

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Penetrating keratoplasty (PKP) has been the definitive surgical treatment option for keratoconus for the past few decades [1-3]. Recently, deep anterior lamellar keratoplasty (DALK) has been considered an acceptable alternative treatment because it has the advantage of eliminating the risk of endothelial rejection and intraocular complications [4,5].
Considering that most patients with keratoconus are young, and that postoperative best-corrected visual acuity (BCVA) is expected to be acceptable, the objective of keratoconus surgery is not only to achieve a clear graft, but also to minimize refractive errors that can last a lifetime. In PKP, oversized donor grafts tend to result in postoperative myopia that is significantly greater than that resulting from same-size donor grafts [6-8]. Despite the concern of flat graft-related complications, such as wound leakage and hyperopic residual refraction [9], numerous attempts have been made to reduce postoperative myopia by using either same-size or smaller donor grafts [10-12].
Few studies have directly compared same-size grafting in DALK with same-size grafting in PKP. Recent studies have reported that DALK with same-size donor grafts results in relatively low myopia [13-15]; however, the optical effect of same-size grafting in DALK for keratoconus is still undetermined.
The aim of this study was to compare clinical outcomes, focusing particularly on optical changes, between DALK and PKP with same-size grafts in patients with keratoconus.
Materials and Methods
In this retrospective study, we reviewed the clinical charts of 16 eyes from 15 patients with keratoconus who underwent corneal transplantation at Seoul National University Hospital between June 2005 and April 2011. DALK with same-size donor grafts was performed for 11 eyes, PKP with same-size donor grafts for 5 eyes. Cases with a minimum follow-up of 12 months were included in the statistical analysis.
Keratoconus diagnosis was based on clinical findings from slit-lamp examination (conical protrusion of the apical cornea, Vogt striae, Fleisher ring, corneal thinning, and epithelial and sub-epithelial scarring) and keratoconus symmetry index [16]. Patients with contact lens intolerance or who were poor candidates for contact lens fitting due to advanced cone underwent keratoplasty. Patients with a history of vernal keratoconjunctivitis, other ocular diseases such as glaucoma and retinal disease, or any previous ocular surgery were excluded from this study. Patients who had intraoperative complications were also excluded. Based on preoperative keratoconus severity, patients were divided into 2 groups: moderate (46 diopter [D] < mean keratometric value <55 D) or advanced (mean keratometric value >55 D or unmeasurable keratometric value).
All patients were operated on by the same surgeon (MKK) at the same institution (Seoul National University Hospital, Seoul, Korea). Procedures were performed while patients were under general anesthesia. DALK was performed using a hydrodissection technique [17,18]. In brief, a half-thickness (250 µm) trephination was performed using the Hessburg-Barron trephine (JedMed Instrument, St. Louis, MO, USA), and the anterior lamella was dissected and removed using a Beaver no. 69 blade (BD, Franklin Lakes, NJ, USA). A 30-gauge needle was beveled, introduced into the deep stroma, and balanced salt solution was gently injected into the stroma for stromal hydrodissection. The stroma was dissected by more than 90% to clearly visualize the Descemet membrane. Using a Barron donor punch (Katena, Denville, NJ, USA), we cut the donor cornea to match the diameter of recipient trephination. Subsequently, the endothelial layer was gently stripped off. The donor cornea was then placed into the recipient bed and sutured with the interrupted or combined technique using 10-0 nylon. In PKP, the recipient cornea was cut with a Hessburg-Barron suction trephine. A same-size donor cornea was punched out using the Barron donor punch and sutured with the interrupted or combined technique. Topical moxifloxacin and prednisolone were applied every 6 hours, and 30 mg of oral prednisolone was administered for 1 week and tapered within 2 weeks. Based on topographic astigmatism, selective suture removal was initiated a minimum of 3 months after the operation and continued over the follow-up period until acceptable topographic astigmatism was achieved.
Outcome measures included BCVA with conversion to logarithm of the minimum angle of resolution (logMAR), refractive error, and endothelial cell count. Postoperative refractive error was measured by automated keratometry (KR-8100; Topcon, Tokyo, Japan), and mean simulated keratometric index (Sim K), corneal astigmatism, 3-mm and 5-mm zone irregular astigmatism, and central corneal thickness were measured by Orbscan II (Orbtec; Bausch & Lomb, Rochester, NY, USA) at 1-year and final follow-up. Endothelial cell density was counted by specular microscopy (Konan specular microscope SP-8800; Konan Medical, Nishinomiya, Japan).
Data were analyzed using SPSS ver. 18 (SPSS Inc., Chicago, IL, USA). All measurements are expressed as mean ± SD. The Mann-Whitney test was employed to compare study outcomes between the study groups, and p ≤ 0.05 was considered statistically significant. The chi-square and Fisher's exact tests were used to compare qualitative parameters. The study was approved by the Seoul National University Hospital ethics committee.
Results
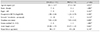
DALK with same-size donor grafts was performed for 11 eyes from 10 subjects and PKP with same-size donor grafts was performed for 5 eyes from 5 patients. The base-line characteristics and preoperative clinical data of all patients are summarized in Table 1. There were no significant differences in baseline characteristics between the two groups.
