

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Ocular manifestations of Down's syndrome have been well described in numerous studies and include eyelid anomalies such as prominent epicanthal folds, upward slanting of the palpebral fissures, epiblepharon, nasolacrimal duct obstruction, blepharitis, keratoconus, retinal abnormalities, iris abnormality such as Brushfield spots, iris abnormalities, glaucoma, amblyopia due to strabismus, refractive errors, strabismus, and media opacities [1-9]. It is therefore important to recognize these conditions early in the life of these patients, as many anomalies are treatable [4,10].
However, most studies of patients with Down's syndrome have been examined with Caucasian subject populations. Very few reports have addressed the ocular status of Down's syndrome patients in Asian populations [5,8]. Moreover, there are a few detailed descriptions of strabismus or refractive errors in Asian patients with Down's syndrome. This study by a single examiner in patients with Down's syndrome of various ages was designed to survey the clinical characteristics of refractive errors and strabismus in Korean patients with Down's syndrome.
Materials and Methods
One investigator examined 41 Korean patients with Down's syndrome, aged between two and 36 years. These patients were invited to participate in this study through the 2009 Special Olympics in Korea. All patients underwent cycloplegic autorefraction (1% cyclopentolate) and/or retinoscopy, slit-lamp biomicroscopy, and detailed dilated fundus examination. Ocular movements were checked.
Myopia is defined as the spherical equivalent refraction of at least -1.00 dioptors (D), hyperopia as the spherical equivalent refraction of at least +1.00 D, and significant stigmatism as the cylinder of at least 3.00 D. Anisometropia is defined as the spherical equivalent difference of at least 2.00 D between the two eyes of the same patient.
Strabismus was measured using either the prism cover test (for distant and near fixation) or the Krimsky corneal reflex test, depending on the degree of patient cooperation. To assess binocular functions, the Titmus House Fly test was employed. All patients were assessed for accommodative ability, via the following protocol: In cases of any myopia, or hypermetropia ≥2.0 D, the child should wear his/her distant correction glasses. Sitting at a fixed distance of about 50 cm in front of the child, the examiner observed retinoscopic streak light movement while the child gazed straight ahead with both eyes open. A small picture which attracted interest was then introduced approximately 30 cm in front of the child. The child was constantly encouraged to fixate on the near target. If normal accommodation was present, the examiner noted a very distinct shift from "with"-movements to "against"-movements. Such a response was classified as "normal accommodation." If this clear shift did not occur when presented with the accommodative target, the accommodation response was classified as "accommodation weakness." The test was repeated at least three times to ensure consistency of the results.
Concerning esotropia, these patients were specifically examined for any increase in strabismus angle at near fixation compared to distant fixation (if the child co-operated well enough). It was also noted whether or not an increased deviation was observed in connection with increased accommodative demands (fixation on a small picture instead of a light source). These two types of responses were both defined as an "increased near response". In addition, if such an increase was found, care was taken to see if this was counteracted or relieved by a near-addition.
Results
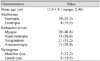
The results of ocular abnormalities found in Korean patients with Down's syndrome are summarized in Table 1.
Refractive error
The prevalences of hypermetropia and myopia were 15 patients (36.6%) and 20 patients (48.8%) respectively. High myopia (>-6.00 D) was detected in three patients (7.3%), and these patients revealed no strabismus. Significant hypermetropia (>3.00 D) was detected in nine patients (22.0%), all of whom exhibited esotropia. Astigmatism was detected in 21 patients (51.2%), with significant astigmatism (≥±3.00 D) detected in seven patients (17.1%). Ansiometropia ≥1.00 D was detected in 11 patients (26.8%), and anisometropia ≥2.00 D was detected in six patients (14.6%).
Strabismus
Strabismus was observed in 18 patients (Table 2). Esotropia was identified in ten patients (24.4%), and exotropia in eight patients (19.5%). The most frequently detected type of esotropia was acquired non-accommodative esotropia (seven of ten patients with esotropia), and the most common type of exotropia was also the basic type (five of eight patients with exotropia). The mean deviation amount of esodeviation was 40 (range, 16 to 70 years) prism diopters, and the magnitude of the exotropia was 30 (range, 18 to 50 years) prism diopters.
