

 PDF
PDF ePub
ePub Citation
Citation Print
Print


In the treatment of congenital cataracts, visual rehabilitation after surgery is as important as the timing of the surgery. To correct postoperative refraction errors, spectacles and contact lenses are available. However, correction with spectacles induces aniseikonia and resultant amblyopia, particularly in severe anisometropic conditions. Moreover, glasses with heavy lenses are associated with optical problems, such as pin cushion effect, peripheral scotoma, and the jack-in-the-box phenomenon. As an alternative solution, contact lenses can provide optical advantages over spectacles. However, the physician should consider certain matters such as the difficulty associated with proper management of contact lenses, limited compliance in younger people, and the increased risk of corneal injury.
Temporary polypseudophakia, initially described by Wilson et al. in 2001 [1], consists of permanent intraocular lens (IOL) implantation in the capsular bag and temporary IOL insertion into the ciliary sulcus in order to achieve emmetropia. The temporary IOL can be removed or exchanged according to subsequent refractive changes. Thus, during the critical period of visual development patients can overcome the adverse effects of thick spectacles or contact lenses, and acquire a constant image similar to that of normal eyes.
When a patient's eye is in need of surgical correction for high myopia after cataract surgery the physician must estimate the refractive change after removal or exchange of the temporary IOL. In this study, we assessed the difference between the expected refractive error and the true manifest refraction after removal of the IOL from the ciliary sulcus.
Materials and Methods
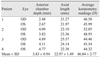
This prospective study included 7 eyes from 4 patients who received temporary IOL removal between June 2008 and February 2009. All patients had undergone cataract extraction and temporary piggyback IOL implantation as infants at the Samsung Medical Center in Seoul, Korea. Data included the power of the implanted IOL, cycloplegic refraction prior to IOL removal, and cycloplegic refraction at 1 month postoperatively. Average keratometry readings, axial length (AXL), and anterior chamber depth (ACD) were measured preoperatively using the IOL Master (Carl Zeiss Meditec, Dublin, CA, USA).
To calculate the predicted change in refraction (PCR) after IOL removal, we used nomograms described by Gills and IOL power calculation formulas including: SRK-II, SRK-T, Hoffer-Q, and Holladay. The Gills' nomograms were modified as shown in Table 1. Although the original Gills' formula for residual myopia is used for the calculation of the negative-diopter IOL which is implanted secondarily, the PCR was calculated using both equations for residual hyperopia and residual myopia, respectively.
The power of the permanent IOL, keratometric reading, A-constant of the IOL, and AXL were used as variables in the IOL power calculation formulas. We then evaluated the prediction error, the difference between the results acquired from each of the formulas, and the actual refractive error after IOL removal.
If the patient could not tolerate wearing glasses and the predicted refraction after anterior IOL explantation was so hyperopic that the eye was could be at risk for amblyopia, we planned to insert a temporary IOL in the interim. However, we encountered no cases requiring IOL exchange. Removal of the temporary IOL was performed when the predicted refraction was plano or mildly myopic. All eye operations were performed under general anesthesia by the same surgeon (ESC). The surgeon fragmented the temporary IOL using an IOL cutter via a 3-mm temporal clear corneal incision after injection of viscoelastic material into the anterior chamber. The pieces were then extracted using lens forceps through the incision; sutures were made with 10-0 nylon at the end of the surgery.
Results
Patients underwent temporary piggyback IOL implantation at a mean age of 6.71 ± 3.68 months (range, 3 to 12 months). All surgeries were performed as soon as possible following diagnosis of the cataract. During the follow-up period, patients experienced a myopic shift from -0.14 ± 2.14 diopters (D; range, -2 to 4 D) initially to -13.11 ± 3.10 D (range, -9.3 to -16.8 D) just prior to removal of the temporary IOL. The temporary IOL was removed at 51.14 ± 18.38 months (range, 29 to 74 months) after piggyback IOL implantation. Among the biometric results shown in Table 2, three ACDs (both eyes of patient 1 and the right eye of patient 3) and one AXL (the right eye of patient 3) fell beyond one standard deviation (SD) from the mean. The mean power of the removed IOLs was 13.5 ± 2.36 D, resulting in 11.18 ± 2.96 D of actual refractive change (Table 3).
We calculated the SD of the prediction error and the mean of the absolute prediction error because prediction errors with opposite signs do not cancel out. As seen in Table 4, the SD and mean absolute prediction error of the SRK-T were smaller than those of the other formulas, but the difference was not statistically significant.
In the case of Gills' formula, the mean for residual myopia showed a better result than that for residual hyperopia. Among the results of the IOL power calculating formulas, the right eye of patient 2, whose keratometry reading was farthest from the mean, had the largest prediction error in the results of each IOL calculating formula. Additionally, the values were at least two to six times greater than those of Gills' formula for myopia. On the other hand, the right eye of patient 1, with a prediction error that fell beyond one SD from the mean, had the shallowest ACD and the largest prediction errors in the results from Gills' formula for residual myopia and hyperopia.
Discussion
