

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Optical coherence tomography (OCT) is the most common imaging tool used to examine the macula, as it is the only instrument that provides direct visualization of the in vivo retinal structure [1]. The traditional OCT technique involves time-domain OCT (TD-OCT) [2-5], where retinal depth information is obtained with a reference arm after longitudinal translation over time [6]. Good reproducibility of retinal thickness measurements by Stratus OCT (Carl Zeiss Meditec, Dublin, CA, USA) has been demonstrated [7,8]. However, since the time-domain method samples only one point at a time, a relatively long period of time is needed to obtain A- and B-scan images, resulting in lower image resolution compared to spectral domain-OCT (SD-OCT) [9].
Newer SD-OCT offers improved image resolution of less than 5 to 7 µm, dramatically faster acquisition speeds (18,000 to 40,000 A-scans/second), and detailed views of the intraretinal microstructures as well as three-dimensional images of the retina [8,10-12]. In SD-OCT, light beams returning from the sample and reference paths are combined at the detector, and then a spectrometer resolves the interference signals throughout the depth of each A-scan without varying the length of the reference path [9]. This allows the acquisition of retinal images approximately 50 times faster with SD-OCT than with TD-OCT [13] and results in improved resolution of the B-scan images and better delineation of the retinal layers, including the retinal pigment epithelium (RPE)-Bruch's membrane choriocapillaris complex [14,15].
Numerous studies and clinical trials have used foveal thickness (FT) values that are measured by Stratus OCT for the determination of macular lesions, such as those in exudative age-related macular degeneration (AMD) and macular edema, and for the assessment of treatment response and guidelines for retreatment [16-18]. In order to use the known treatment and follow-up guidelines that are proposed in numerous clinical studies, it is essential to match the thickness parameters of different OCT devices, especially between TD-OCT and SD-OCT. A recent study on normal subjects demonstrated that Spectralis OCT (Heidelberg Engineering Inc., Heidelberg, Germany) obtained retinal thickness measurements that were increased by approximately 65 to 70 µm compared to Stratus OCT measurements [19].
However, studies have reported discrepancies in FT values measured by TD-OCT and SD-OCT in eyes with various retinal diseases [20-23]. Stratus OCT defines retinal thickness from the internal limiting membrane (ILM) to the complex of the inner and outer segments (IS/OS) of the photoreceptor junction and RPE layer, while Spectralis OCT selects images from the ILM to the RPE-Bruch's membrane choriocapillaris complex [12]. Because the segmentation algorithm for each OCT instrument is different, the measured FT should also be different for each. One study using Stratus and Spectralis OCT reported that the mean foveal thickness differences (FTD) in eyes with choroidal neovascularization (CNV) and AMD were significantly greater than those in normal eyes and in other retinal diseases [20]. Conversion equations and their application to TD-OCT and SD-OCT for the examination of eyes with diabetic macular edema [22] and with AMD [23] have been previously reported. However, no studies have compared the distribution of FTDs in various retinal diseases or constructed conversion formulas that predict TD-OCT-measured FT on the basis of SD-OCT-measured FT across different retinal diseases. In addition, the association between the amount of FTD and the disease severity indicated by FT has not yet been investigated.
The purpose of this study was to compare the measurement values obtained using TD-OCT (Stratus) and SD-OCT (Spectralis) devices in normal and diseased retinas in order to construct conversion formulas in normal eyes and eyes with various retinal diseases. These conversion formulas must be as accurate as possible in order to predict the FT provided by Stratus OCT on the basis of data obtained using Spectralis OCT. The accuracy of these formulas must also be verified to ensure minimal errors in clinical application.
Materials and Methods
This was a retrospective cross-sectional study comparing measurement values between TD-OCT and SD-OCT devices in normal and diseased retinas. This study was approved by the Institutional Review Board of Seoul National University Bundang Hospital, and the tenets of the Declaration of Helsinki were followed throughout the study.
Consecutive patients who visited the retina clinic of Seoul National University Bundang Hospital and who were examined with both Stratus and Spectralis OCT between September 2009 and October 2009 were included in this study. Because the new Spectralis OCT was first introduced to our hospital in September 2009, there was no information regarding the FT of the new SD-OCT machine. Therefore, all subjects who visited the retina clinic during this period and who were indicated for OCT examination underwent both Stratus and Spectralis OCT examinations of a dilated pupil on the same day by two well-trained OCT technicians. The medical records and OCT data of 366 consecutive patients (475 eyes) and 13 normal controls (13 eyes) were retrospectively reviewed. Ocular disorder diagnoses were obtained from a computerized database of electronic medical records. Thirteen eyes of 13 subjects who visited the retina clinic during the study period without posterior segment pathology and with definite normal features on OCT scanning were categorized as normal.
