

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Posner-Schlossman syndrome (PSS) is a self-limiting and benign condition characterized by unilateral, recurrent episodes of markedly elevated intraocular pressure (IOP) with mild idiopathic anterior uveitis, open angles, no visual fields defect, and normal optic discs [1]. However, an association between primary open-angle glaucoma (POAG) and PSS, with about 45% of PSS patients having an accompanying POAG, was shown [2,3]. Another complication of PSS, nonarteritic anterior ischemic optic neuropathy (NAION) was also reported [4,5]. We report a case of optic disc pallor which is different from glaucomatous optic neuropathy and NAION occurring after recurrent episodes of marked elevated IOP secondary to PSS.
Case Report
The patient was seen in 1996 at the age of 32, with blurred vision in the right eye and headache. He had no previous medical history, including diabetes and hypertension or trauma history. He was using no systemic medications. His vision was 0.9 in the right eye, 1.0 in the left eye. There was mild epithelial edema of the cornea with a few keratic precipitates and no cells seen on slit-lamp examination of the right eye. The IOP was 60 mmHg in the right eye. Gonioscopy showed an open angle. The left eye was normal. He had five episodes of PSS crises over the next 14 years, with a highest IOP of 60 mmHg. Anterior segment inflammation and elevated IOP were controlled after few weeks of treatment with antiglaucoma medication and topical corticosteroids. This was his treatment course after each PSS event.
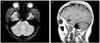
At his first medical examination in 1996, his cup/disc ratio was noted to be 0.4 in the right eye and 0.4 in the left eye. Visual fields were normal (Fig. 1A and 1B). After his fifth attack, in 2010, his uncorrected visual acuity was 1.0 in both eyes and a relative afferent papillary defect of right eye was observed. Color vision was normal. His right optic disc was pale and the field loss in the right eye had progressed to a superior paracentral scotoma (Fig. 2A and 2B). Retinal nerve fiber thickness of the right eye was generally reduced (Fig. 3). There was P100 delay of the right eye in the visual evoked potential test (Fig. 4). There were no abnormal findings on brain magnetic resonance image (Fig. 5).
Discussion
PSS is a syndrome associated with recurrent anterior segment inflammation and elevated IOP. After an attack, IOP and facility of aqueous outflow return to normal. The etiology of PSS is unknown, although abnormal vascular process, autonomic defect, allergic conditions, variation of developmental glaucoma, association of HLA-Bw54, cytomegalovirus, and herpes simplex virus have been suggested [6-8].
There were case reports of PSS and NAION [4,5]. The presumed mechanism causing NAION was decreased perfusion to the optic disc secondary to the rise in intraocular pressure. Risk factors for NAION such as old age, small cup to disc ratio, and hypertension were considered when treating PSS patients.
This is case of optic disc pallor in a patient with recurrent anterior segment inflammation and high intraocular pressure. Optic disc perfusion is directly proportional to mean arterial pressure and inversely proportional to IOP [9]. We had not found something that explained optic disc pallor excluding high IOP. Decreased optic nerve perfusion by recurrent high IOP might induce optic disc pallor.
In conclusion, PSS could cause optic disc changes such as glaucomatous change and ischemic change. Thoughtful attention and aggressive IOP control are required especially in PSS patients with prolonged periods of high intraocular pressure and recurrent attacks.




 XML Download
XML Download