

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Refractive error is caused by refractive changes, resulting from the difference in refractive power according to the curved surface of the cornea and crystalline lens, and the axial changes associated with the axial length (AL) such as corneal thickness, anterior chamber depth (ACD), crystalline lens thickness (LT), and vitreous chamber depth (VCD) [1,2].
Many prior studies have reported on the correlation between the refractive error and the distribution of ocular values. Olsen et al. [3] reported that ocular refraction is correlated with the corneal power (CP), the lens power and the AL. Wong et al. [4] reported that the VCD was the most important determinant of refraction in adults over 40 years of age. However, the mechanism associated with the development of anisometropia has not been well defined. Previous studies have reported on the correlation between the degree of anisometropia and AL [5]. We determined the correlation of differences in other ocular component values (CP, ACD, crystalline LT, and VCD) as well as AL with the degree of myopic anisometropia.
Materials and Methods
Fifty patients presenting to this hospital over a two-year period from January 2007 to December 2008 were enrolled in this study. This retrospective study design followed the tenets of the Declaration of Helsinki for biomedical research and it was approved by the institutional review board of the review board of the Catholic University of Korea in Seoul, Korea.
The subjects were divided into 6 groups according to the difference in refractive error: group 1, 1.50-2.99 D; group 2, 3.00-3.99 D; group 3, 4.00-5.99 D; group 4, 6.00-7.99 D; group 5, 8.00-11.99 D; and group 6, ≥12.00 D. Refraction was measured with an auto refractometer (RK-5; Canon, Tokyo, Japan). The measurements included crystalline LT, ACD, VCD, and AL by A-scan ultrasonometry (Ultrascan; Alcon, Irvine, CA, USA). In addition, the CP in a 3 mm zone at the center of the cornea was measured with a keratometer (OM-4; Topcon, Tokyo, Japan).
The correlation between the differences in the ocular component values with the degree of anisomyopia was analyzed by linear regression analysis and the mean ages of each group were analyzed by one-way analysis of variance using SPSS ver. 19.0 (SPSS Inc., Chicago, IL, USA; a p < 0.05 was the accepted level of significance).
Results
The age on average was 36 ± 14.9 years and the age range was from 19 to 68 years. There were 30 males and 20 females. All subjects had anisomyopia with a difference equal to or more than 1.50 diopters (D) in both eyes. Twelve patients had amblyopia. The difference in the refractive error on average was 6.83 D. Five had refractive differences (RD) from 1.50 to 2.99 D, 11 had RD from 3.00 to 3.99 D, 9 had RD from 4.00 to 5.99 D, 12 had RD from 6.00 to 7.99 D, 7 had RD from 8.00 to 11.99 D, and 6 had ≥12.00 D. The mean age per group is presented in Table 1. No statistical difference in age was observed among the groups (one-way analysis of variance, p = 0.997). The mean refractive errors of the smaller eye and larger eye were calculated for each group (Table 1). The ocular component value for CP, ACD, and LT of the smaller and larger eyes in patients with anisometropia are presented in Table 2. The ocular component value of AL, VCD, and ACD + LT of the smaller and larger eyes in patients with anisometropia are shown in Table 3. The interocular difference of the ocular components are represented by the following figures: ΔACD, ΔLT, ΔAL, Δ(ACD + LT), ΔVCD, and ΔCP.
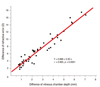
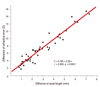
As the degree of anisometropia increased, there was no significant correlation among the ΔCP, ΔACD, ΔLT, and Δ(ACD + LT) (p = 0.439, p = 0.063, p = 0.255, and p = 0.366, respectively). However, the RD showed a significantly positive correlation with the VCD and AL (r = 0.963, p < 0.0001 for both) on the linear regression. A significant positive correlation was found between RD and AL, which was primarily caused by the difference in the depth of the vitreous chamber (r = 0.963) (Figs. 1 and 2). The linear correlation equations of ΔVCD and ΔAL, the ocular components that affect the degree of anisometropia, were RD = 0.782 + 2.281 ΔAL, r = 0.963, and RD = 0.888 + 2.304 ΔVCD, r = 0.963, which shows strong positive correlations for both parameters (Figs. 1 and 2).
