

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Behçet's disease is a systemic immune-mediated vasculitis of unclear origin [1]. Frosted branch angiitis (FBA), first described in 1976 by Ito et al. [2], is a retinal perivasculitis with severe sheathing of all retinal vessels, resembling the frosted branches of a tree [3]. The disease may be idiopathic in a majority of cases or may be associated with ocular and systemic pathology [4]. FBA in association with Behçet's disease is rare and there are only six reported cases of this uncommon combination [5-10]. In this article, an unusual case of unilateral occlusive retinal vasculitis resembling FBA in association with Behçet's disease is reported. In addition, the authors give a literature review of FBA as an ocular manifestation of Behçet's disease with a summary of previously reported cases.
Case Report
A 39-year-old male presented with decreased vision in his left eye for two days. Visual acuity was 20 / 20 in the right eye and hand movement in the left eye. On slit lamp examination of the left eye, severe inflammation was seen in the anterior chamber (cells +4) and the vitreous (cells +4). Fundus examination of the left eye demonstrated thick, white, confluent sheathing surrounding the retinal veins and arteries from the posterior pole to the periphery with extensive retinal hemorrhages, optic disc swelling, and macular edema (Fig. 1A). The right eye was normal. B-scan ultrasonography and spectral-domain optical coherence tomography of the left eye showed a severely edematous and detached retina in posterior pole (Fig. 1B and 1D). Fluorescein angiography demonstrated a prolonged arteriovenous transit time, blockage of fluorescein corresponding to extensive retinal hemorrhage, widespread area of capillary non-perfusion, and extensive staining of sheathing veessels (Fig. 1G). A diagnosis of occlusive retinal vasculitis resembling acute FBA was made and systemic evaluation for retinal vasculitis was performed. The patient had a history of recurrent genital and oral ulcers over two years, but no other systemic manifestations of Behçet's disease on presentation. The results of laboratory examinations, including serology for herpes virus, varicella zoster virus, and human immunodeficiency virus were normal or negative. Other examinations, including brain magnetic resonance imaging and polymerase chain reaction assay for varicella zoster virus and cytomegalovirus in the aqueous humor, were negative or normal. Human leukocyte antigen typing resulted in a positive HLA-B51.
The patient was started on intravenous methylprednisolone. Vitreous opacity progressed and angle hypopyon appeared until 24-hour after treatment initiation (Fig. 1C). However, during two weeks after treatment, the vascular sheathing and vitreous opacity gradually disappeared. Systemic steroids were slowly tapered during the next two months and cyclosporine 150 mg/day was added. Two months later, follow-up angiographic findings revealed a widespread area of non-perfusion in three retinal quadrants with neovascularization of the disc (Fig. 1H). Although panretinal photocoagulation for non-perfusion areas was performed, neovascularization progressed by four months (Fig. 1F). However, iris rubeosis and neovascular glaucoma had not developed by 10 months. Six months after his presentation, he developed two ulcers on oral mucosa and pseudofolliculitis on his face, along the hairline. A diagnosis of Behçet's disease was made using the international criteria following a rheumatology consultation. Eight months later, follow-up optical coherence tomography imaging revealed atrophy and disruption of the photoreceptor layer in the macular area (Fig. 1E). The final visual acuity was hand movement in the left eye. He is currently on maintenance cyclosporine therapy.
Discussion
FBA can be idiopathic or associated with various ocular and systemic disorders. In 1997, Kleiner [4] classified the patients who had the appearance of FBA into three subgroups. First are patients with lymphoma or leukemia whose disease is due to infiltration with malignant cells (frosted branch-like appearance). Second is the group of patients who have associated viral infections or autoimmune disease (secondary FBA). Cases associated with Behçet's disease such as this study can be classified into this subgroup. Finally, there is a group of otherwise healthy young patients who develop acute visual loss (acute idiopathic FBA).
Our case can be classified into acute idiopathic FBA because systemic examination revealed no obvious abnormalities except positive HLA-B51 and ocular findings on presentation. However, the history of recurrent oral and genital ulcers over a period of two years and a positive HLA-B51 suggested the possibility of an underlying Behçet's disease [1,11]. Obliterative retinal vasculitis and hypopyon iritis on presentation also supports ocular manifestations of Behçet's disease [1,11]. Six months after his ocular presentation, he developed oral ulcers and pseudofolliculitis, which led the authors confirm the diagnosis of Behçet's disease with secondary FBA. The patient had severe occlusive vasculitis involving three quadrants of his retina, initial visual acuity was hand movement, and the patient had no visual improvement even with the proper treatment. For these reasons, the authors started early immunosuppressive treatment to prevent involvement of the contralateral eye before confirming the diagnosis of Behçet's disease.
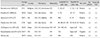
The authors found six cases in PubMed using the search parameters of "frosted branch angiitis, Behçet's disease." Including this study, seven cases are discussed here [5-10]. Table 1 shows the characteristics of patients diagnosed as having secondary FBA associated with Behçet's disease. All cases aside from this study presented with improvement of visual acuity during the follow-up period, and three cases recovered their sight up to 20 / 20 or 10 / 10. Four cases presented with bilateral involvement, and while three cases presented with bilateral involvement initially, the other one was reported to affect both eyes, two years apart [5,8-10]. This case suggests that the subsequent involvement of the other eye could occur and early immunosuppressive treatment should be considered, especially in cases of initially unilateral involvement [9]. Three cases presented with neuro-Behçet's disease and two cases revealed typical hypopyon iritis. All patients had a history of recurrent oral or genital ulceration, and five of six cases had a positive HLA-B51. These findings suggest that both a careful history and a positive HLA-B51 can help make a diagnosis of underlying Behçet's disease.
In summary, this case revealed that FBA can be an ocular manifestation of Behçet's disease, which could initially be unilateral and result in blindness, particularly when combined with severe occlusive retinal vasculitis. This condition may consecutively involve both eyes and result in the deterioration of bilateral visual function. Thus, the authors recommend that Behçet's disease should be considered in a diagnostic workup for unilateral FBA, and a careful history and a positive HLA-B51 are helpful to establish an early diagnosis. In addition, it is recommended that patients with unilateral FBA with suspicion of Behçet's disease should be treated with the early immunosuppressive treatment in order to prevent the involvement of the contralateral eye.

 XML Download
XML Download