As axial myopia after piggyback IOL implantation progresses, the surgeon needs to consider when the temporary IOL should be removed or exchanged. Therefore, exact prediction of refractive error after IOL explantation is mandatory. However, to the best of our knowledge, there is no published data that describes the visual outcomes after temporary IOL removal. Therefore, we performed this study to evaluate the refractive outcomes after temporary IOL removal, and the predictability of several formulas used to calculate refractive change. Although the predictability of SRK-T was the best among the formulas, the modified Gills' formula for myopia had relatively good predictability. This formula in particular yielded more accurate results when the keratometry reading showed an extreme deviation from the mean. This may be due to the fact that Gills' formula is an empiric method of predictive modeling that does not use keratometric readings as a variable. Therefore, this formula can be used if the patient's keratometric reading is unavailable or falls beyond one SD from the mean.
On the other hand, there are some limitations to this formula. First, this formula assumes that the IOL position is fixed according to the AXL. Hence, when the postoperative ACD differs from the mean, this formula does not work well. This was observed in the case of patient 1, in whom the ACD was unusually shallow. As such, a myopic error would be produced in an eye with a shallow ACD and a hyperopic error would be created in an eye with a deep anterior chamber. A 1-mm error of postoperative ACD corresponds to 1.5 D of refractive difference [2,3]. Second, this formula sets no limit on the angle of the haptics or the thickness of the optics. Although it was not proven in this study, posterior-angled haptics and thick optics in an anterior IOL may push the permanent IOL backward. Thus, after removal of the anterior IOL, if the permanent IOL does not move enough anteriorly due to irreversible anatomical changes caused by the temporary IOL, the resultant refraction error may become more hyperopic than expected. This could potentially explain why the mean of the formula for residual myopia is closer to emmetropia than that of the formula for residual hyperopia. Third, there are no references that can be accepted as standard data.
The reasons for inaccuracy in refractive prediction might be due to the limited anterior segment development prior to the first surgery or astigmatism development after the second surgery caused by the corneal incision.
In this study, the IOL power calculation formulas had a mean absolute prediction error ranging from 1.17 to 1.87 D. Significant variability did occur with outcomes ranging from 0.2 to 2.7 D. Compared with several reports on the prediction error after single IOL implantation in children, the accuracy of the IOL calculating formula has been reported as an absolute prediction error between 1 and 2 D with a wide range over 3 D [4-7]. Therefore, the predictability in our series appears similar to that observed in other series for single IOL implantation. However, these formulas were derived from data on an adult eye. It is well known that refractive error predictability in cases of pediatric cataracts is more difficult. There are several potential sources for error in IOL power selection in children. One source is inaccuracy of the AXL and keratometry measurements. A lack of cooperation in children who have biometry measurements not performed under general anesthesia may lead to a greater magnitude in errors of keratometry and AXL, which could lead to a resultant refractive surprise [8,9]. Although the AXL, ACD, and keratometry readings in this study were obtained using the IOL Master, which is a non-contact system that can calculate exact AXL and ACD measurement, the accuracy of this system may decrease in an uncooperative child without precise central fixation [10,11].
The patients in this study were cooperative with multiple preoperative check-ups so it can be assumed that the results from the IOL Master were precise and reliable. However, the predictability of the postoperative refraction was not better than that seen in adults. This is likely the reason that ACD and keratometry readings deviated from the mean in some cases. Another reason is an unexpected change in ACD after removal of the anterior IOL. Using the IOL calculation formulas, it was estimated that the outcome would be closer to myopia rather than the actual refraction after surgery in both eyes of patient 2 and in the right eye of patient 3. After removal of the anterior IOL, the permanent IOL settled in a more posterior position than anticipated by the formulas. Put another way, the permanent IOL either shifted anteriorly less than expected or not at all. There is a possibility that the temporary IOL in the ciliary sulcus affected both the ciliary body and its related anatomical structures in an irreversible manner.
No consensus has been reached regarding either a proper procedure for infantile cataract extraction or a refractive goal after surgery. Even in the auctorial clinic, although aphakic correction or single IOL implantation has been applied after cataract extraction, temporary polypseudophakia has resulted in the best visual outcomes thus far. Furthermore, the frequency of glaucoma, with the greatest risk for potential complications, has been noted to be relatively low. For that reason, we have used this method in most cataract patients under age 2 since 2002. The current study includes the first patient who underwent this procedure and subsequent consecutive cases including the initial IOL removal.
This study is not without limitations. The small number of cases in this study yielded results that can hardly be considered representative. No concrete cause of predictive error has been found, and advanced changes have not been identified in all aspects of the surgery. However, it is meaningful that even without a keratometry reading predictions made using Gill's formula and SRK-T show relatively precise results compared with a variety of IOL calculation formulas.



 XML Download
XML Download