The average value of ocular components in the smaller eye and the larger eye were compared in Fig. 3. The average degree of anisometropia was 6.83 D. There was a 0.13 mm difference in ACD, a 0.05 mm difference in LT, a 0.19 mm difference in the length between the cornea and the posterior surface of the lens surface, a 2.55 mm difference in VCD, and a 2.61 mm difference in the AL. The AL difference was due primarily to the difference in vitreous depth. There was also a difference in the corneal refractive power of 0.13 D.
Discussion
Refractive anisometropia is a condition that requires different corrective lenses for each eye due to the difference of refraction between the eyes. Aniseikonia is induced by spectacle correction. Generally, the difference in refractive error between each eye is minimal; this is referred to as physiologic anisometropia. If there is a difference of more than 2.00 D, this is referred to as refractive anisometropia.
Brown [6] reported that the depth of the vitreous decreases as age increases. Comparison of eyes with emmetropia and myopia, show a more significant correlation between the vitreous depth and myopia than between the vitreous depth and emmetropia, by most investigators [7-9]. The growth of the AL and the increase of the depth of the vitreous is the main factor with regard to the development of myopia [10].
Several studies have been conducted to explore the interocular difference in anisometropia. However, there are few studies exploring the relationship between various ocular components and the degree of anisometropia. Two such studies showed that anisometric children had greater interocular differences in AL [5,11]. One of these reports studied a population with a broad age-range that included some individuals with mature eyeballs and others with immature eyeballs [11]. The low ages of subjects in that and another study may have skewed the results, as the eyeballs of those subjects are still in the process of enlarging [11,12]. In contrast, the population used in this study was composed of subjects with mature eyeballs and a more homogenous sample in general.
In a population-based sample of 6-year-old children, anisometropia resulted from relatively large interocular differences in AL and ACD, but not average CP [11]. Tayah et al. [13] showed that there was a significant correlation between RD and the difference of AL, and a weak correlation between RD and crystalline difference. Zaka-Ur-Rab [5] reported that RD had a positive correlation with AL (r = 0.674, p < 0.001). The difference between the AL within a pair of eyes is considered to be a major contributor to anisometropia in myopic cases. In this study, we present a positive correlation between RD and the difference of AL (r = 0.963, p < 0.0001) as well as a positive correlation between RD and the difference of VCDs (r = 0.963, p < 0.0001). However, RD showed no significant correlation with crystalline difference, ACD, or CP.
In this study, interocular differences of AL, VCD, except LT, ACD, and CP was significant in anisomyopia (paired t-test, p < 0.05). The severity of anisomyopia was not correlated with the between-eye differences in the anterior chamber values of the eyeball (CP, ACD, LT, and ACD + LT) by linear regression. The severity of anisomyopia was significantly correlated with the between-eye differences in VCD.
Lee and Kwon [14] reported that the best-corrected visual acuity of anisometropic eyes was correlated with the amount of ansiometropia in children. In adults, the best-corrected visual acuity of anisometropic eyes was also correlated with the amount of ansiometropia (r = -0.287, p = 0.043).
The limitations of this study include the analysis of only anisomyopia and the small number of subjects used. A prospective study of the different types of refractive anisometropia with a larger number of subjects is needed.
In conclusion, the degree of anisomyopia was not significantly different with regard to the corneal refractive power of both eyes (p > 0.05). The distance from the cornea to the posterior surface of the lens did not appear to have a significant effect on the degree of anisometropia (p > 0.05). The degree of anisometropia had a significant correlation with the AL (r = 0.963) caused by the difference in the VCD (r = 0.963). The larger the differences in VCD between the eyes, the greater the severity of anisomyopia.




 XML Download
XML Download