With respect to visual comparisons between both types of surgeries, the mean final BCVA was 0.34 ± 0.32 (range, 0.046 to 1.00) logMAR in the DALK group and 0.52 ± 0.69 (range, 0.046 to 1.70) in the PKP group (p = 0.980, Mann-Whitney test). BCVA of >20 / 40 was achieved in 64.0% and 60.0% patients in the DALK and PKP groups, respectively (p = 1.000, Fisher's exact test) (Table 2), suggesting comparable visual outcome in both groups. Interface opacity was not detected in any cases in the DALK group.
Our study provided interesting results regarding optical properties in the DALK group. At 1-year follow-up, postoperative mean Sim K was higher in the DALK group (46.91 ± 2.29 D) than it was the PKP group (43.97 ± 1.19 D), a statistically significant difference (p = 0.018, Mann-Whitney test), and was stable at 47.16 D in the DALK group at final follow-up. Meanwhile, in the PKP group, postoperative mean Sim K tended to increase over time because of continued stitch removal and was 47.74 ± 3.02 D at final follow-up, which was not significantly different from the DALK group (p = 0.527, Mann-Whitney test). Postoperative spherical equivalent (SE) refractive error was similar between the groups at both 1-year and final follow-up (p = 0.277 and p = 0.659, respectively; Mann-Whitney test). The incidence of astigmatism tended to be lower in the DALK group than in the PKP group for all follow-up periods, but these differences were not statistically significant. Interestingly, 5-mm corneal irregularity indices were significantly less in the DALK group than in the PKP group at 1-year follow-up (p = 0.021, Mann-Whitney test), however, there was only marginal significance at final follow-up (p = 0.084, Mann-Whitney test) (Table 3 and Fig. 1). Mean time from operation to suture removal was lower in the DALK group (9.6 ± 4.2 months) than in the PKP group (23.6 ± 14.9 months, p = 0.021, Mann-Whitney test).
As expected, mean central corneal thickness was signifi cantly greater in the DALK group than in the PKP group at 1-year follow-up (p = 0.035, Mann-Whitney test) and was quite similar between the groups at the final follow-up (p = 0.052, Mann-Whitney test). Endothelial cell counts were lower in the PKP group than in the DALK group at the final follow-up (p = 0.021, Mann-Whitney test).
Discussion
Our retrospective study revealed that visual and optical outcomes after DALK are comparable to those after PKP. Our study also confirmed that a patient's endothelial cell count remains stable after DALK, whereas a reduction in endothelial cells occurs after PKP.
Recently, DALK has increased in popularity due to its prevention of the main withdrawal factors of lamellar keratoplasty, such as interface opacity [19]. Many studies have reported that visual outcomes after DALK surgery using the big-bubble technique are comparable to those after PKP [13,20-23]. The results of our study, in which a hydrodissection technique was used for DALK surgery, corresponded well with the results of these studies and support the feasibility of using DALK for treating keratoconus. Generally, the percentage of keratoconus patients who achieve a BCVA of >20 / 40 after DALK ranges between 72% and 92% [17-20]. In our study, corroborating visual outcomes were achieved, with 64.0% of the eyes treated with DALK obtaining a BCVA of 20 / 40 or better.
Meanwhile, a reduction in myopia as well as in astigmatism is a major concern in surgically treated keratoconus. In PKP, same-size donor grafts have been reported to be effective in reducing high myopia [10-12]. However, the effect of the size disparity between the recipient and donor graft on myopia in DALK had not been fully determined until now. In this study, we examined the effects of same-size grafting in DALK on myopic SEs. Unexpectedly, we discovered that the mean SE was -7.64 D after final stitch removal (range, -0.88 to -16.8 D). This indicated a higher myopia than that reported by other studies with same-size donor grafts, which had SE values of -1.0 ± 1.8 D [23], -1.81 D (range, -7.56 to +3.65 D) [13], -3.50 D (median) [14], and -2.54 D (range, -1.65 to -4.13 D) [15], and even higher than that reported by studies with oversized donor grafts, which had values of -2.91 ± 1.7 D [24], -3.13 ± 2.63 D [25], and -0.90 ± 2.71 D [19] (Table 4).
We hypothesize that 3 factors contribute to postoperative myopia in DALK: axial length, preoperative corneal steepening, and residual bed thickness, rather than discrepancy between donor graft size and recipient trephination. Javadi et al. [26] and Shimmura et al. [9] also reported that reducing recipient-donor disparity cannot be expected to dramatically negate the postoperative axial myopia of keratoconic eyes after DALK or PKP, respectively. In our study, mean axial length was 25.08 mm, which is much greater than 24.50 mm, the reference value used by Shimmura et al. [9] for determining the disparity between the donor and recipient cornea. Thus, axial length is a critical factor that explains the lack of reduction of postoperative myopia in same-size DALK surgery.
