

 PDF
PDF ePub
ePub Citation
Citation Print
Print


For blepharoptosis repair, typically a long skin incision is made along the upper eyelid crease, the orbital septum is opened, a dissection is made until the levator aponeurosis is found under the preaponeurotic fat pad, and the levator aponeurosis is sutured to the tarsus at three different positions [1]. However, in 1999, Lucarelli and Lemke [2] introduced a new surgical technique, which enables blepharoptosis repair in patients who had blepharoptosis without dermatochalasis, with an 8 to 10 mm skin incision, exposing the tarsus through the incision and suturing the levator aponeurosis to the tarsus at just one position. After its introduction, this technique has been widely used and shown to be effective in Caucasians [3-6].
When blepharoptosis coexists with dermatochalasis, the typical procedure requires an initial excision of the redundant skin, and the rest of the procedure remains similar to that described above; after the skin excision, an incision is made along the full length of the orbital septum and the levator aponeurosis is fixed on the tarsus at three different positions. Some studies have introduced a surgical technique that is comprised of a modified single suture, instead of the traditional three sutures, for fixing the levator aponeurosis on the tarsus, but the incision is made along the full length of the orbital septum [7-10].
In this study, we describe the technique and results of a modified surgical technique for blepharoptosis repair with excision of the redundant skin, followed by a small incision instead of the traditional long incision to the orbital septum, minimal dissection, and the placement of a single fixation suture between the levator aponeurosis and the tarsus, in patients with ptosis and dermatochalasis.
Materials and Methods
A retrospective review of records from March 2007 to March 2010 included 33 patients (52 eyelids) with unilateral or bilateral involutional ptosis coexisting with dermatochalasis, which was corrected by a small incision in the orbital septum after redundant upper lid skin excision, followed by a single suture, instead of the traditional three sutures, between the levator aponeurosis and the tarsus. Preoperative evaluation included levator function and marginal reflex distances (MRD1). Also, the presence or absence of upper eyelid skin redundancy was checked. The eyelid skin incision was marked along the natural lid crease line and the redundant skin to be excised was designed (Fig. 1A). Local anesthetic infiltration was achieved with 1 to 1.5 mL of 2% lidocaine with 1 : 100,000 units of epinephrine. The skin incision was made using a no. 15 blade and the redundant skin and underlying orbicularis muscle were excised by either Westcott scissors or monopolar cautery (Fig. 1B). The orbital septum was incised at its center for about a length of 10 mm, just above the tarsal plate, and the pretarsal orbicularis muscle was dissected until the tarsal plate was exposed across the same width (Fig. 1C). Dissection was performed in an upward direction from the tarsal plate, the preaponeurotic fat pad was identified, and the levator aponeurosis was exposed until reaching the level of the musculo-aponeurotic junction (Fig. 1D). Next, the levator aponeurosis was released from the underlying Muller's muscle at the upper margin of the tarsal plate. With a double-armed, non-absorbable suture (5-0 nylon or 6-0 silk) a partial thickness suture of more than 5 mm in width was placed through the tarsal plate in a horizontal fashion (Fig. 1E). Next, the suture was passed through the levator aponeurosis at a predetermined position (Fig. 1F). After tying a temporary knot, the eyelid height and contour were examined carefully with the patient in a sitting position, after which the permanent fixation suture was tied down (Fig. 1G). Remnants of the levator aponeurosis below the fixation suture were excised, and then the skin was closed in an interrupted fashion with 6-0 black silk. At this time, a double fold was made by suturing the aponeurosis and subcutaneous tissue only at the medial and lateral edges of the exposed tarsus with 6-0 nylon (Fig. 1H). For all patients, the follow-up period was at least 6 months following surgery, and the outcome measures included the pre- and postoperative MRD1, eyelid contour, postoperative complications, and the need for reoperation. Since it was difficult to accurately assess the abnormality of the eyelid contour during the early postoperative period due to eyelid edema, evaluations were made at 1 month after the operation. When the patient's eyelid contour was considered unsatisfactory, and thus requiring an additional surgery, revision was performed 1 or 2 months after the first surgery. Regardless of the revisional surgery, the success of these patients was also evaluated by their MRD1 values at 6 months after the operation. In patients with unilateral ptosis (Groups I and II), surgery was considered successful when an eyelid symmetry within 1 mm of the contralateral lid height was achieved [11,12]. After surgery for bilateral ptosis, an eyelid position of 2 mm below the superior limbus was considered as the baseline, and based on the criteria of Carter et al. [13], when the upper eyelids were within 1 mm, 1 to 2 mm, and more than 2 mm below the baseline, the outcome was considered as excellent, good, and poor, respectively. In patients with bilateral ptosis (Group III), surgery was considered successful when the grade was excellent or good.
Results
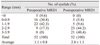
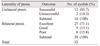