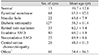
Eyes with retinal pathology were categorized into eight retinal disease groups: epiretinal membrane (ERM, n = 68), macular hole (MH, n = 22), diabetic retinopathy (DR, n = 127), retinal vein occlusion (RVO, n = 53), exudative AMD (n = 80), nonexudative AMD (n = 25), central serous chorioretinopathy (CSC, n = 26), and others (rhegmatogenous retinal detachment, n = 18; normal tension glaucoma, n = 15; uveitis, n = 19; and senile retinoschisis, n = 9). Retinal diseases with pathological changes that were mostly confined within the inner retina, including ERM, MH, DR, and RVO, were defined as the inner-retinal disease group.
When measuring FT with Stratus OCT, we used a 6-mm linear cross-hair pattern that was centered on the fovea (512 A-scans; scan length, 6.0 mm) and a fast macular thickness map pattern. The automated analysis package of the Stratus OCT defines retinal thickness as the distance between the ILM and the complex of the photoreceptor junction of the IS/OS layer (Fig. 1A) [1,24].
The axial resolution of Spectralis OCT is less than 7 µm with a data-acquisition speed of 40,000 A-scans/second [24]. Scans were obtained with the automated averaging system (automatic real time mean = 10) activated in order to amplify the signals and to reduce the noise in the images [24]. Retinal thickness was defined as the distance between the ILM to the bottom of the RPE-Bruch's membrane choriocapillaris complex by automatic segmentation algorithms of the Spectralis software (Fig. 1B) [1,24]. The average retinal thickness within a 1-mm radius of the central fovea on the Early Treatment Diabetic Retinopathy Study grid, as measured using Stratus and Spectralis OCT, was defined as FT in normal subjects and subjects with any form of retinal disease, including macular hole [1].
For each scan, the color thickness maps and horizontal line scans of the Stratus and Spectralis OCTs were reviewed for image artifacts due to failure of identification of the inner or outer retinal boundaries or to segmentation algorithm failure, that is, when segmentation lines of the OCT images were not properly placed. All comparisons and analyses of FT were performed after the exclusion of artifacts on OCT scans.
The FTD was defined as the difference between the FT values that were measured by Stratus and Spectralis OCT in the same patient. The mean value of the FTDs of each retinal disease group was compared to that of the normal group. The proportion of eyes that had FTDs that were 1.96 standard deviations (SD) from the mean FTD of normal eyes was compared between disease groups, and the coefficients of variation of the FTDs were calculated in order to analyze the degree of relative dispersion of the FTDs in each disease category.
Because the thickness of the CNV was included in the FT that was measured by Spectralis OCT (Fig. 1D), but not in the Stratus OCT-measured FT (Fig. 1C), each OCT image of the exudative AMD group was reviewed to measure the CNV thickness using the Heidelberg Explorer ver. 4.0 software package (Heidelberg Engineering Inc.). Erroneous outer segmentation lines in OCT images obtained for patients with exudative AMD, including CNV thickness, were repositioned manually into the RPE-Bruch's membrane junction. CNV thickness was then subtracted from the original FT measured using Spectralis OCT and was defined as a Modified Spectralis OCT FT. In addition, the FTD between the FT of Stratus OCT and modified Spectralis OCT FT was defined as Modified FTD. Finally, an additional conversion formula was constructed from the FT value measured by Stratus and Spectralis OCT and CNV thickness using generalized estimating equations (GEE).
Statistical analysis was performed with SAS ver. 9.1 (SAS Institute Inc., Cary, NC, USA). Comparisons of the differences in FTDs of patients with different retinal disorders measured by Stratus and Spectralis OCT were performed using GEE to adjust for the inclusion of bilateral eyes of individuals. The working correlation structure was assumed to be exchangeable or independent. The mean FTDs of the disease groups and the proportions of eyes that had an FTD that was 1.96 SD from the mean FTD of normal eyes were compared to those of normal controls using GEE. Formulas based on GEE were constructed to estimate the Stratus OCT FT from Spectralis OCT FT, and the discrepancies between the predicted and actual OCT FT were presented and compared among groups. The associations between FT and FTD were analyzed, and formulas based on the GEE were constructed for the normal, inner-retinal disease, and exudative AMD groups. A p-value less than 0.05 was considered statistically significant.
