

 PDF
PDF ePub
ePub Citation
Citation Print
Print


It is clinically difficult to diagnose a lesion in the lacrimal caruncle because such lesions are relatively rare and variable. Of the few reports on caruncular lesions, most have been nevi, papillomas, or sebaceous gland hyperplasias, both benign and malignant [1-3]. However, reports on infectious disease in the caruncle are rare. There are few case reports on caruncular abscess caused by bacterial infection [4,5]. We report a case of actinomyces infection on the caruncle, leading to an abscess. The actinomyces infection was confirmed by histopathologic examination.
Case Report
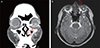
A 47-year-old woman was a dmitted to o ur clinic for persistent purulent discharge from the left eye for a duration of six months. She had been diagnosed with chronic conjunctivitis at a private eye clinic. Despite conservative treatment, the symptom was persistent, leading to referral of this patient to our clinic. Her corrected visual acuity was 1.2, and no specific findings were noted in her past medical history. Slit lamp examination showed discharge via a fistula in the central part of the caruncle of the left eye, a red and swollen caruncle, and mild hyperemic conjunctiva (Fig. 1). Lacrimal drainage was patent to syringing and showed no reflux in the upper or lower canaliculus of the left eye. Computed tomography (CT) scan and magnetic resonance imaging (MRI) showed an elliptical hypo-dense lesion of about 1 cm in diameter in the medial portion of the left lower eyelid (Fig. 2). Caruncular abscess was diagnosed preoperatively, and excisional drainage and bacterial culture were performed. Intraoperative lacrimal probing and irrigation were performed to confirm that the abscess and canaliculus were not connected. Bacteria were not identified in the culture, but biopsy of the lesion confirmed a benign purulent cyst with 'sulfur granules' by histopathologic examination (Fig. 3). Postoperative oral and topical antibiotics were administered; the lesion resolved with no evidence of recurrence within four months, and the symptom significantly improved.
Discussion
Actinomycosis is a chronic disease that spreads to surrounding tissues with the formation of abscesses and granulomas that are typically accompanied by microcolonies known as 'sulfur granules' [6]. Actinomyces is a genus of the Actinobacteria, anaerobic gram-positive organisms that grow through the formation of hyphae [6]. The diagnosis of actinomycosis is confirmed microbiologically by the identification of Actinomyces in a sample obtained from the lesion and pathologically by observing sulfur granules from tissue or an abscess. Actinomycosis is a relatively rare disease, and although some cases of orbital cellulitis and chronic endophthalmitis after cataract surgery were reported to generate cultured actinomyces [6-8], most of the described cases have been canaliculitis.
Actinomyces canaliculitis is usually accompanied by a mucopurulent punctal discharge, epiphora, inflammation of the medial canthus, a thickened canaliculus, and a red pouting punctum [6]. Since the frequency of canaliculitis is low, it is often mistaken for refractory chronic or recurrent conjunctivitis, although differentiation is possible by confirming the presence of purulent discharge from the punctum.
The case under discussion was originally mistaken for chronic conjunctivitis due to erythema, swelling, and purulent discharge from the pericaruncular area. After failing to respond to treatment, the patient was referred to us. Although canaliculitis can show a similar pattern, the purulent discharge was observed to not originate from the punctum, and a CT scan and MRI identified a lesion near the lower eyelid, which led to a preoperative diagnosis of a caruncular abscess. A biopsy confirmed the presence of 'sulfur granules' containing masses of Actinomyces. Topical ciprofloxacin and oral penicillin antibiotics were administered postoperatively, and the erythema and swelling of the pericaruncular area gradually decreased; purulent discharge was no longer observed.
Reports of caruncle infection a re d ifficult to find, although Koo and Chang [4] reported a case of caruncular abscess with Methicillin-resistant Staphylococcus aureus, and Pappalardo et al. [5] reported granules of the caruncle caused by actinomycosis. To our knowledge, this is the first reported case of caruncular abscess with chronic purulent discharge caused by actinomycosis in Korea. Actinomyces should be considered as a potential agent of chronic infection in the caruncle.


 XML Download
XML Download