bruising on the right eyelid were observed but there were no lacerations. He complained of image tilting in the right eye compared to the image inthe left eye. His corrected visual acuity was 6 / 6 in both eyes. Findings on intraocular examination were unremarkable. Non-dilatating fundusphotos (VX-10; Kowa Optimed, Tokyo, Japan) showed a 12-degree excyclotorsion in the right eye and an 8-degree excyclotorsion in the left eye. Image J (National Institutes of Health, Bethesda, MD, USA) was used to measure the angle between the line that crosses the center of the optic disc and parallels the fovea and the line that extends from the optic disc center to the fovea [1]. Non-enhanced orbit computed tomography was performed to rule out eyeball rupture, intraocular foreign body, or orbit wall fracture as well as any other abnormalities. During surgery, a 15-mm horizontal conjunctival laceration over the superior rectus muscle was found. The tendon of the superior oblique muscle protruded inferio-nasally through the lacerated conjunctiva (Fig. 1A). The cut margin of the ruptured tendon was irregular and the width was about 4 mm. We could not find the distal end of the tendon. It was assumed that the location of the rupture was in the middle of the tendon under the superior rectus muscle. The superior rectus muscle seemed to be intact. To correct torsional diplopia, we attached the anterior and posterior borders of the superior oblique tendon 5 and 9 mm apart from the nasal margin of the superior rectus muscle insertion (Fig. 1B). One week postoperatively, the patient showed vertical diplopia and 4-prism dioptor right hypertropia by the alternative prism and cover test in the primary position. Double Maddox rod testing revealed 2° of excyclotorsion in the right eye. However, the patient did not complain of torsional diplopia. In the fundus photographs, the excyclotorsion of the right eye improved from 12° to 7° (Fig. 2). Underaction of the right superior oblique muscle was not noted. Three months postoperatively, right hypertropia gradually increased to 20-prism diopters and the patient complained of vertical diplopia. A 7 mm resection of the right inferior rectus was performed. Two months postoperatively, the patient remained comfortable and stable.
Discussion
The superior oblique muscle originates in the annulus of Zinn. It loops through the trochlea, and passes under the superior rectus muscle and inserts into the sclera on the posterotemporal surface of the eyeball. Traumatic injury to the superior oblique muscle is extremely rare, and mostly arises from injuries caused by hook-shaped objects, and is frequently associated with penetrating eyelid injury [2,3]. When the ruptured muscle belly from the origin could not be found and was left unconnected, the patient showed a pattern of superior oblique muscle palsy [2]. However, Harish et al. [4] reported that excision of the loose hanging tendon near the medial border of the superior rectus muscle did not result in progressive muscle sequelae until six months later. That might be possible because some of the posterior fibers of the superior oblique tendon were still intact. In our case, the patient initially complained of torsional diplopia, which coincided with the excyclotorsion of the right eye on the fundus photograph. To correct this, we planned to reattach the ruptured tendon to the middle of the original track where the superior oblique muscle might have passed. Dow [5] found that anchoring the avulsed superior oblique muscle to the medial orbital wall adjacent to the trochlea resulted in slight hypertropia with full ocular motility. However, when the ruptured tendons were reapproximated with each other, postoperatively, asymptomatic Brown's syndrome could develop [3]. Because the ruptured superior oblique muscle shortened in our case, we recessed the muscle 5 mm from the medial border of the superior rectus muscle. According to Parks [6] and Helveston [7], the distance between the nasal edge of the superior rectus and anterior border of the superior oblique muscle in the primary position was 3 to 5 mm. The postoperative result was favorable. Torsional diplopia, the main complaint of the patient, improved and the degree of excyclotorsion of the right eye decreased in the fundus photographs. However, three months after the operation, hypertropia increased to 20 prism dioptors. This could have been due to the torn tendon that was not attached far enough laterally to avoid a weakening effect. Additionally, during the exploratory procedure to find the distal remnant of the superior oblique tendon, the superior rectus muscle could have been injured, although initially the superior rectus muscle seemed to be intact. Upon healing, it might have undergone localized fibrosis that caused contraction and secondary hypertropia. To correct the hypertropia, we performed the second operation. An inferior rectus resection was chosen for adhesion around the superior rectus muscle and to avoid contralateral inferior rectus recession. Two months after the second operation, the patient was comfortable and muscle function was stable.
When the superior oblique muscle is ruptured, intraoperative reapproximation of the muscle can be performed. However, because the function of the muscle is hard to restore perfectly, postoperative complications should be anticipated and careful follow-up is needed to determine further treatment.

 XML Download
XML Download