

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Ophthalmic artery obstruction and central retinal artery obstruction (CRAO) and their serious visual adverse effects following cosmetic surgery are very rare, however they are potentially devastating. A periocular autologous fat injection can not only lead to visual complications, but may also cause brain and facial skin damage, as seen in this case. We report a case of ophthalmic artery obstruction and brain infarction with resulting facial skin damage. Ophthalmic artery obstruction was confirmed by fluorescein angiography and brain infarction was confirmed by magnetic resonance imaging (MRI).
Case Report
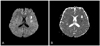
A 44-year-old woman was referred to our hospital from a local clinic for decreased visual acuity in her left eye. Two hours before the manifestation of symptoms, an autologous fat injection was administered in the periocular area under intravenous anesthesia. The autologous fat was obtained from the abdominal area and the procedure was performed by a local plastic surgeon. When the effect of the anesthesia wore off, the patient reported a loss of vision in the left eye. The best corrected visual acuity was 1.0 in the right eye and no light perception on the left side. The left pupil was dilated and a relative afferent pupillary defect was detected. During physical examination, the patient suddenly complained of dysarthria and the skin color of the nose changed to purple (Fig. 1). The patient was immediately transferred to the emergency room and neurological examination, blood tests, and an MRI scan of the brain were performed. Within 30 minutes, the dysarthria improved significantly and the patient was able to speak normally. On examination, the right fundus appeared to be normal but the left showed a cherry red spot with visible emboli in several retinal arteries (Fig. 2A and 2B). Fluorescein angiography of the left eye revealed markedly prolonged choroidal filling around the optic disc and a delay in retinal arterial filling while that of the right eye revealed no abnormalities (Fig. 3A and 3B). The results of laboratory examinations were normal, however the MRI scan showed an ill-defined hyperintense lesion at the left insular cortex (Fig. 4A and 4B). The patient was finally diagnosed with ophthalmic artery obstruction and left middle cerebral artery infarction. The patient was promptly administered ocular massage, intravenous mannitolization, and oxygen and carbon dioxide therapy. Twenty-four hours after autologous fat injection, the left fundus exhibited marked retinal edema and multiple fat emboli and the visual acuity of the left eye was no light perception (Fig. 2C). At 2 months after the injection, the patient had no perception of light in the left eye and the left fundus showed optic atrophy, multiple retinal hemorrhages, and a fibrous change on its posterior pole (Fig. 2D).
Discussion
Retinal artery occlusion is usually associated with a sudden and profound loss of vision. Although it is especially common in atherosclerotic carotid artery diseases, retinal artery occlusion secondary to fat embolization is also a recognized, although uncommon, complication of autologous fat injection. Several reports have been published regarding iatrogenic retinal artery occlusion caused by retrobulbar corticosteroid injections [1], intranasal corticosteroid injections [2], and autologous fat injections into the glabellar region [3-5]. A retinal artery occlusion that is caused by autologous fat and that does not respond to thrombolytic agents is associated with a poorer prognosis than if caused by atherosclerotic disease [6]. Patient received an injection of autologous fat into the periocular area and then developed ophthalmic artery obstruction and left middle cerebral artery infarction. Ophthalmic artery obstruction was diagnosed by fluorescein angiography. In cases of CRAO, fluorescein angiography usually shows delays in both retinal arterial filling and retinal arteriovenous transit time with normal choroidal vascular bed filling. A markedly prolonged choroidal filling in the presence of a cherry red spot should arouse suspicion of an ophthalmic artery obstruction [7]. Some studies regarding iatrogenic CRAO report that vascular disturbances after direct injection of foreign material into a branch of the ophthalmic artery occur because of retrograde flow of an intra-arterial injection into the central retinal artery [1-4]. We presume that the ophthalmic artery obstruction in this case developed via a similar mechanism. The foreign material was injected into one of the peripheral branches of the ophthalmic artery and the force of the injection was sufficient to thrust the emboli into the left middle cerebral artery via the internal carotid artery. The skin lesions indicated that the distal arterial branches, which supply blood to the nose, were also occluded.
Our case is not the first report of ophthalmic artery occlusion with cerebral infarction after fat injection into the face. However, our case is distinct from others in that visual loss preceded neurologic symptoms and skin damage by about two hours. Therefore, we should pay special attention to each patient's neurologic status and not delay imaging studies of the brain if visual loss or relative afferent pupillary defects are detected after fat injection into the face. There has also been a report of optic nerve infarction after autologous fat transplantation that was confirmed by diffusion-weighted MRI [8]. Consequently it is recommended that orbital MRI is performed as well as brain MRI with diffusion-weighted imaging.
This case indicates that cosmetic plastic surgeons and ophthalmologists should be careful while administering periocular autologous fat injections. Fat injections should be performed slowly and with the lowest possible pressure. Injection fillers with blunt needles may be the most appropriate choice [6]. However, because the peripheral arteries of the face are small and collapsible, during aspiration blood may not appear in the delivering syringe despite entry of the needle into an arterial lumen [4]. Therefore, the risk of visual loss and even brain damage should be explained to the patient prior to the procedure.



 XML Download
XML Download