Refractive state: correlation to esotropia
Patients with esotropia had refractive errors of +4.89 D (±3.73) and patients with exotropia had refractive errors of -0.31 D (±1.78). Nine of the ten patients with esotropia also evidenced significant hyperometropia (>+3.00 D). Three of these exhibited a high degree of hyperometropia (>6.00 D) with esotropia. However, 23 patients without strabismus had refractive errors of -0.52 D (±2.55).
Accommodative ability
Six of the 18 patients with strabismus had an accommodation weakness. All of these patients belonged to the acquired esotropia group. Five of these patients had esotropia associated with hypermetropia. In the non-strabismus group (n = 23), five patients had evidence of an accommodation weakness. The difference in the presence of accommodation weaknesses between the strabismus and non-strabismus group could not be statistically compared due to the small number of subjects.
Discussion
A strabismus frequency of 43.9% among Down's syndrome patients correlates well with the results of previous studies [4-8]. A previous report concerning Korean patients with Down's syndrome has documented that esotropia is rather common and that the mean prevalence of exotropia is somewhat higher than that of other previous studies [8]. In this study, esotropia was the most frequently detected type of strabismus, and the prevalence of exotropia was 19.4%. These findings reflect a much higher prevalence of exotropia than was previously reported [4-8] which likely reflects ethnic differences. Our study demonstrated that esotropia is more common than exotropia and that myopia is more common than hypermetropia in Korean patients with Down's syndrome.
In six of seven patients with acquired esotropia, significant hypermetropia was detected (mean +3.55 ± 2.54 D). Esotropia occurred with lower frequency in the low-grade hypermetropia group than in the other group. Thus, in addition to the well-known general correlation between hypermetropia and esotropia, our study results demonstrate that Down's syndrome patients with stable refractive values around emmetropia or low-grade hypermetropia appear to be less likely to develop esotropia.
Six of 15 patients with hypermetropia demonstrated weak accommodation, enhancing the effect of the hypermetropic refractive error. Hypoaccommodation has generally been recognized as a well-known mechanism of convergence excess esotropia in mentally normal individuals [10]. The increased accommodative effort exerted when attempting to compensate for the accommodation weakness results in esotropia. Although this hypoaccommodation convergence excess could be regarded as a specific entity occurring in normal populations, a materially similar explanation may make sense for Down's syndrome patients with accommodation weakness and esotropia. In particular, the group of five children with esotropia, accommodation weakness, and an "increased near response" parallels very closely the description of hypoaccommodative convergence excess. Although there must apparently be additional contributing factors, we agree with Haugen and Hovding's opinion [6] that accommodation weakness is one such factor in esotropia occurring in Down's syndrome.
It is quite difficult to evaluate binocular functions in Down's syndrome patients who cooperate poorly as the result of intellectual disability. Currently, only limited information is available regarding binocular potential in Down's syndrome patients. However, Haugen and Hovding [6] also reported that 44% of the children with strabismus provided a clearly positive response to the stereo test, and 40% of all the children with acquired esotropia evidenced good binocular sensory functions. This should encourage our efforts toward the early tracing and treatment of refractive errors and accommodation weakness.
Several reports have suggested that bifocals are an effective method to correct reduced accommodation in children with Down's syndrome [11,12]. Bifocals confer benefits to Down's syndrome children with accommodation weaknesses, both directly (better focusing through the bifocal) and indirectly (by encouraging improved accommodation through the distance part of the lens) [11,12]. Stewart et al. [11] have suggested that bifocal spectacles can be prescribed to Down's syndrome children as an active treatment for their reduced accommodation response, with a success rate of over 60%.
The first limitation of our study is that it was a non-comparative, cross-sectional study, not a longitudinal study. Another limitation of this study is that our subjects were recruited from the Special Olympics of Korea, and thus our results may not be representative of the general population with Down's syndrome. However, our study by a single examiner in patients with Down's syndrome of various ages (2 to 36 years old) is quite novel. Our findings make sense in terms of accommodation weakness as well as hyperopic errors of Down's syndrome, which are associated with the occurrence of esotropia. Due to the limited number of patients examined in this study, caution should be exercised before drawing any broad conclusions. Nevertheless, hypermetropia and accommodation weakness are likely important factors in esotropia in Down's syndrome patients. Based on the results of this study, eye examinations of Down's syndrome patients should routinely include a measure of accommodation at near, and bifocals should be considered for those who evidence under-accommodation.

 XML Download
XML Download