Another factor determining postoperative myopia is likely the preoperative keratometric value, especially for DALK, in which the Descemet membrane is left intact. In our study, preoperative mean keratometric value in the DALK group was 59.85 ± 1.55 D, and the keratometric values for 3 patients were not measurable because of extreme corneal steepness. These preoperative keratometric values were relatively higher than those in previous studies that observed low postoperative myopia after DALK (54.43 ± 5.2 D [24] and 53.94 ± 6.74 D [27,28]). We postulate that postoperative keratometric value might be dependent, at least in part, on the preoperative keratometric value rather than graft size disparity. This means that same-size corneal grafts might not be effective in flattening the cornea after DALK for advanced keratoconus. In fact, in the present study, postoperative mean Sim K was 47.16 ± 1.98 D with same-size grafts, which is not dramatically different from the 46.83 D ± 2.0 D [26] and 45.53 D ± 2.75 D [19] reported in the other studies with 0.25-mm oversize grafts. This suggests that size disparity is not a critical factor in determining postoperative corneal steepening.
Finally, residual bed thickness could determine stiffness and corresponding resistance against the compressive forces of the donor graft. This concept was partially embraced by Arjdomand et al. [29] who recommend a residual stromal bed of 20 um or less to achieve good visual outcomes after DALK. For ease of understanding, we adopted a simple model to explain how the residual bed can influence the effect of donor grafts on myopia after DALK (Fig. 2). Regarding the laws of equilibrium of forces on the graft, tensile forces of the peripheral recipient cornea, which act downward, counteract the two upward forces: those provided by the pressure of the aqueous humor and the pushing force of the recipient bed against the graft (Fig. 2A). In this static equilibrium condition, stiffness, which refers to the resistance of an elastic body to deformation by an applied force, becomes a crucial factor. For example, in the cornea, the postoperative deflection of preoperative corneal steepness is mainly determined by the stiffness of the peripheral recipient cornea and residual bed below the lamellar interface. Among the aforementioned factors, we specifically focused on the residual bed. If the stiffness of the residual recipient bed decreases (for example, in a thinner residual bed), the graft exerts compressive force on the recipient bed effectively and it flattens easily, resulting in flattening of the graft (Fig. 2B). In contrast, if stiffness of the residual recipient bed increases (for example, in a thicker residual bed) and stiffness of the peripheral cornea decreases (which occurs with a thinner peripheral cornea in advanced keratoconus cases), the residual cornea would resist the downward flattening force, resulting in steepening of the graft (Fig. 2C). Physically, the bending stiffness of the residual bed is proportional to the triple-square of the thickness of the residual bed in this physical model [30], which can be applied with respect to DALK. This suggests that residual bed thickness and preoperative corneal steepness of the keratoconic eye have an effect on postoperative keratometry and refractive state. Based on this concept, we checked residual bed thickness in the anterior segment by OCT (Visante; Carl Zeiss Meditec, Dublin, CA, USA) in some patients (n = 5, unpublished data) and found that the mean residual thickness was 72 ± 19.6 µm. We prefer the hydrodissection technique, which has the advantages of smaller increases in intraocular pressure and less induction of apoptosis in the peripheral stroma compared with those observed in the big-bubble technique [17]. Thicker residual beds in present study might be partially involved in the hydrodissection technique, which provides inferior visualization of the Descemet membrane to that provided by the big-bubble technique. Taken together, thick residual recipient bed, steep preoperative cornea, and greater axial length appears to result in moderate postoperative myopia after DALK despite the use of same-size grafts. Larger prospective randomized studies of patients with advanced keratoconus treated with DALK should be performed to confirm this hypothesis with respect to postoperative myopia after DALK.
On the other hand, DALK with same-size grafting appears to result in less peripheral irregular astigmatism. Corneal irregularity indices measured at 5 mm in the DALK group were less than those in the PKP group at 1-year follow-up. Most of cases in DALK had complete suture removal before 1-year follow-up. In the PKP group, corneal irregularity indices at 5 mm tended to decrease over time because of continued stitch removal; there was only marginal significance between the 2 groups at the final follow-up. Thus, DALK may have a beneficial effect through early completion of suture removal that resulted in early stabilization of corneal irregular astigmatism. This advantage in reducing peripheral irregular astigmatism was more prominent when DALK was compared to PKP with a 0.25-mm-oversized graft. Most of the baseline characteristics and postoperative parameters including refractive error and topographic data were comparable between DALK with same size graft and PKP with oversized graft; however, 3-mm and 5-mm peripheral irregular astigmatism were significantly less in DALK than in PKP with oversized graft at final follow-up (Appendix 1). In oversized grafting, Javadi et al. reported that high order aberration and contrast sensitivity function are comparable between DALK and PKP. In present study, because high order aberration and contrast sensitivity data were not available, the effect of irregular astigmatism on visual quality could not be evaluated. To clarify the clinical relevance of decreasing irregular astigmatism, further studies comparing high order aberration between DALK with same-size grafting and PKP with same-size grafting are needed.
In conclusion, the optical outcomes of DALK with same-size grafts are comparable to those of PKP with same-size grafts for treatment of keratoconus, while DALK also preserves the endothelial cell counts that are diminished in PKP.





 XML Download
XML Download