Fourteen male patients and 19 female patients met the eligibility criteria for this study (Table 1). The average age of the 33 patients was 68.4 ± 11.3 years, ranging from 52 to 82 years. The postoperative mean follow-up period was 11.2 months, ranging from 6 to 15 months. The average preoperative levator function was 13.6 ± 4.2 mm, ranging from 9.0 to 17.0 mm. The average preoperative MRD1 was 1.1 ± 0.8 mm, ranging from 1.0 to 2.5 mm. The average postoperative MRD1 measured 2.8 ± 1.1 mm, ranging from 0.5 to 3.9 mm (Table 2). Of the 33 patients, 9 patients (9 eyelids) underwent surgery on one eyelid for unilateral blepharoptosis and dermatochalasis (Group I), 5 patients (5 eyelids) underwent repair of blepharoptosis and dermatochalasis on one eyelid and simple skin excision blepharoplasty of the contralateral eyelid (Group II), and 19 patients (38 eyelids) underwent bilateral blepharoptosis and dermatochalasis repair (Group III). Of the 14 eyelids in Groups I and II that underwent unilateral ptosis repair, 12 eyelids (85.7%) showed a less than 1-mm difference from the contralateral lid, and the ptosis repair was considered successful in these cases. Of the 38 eyelids in Group III that underwent bilateral ptosis repair, 27 eyelids (71.1%), 5 eyelids (13.1%), and 6 eyelids (15.8%) showed excellent, good, and poor outcomes, respectively, of which 32 eyelids (84.2%) with excellent or good outcomes were considered successful. Overall, 44 eyelids (84.6%) out of 52 total eyelids had successful outcomes (Table 3, Fig. 2). As for postoperative complications, 5 eyelids demonstrated peaking or an unsatisfactory lid contour; of these 5 eyelids, 2 eyelids were corrected by the traditional long incision in the orbital septum and placement of three fixation sutures. In the remaining 3 eyelids, the small incision in the orbital septum was widened slightly, either medially or laterally, and they were corrected by re-suturing and placing an additional suture between the levator aponeurosis and the tarsus (Table 4).
Discussion
Involutional ptosis, which is the most common form of acquired ptosis, is caused by stretching or dehiscence of the levator aponeurosis, affecting middle-aged or older patients, and often coexists with dermatochalasis. When blepharoptosis and dermatochalasis coexist, typically, the redundant upper eyelid skin is excised, a full-length incision is made through the orbital septum, dissection is performed to expose the levator aponeurosis and the tarsal plate, and then the levator aponeurosis is sutured to the tarsus at three different positions [7]. Recently, some studies have been performed to revise blepharoptosis surgery in two main areas: first, reducing the incision size and, secondly, reducing the number of sutures used to fix the levator aponeurosis on the tarsus. In 1999, Lucarelli and Lemke [2] reported on the successful repair of ptosis in patients who had ptosis without dermatochalasis by the small-incision technique and placement of a single fixation suture between the levator aponeurosis and the tarsus. Since that time, many surgeons have reported that this technique is simple and effective [3-6]. In patients who have ptosis coexisting with dermatochalasis, excision of the redundant skin is necessary, thereby making a full-length skin incision inevitable. However, minimizing the dissection of subcutaneous tissues reduces the amount of tissue damage and bleeding. In addition, adjusting and fixing the levator aponeurosis on the tarsus at three different positions is very time and labor consuming, and many efforts have been made to simplify this procedure. Liu [8] and Baek et al. [9] reported on a technique that uses a single-suture aponeurotic tuck, Meltzer et al. [10] reported on a technique that uses a single adjustable suture, Jeong [14] reported on a single radial suture technique, and Chang and La [15] reported successful ptosis correction in patients without dermatochalasis by a small cutaneous incision and minimal dissection.
Following this trend, in this study, patients with ptosis and dermatochalasis underwent correction by excision of the redundant skin, a small incision to the orbital septum, minimal dissection, and a single fixation suture between the levator aponeurosis and the tarsus, and successful results were obtained in 84.6% of the operated eyelids. This result is comparable with previously reported success rates of 65% to 90% [10,16-18]. Meltzer et al. [10] performed ptosis repair by a long traditional incision with a 5 to 6 mm wide-bite single adjustable suture. Ninety percent of the patients had a less than 0.5 mm difference in height between the two lids and the remainder had a difference of less than 1 mm. The success rate of this study seems to be higher than that of our surgical technique; however, in their study, an adjustable suture that was adjusted within the first four postoperative days was used, which might explain the relatively higher success rate. McCulley et al. [16] performed levator advancement with a traditional eyelid crease incision with one to three sutures, and 77% had a less than 1 mm difference between upper eyelid heights. Bartley et al. [17] performed levator aponeurosis advancement in patients with acquired unilateral blepharoptosis with one to three sutures, and 65% of the patients were within 1 mm of the height of the contralateral eye. Li et al. [18] performed blepharoptosis surgery and double-eyelid blepharoplasty in patients with latent aponeurotic ptosis with three separate sutures and the reported success rate was 88.2%.
The advantages of this technique are minimal tissue damage, bleeding, edema, and a shorter operation time. However, there are some disadvantages: the minimized surgical exposure limits the removal of the orbital fat, and this technique also requires a more detailed knowledge of the upper eyelid anatomy in order to identify the levator aponeurosis and the tarsal plate [2,3]. In our study, although the sutures for the double fold were only made at the central part of the incision, double folds were well-formed in most patients. We speculated that this was because many patients already had their original double folds before the surgery or that postoperative subcutaneous adhesions along the full eyelid crease incision helped to form double folds.
Repair of blepharoptosis coexisting with dermatochalasis by a small incision to the orbital septum and minimal dissection can be an effective technique, especially in patients with good levator function (of at least 8 mm of levator function), and in patients without previous eyelid surgery. If the levator function is poor, more advancement and upward dissection of levator aponeurosis is required, and this procedure through a small orbital septum incision is rather inconvenient. Also, adhesions due to previous eyelid surgery can make identification and dissection of underlying tissue difficult. Recurrence of ptosis or eyelid contour abnormalities, which can occur due to the use of a single fixation suture, can be prevented by a wide bite suture into the tarsal plate. If peaking or unnatural lid contour does not improve, readjustment or placement of additional sutures after widening the incision could be an effective solution [2,3].
In conclusion, blepharoptosis repair through a small orbital septum incision and minimal dissection can be considered an efficient technique in patients with coexisting ptosis and dermatochalasis.




 XML Download
XML Download