Results
The mean age of each group and the number of eyes examined in each group are shown in Table 1. The mean age ± SD of all subjects was 61.5 ± 13.1 years (range, 14 to 88 years). The mean FTD was largest in the exudative AMD group (94.0 ± 55.0 µm), followed by the nonexudative AMD group (75.2 ± 36.2 µm), others (73.9 ± 41.1 µm), ERM (69.2 ± 34.5 µm), normal (66.2 ± 11.7 µm), DR (60.5 ± 37.6 µm), MH (57.2 ± 20.7 µm), RVO (54.5 ± 33.2 µm), and CSC (53.2 ± 23.6 µm) groups (Fig. 2A and Table 2). The mean FTD was greater in the exudative AMD group than in normal controls (p < 0.0001, GEE), but there were no significant differences between the mean FTD of the other retinal diseases and that of the normal group. The coefficient of variation of FTD was largest in the DR group (62.2%) and smallest in the normal group (17.6%) (Table 2).
The proportion of eyes showing FTD values outside of 1.96 SD of the normal control values (FTD >89.0 or <43.3 µm) was greatest in the exudative AMD group (50.0%) and smallest in the macular hole group (18.2%) (Fig. 3). However, no statistically significant difference was found when comparing the proportions among disease groups.
In normal subjects, there were no correlations between FTD and Stratus OCT-measured FT (FTStratus, p = 0.13, GEE) or between FTD and Spectralis OCT-measured FT (FTSpectralis, p = 0.39, GEE). In the inner-retinal disease group, there was no significant correlation between FTD and FTStratus (p = 0.81, GEE), but a statistically significant positive correlation was observed between FTD and FTSpectralis (p = 0.0004, GEE, FTD = 0.10 × FTSpectralis + 25.76). In the exudative AMD group, the correlations of FTD and Modified FTD with FT measured by Stratus and Spectralis OCT were analyzed. There was a statistically significant positive correlation between FTSpectralis and FTD (p < 0.0001, GEE, FTD = 0.53 × FTSpectralis - 67.61), but no significant correlation between FTStratus and FTD (p = 0.59, GEE), between FTStratus and modified FTD (p = 0.26, GEE), or between modified FTSpectralis and modified FTD (p = 0.63, GEE).
Finally, the conversion formulas of FTStratus from FTSpectralis shown in Table 3 and Fig. 4 were statistically significant, except in the nonexudative AMD group. In Fig. 4, the prediction lines of the inner-retinal disease groups were close to that of the normal group, while the exudative AMD group showed a prediction line that deviated most from that of normal subjects and, thus, had the lowest correlation coefficient (0.47). For the exudative AMD group, an additional formula was constructed that considered CNV thickness, which resulted in a correlation coefficient for FTSpectralis (0.79) that was closer to 1.0 than that of the original formula. Fig. 2B shows the averages and SDs of the differences between the FTStratus values calculated by the conversion formulas and the actual FTStratus in each group. The SD was largest in the exudative AMD group (38.6 µm) and lowest in the normal subjects (11.3 µm). The SDs of the differences between predicted FTStratus and actual FTStratus (the right column of Table 3) were smaller than the SDs of the differences in FTDs (Table 2) in each group, except for the MH group. The SD was dramatically decreased by applying the conversion formulas in the exudative AMD group (38.6 µm from 55.0 µm). Furthermore, in the exudative AMD group, the additional conversion formula that considered CNV thicknesses was also applied, and the SD after considering CNV thicknesses (37.2 µm) was slightly smaller than that before considering CNV thicknesses (38.6 µm).
Discussion
OCT imaging currently has a large role in the diagnosis and management of exudative AMD, and it has a significant impact on the management of patients, especially with regard to treatment with anti-vascular endothelial growth factor agents [25]. Despite its use, there is some variation among different OCT systems in how images are captured, quantified, and displayed to the clinician, and these factors may have a significant impact on how OCT data is interpreted, which subsequently affects management decisions [25].
It is well known that Stratus OCT defines the outer retinal border as the complex of the photoreceptor IS/OS junction layer and RPE, while Spectralis OCT selects the Bruch's membrane [12,21]. In patients with exudative AMD, the retinal outer structure can be disturbed by CNV, RPE detachment, subretinal fluid accumulation, intraretinal edema, or fibrotic scars [26]. These retinal morphological changes may make the differentiation of retinal layers by the OCT software more difficult. This may explain why the mean FTD and the proportion of patients with a mean FTD that was 1.96 SDs outside of the mean FTD of normal subjects were greatest in patients with exudative AMD. Likewise, the revised conversion formula for FTStratus for exudative AMD using CNV thickness (Table 3) was well-matched to our expectations of low SDs and higher correlation coefficients, and this can be interpreted to mean that the FTStratus is equivalent to FTSpectralis less the CNV thickness (equivalent to the modified FTSpectralis).
There was a statistically significant positive correlation between FTSpectralis and FTD in the exudative AMD group. However, there was no significant correlation between FTStratus and FTD in that disease group. The higher resolution and accuracy of Spectralis OCT may be the main reasons why this has been shown in previous reports [27,28]. Another explanation is that Spectralis OCT includes CNV during the measurement of FT, and the included CNV thickness should be larger in eyes with large FTSpectralis, which leads to increased FTD with increasing FTSpectralis. This explanation is also supported by the fact that there was no correlation between FTSpectralis and modified FTD (p = 0.63, GEE). Using the Modified FTD formulation, therefore, the FTD can be controlled in the accepted range even in eyes with large FT values. In Fig. 4, the prediction line for exudative AMD shows increasing discrepancy in FTStratus values from the line of normal subjects. This could also be explained by the increasing thickness of CNV in exudative AMD eyes with increasing FTSpectralis.
However, the FTD values of eyes in the inner-retinal disease group were associated with FTSpectralis but not with FTStratus. The better accuracy of Spectralis OCT in delineating retinal borders in eyes with inner-retinal pathology, as well as outer-retinal diseases, may support the positive correlation between FTD and FTSpectralis. The use of the eye tracker when scanning the retina with Spectralis OCT results in a better localization of the fovea and a lower incidence of artifacts than when using Stratus OCT. In summary, FTD values are expected to be greater in eyes with either inner-retinal disease or exudative AMD showing large FT on Spectralis OCT than in eyes with small FT.
In previous studies on diabetic macular edema [21,22], the mean FTDs between the FTs measured by Stratus and Spectralis OCTs were 77.7 and 76 µm, respectively, whereas that of the patients with DR in this study was 60.5 µm. In another study that included eyes with various retinal diseases [20], the mean FTD between the FTs measured by Stratus and Spectralis OCTs was largest (97.1 µm) in CNV (n = 9), followed by 65.3 µm in DR (n = 12), 84.5 µm in ERM (n = 10), and 60.7 µm in RVO (n = 7), which generally corresponded to our results (94.0 µm in Exudative AMD [n = 80], 60.5 µm in DR [n = 127], 69.2 µm in ERM [n = 68], and 54.5 µm in RVO [n = 53]).
In the present study, we constructed conversion formulas that predicted FTStratus from FTSpectralis for each retinal disease group (Fig. 4 and Table 3). The conversion formulas were different among the disease groups and statistically significant, except for eyes with nonexudative AMD. It should be noted that the SDs of the differences between actual FTStratus and predicted FTStratus calculated from FTSpectralis using the conversion formulas (Table 3) were smaller than the SDs of FTD (Table 2). Thus, these formulas can be useful when calculating FTStratus from FTSpectralis according to the corresponding retinal disease, and they may be more precise than considering mean FTD alone, irrespective of the disease diagnosis.
The exudative AMD group showed the most dramatic decrease in the SD of the discrepancy, from 55.0 to 38.6 µm, which indicates that the conversion formula was more accurate in eyes with exudative AMD (Fig. 2B and Table 3). In the exudative AMD group, when CNV thickness was included in the model, the conversion formula showed a correlation coefficient that was closer to 1.0 (0.79) and a smaller SD (37.2 µm) compared to the conversion formula that included FT alone (0.47 and 38.6 µm), which implies that the prediction was more firm after accounting for CNV thickness.
There are several limitations to the present study. Because we included consecutive patients who visited our hospital during the study period, the number of patients and the severity of retinal diseases were not well controlled, which might have influenced the results and statistical significance. Another limitation is that we did not measure the FT of the same eyes with two different SD-OCT devices, and therefore our results cannot be applied to other types of SD-OCT devices. However, from our results, it is expected that the inclusion of CNV in the outer retinal boundary is the most important determining factor for measured FT of eyes with CNV. The segmentation algorithms of OCT devices should be tested when the prediction of FTStratus is required, and there may be less variance in FTD when using OCT devices with segmentation algorithms that are similar to those of Stratus OCT, such as Cirrus HD OCT (Carl Zeiss Meditec).
In conclusion, the differences in the measured FTs between Stratus and Spectralis OCT were not uniform among retinal disease groups and showed large inter-individual variations compared to eyes with normal retinal anatomies, especially in eyes with exudative AMD. Thus, simple adjustments of mean FTD between two OCT devices can lead to incorrect results. Statistically significant conversion formulas could be constructed for different retinal disease groups, and these can be used when predictions of Stratus OCT-measured FT from Spectralis OCT-measured FT are required.






 XML Download
XML Download