

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Valsalva retinopathy, first described by Duane in 1972, is caused by a sudden increase in intra-thoracic or abdominal pressure. Most cases have been reported to follow a benign course where the visual acuity is recovered as the hemorrhage is absorbed.1
Valsalva retinopathy may occur during various activities, including aerobic excercise,2 excessive sexual intercourse,3 blowing a bubble,4 prostate surgery,5 dental surgery,6 vomiting, as a result of constipation in pregnant women,7 carrying heavy loads, receiving endotracheal intubation, severe coughing,8 colonoscopy,9 and LASIK surgery.10 In Korea, valsalva retinopathy has been reported to occur as a result of lifting a barbell,11 blowing into a rubber glove,12 and strenuous exercise.13
Case Report
A 17-year-old man presented to us with a chief complaint of the sudden onset of decreased visual acuity, accompanied by central scotoma, which developed in the left eye. There was no significant past medical or surgical history. No relevant ophthalmologic history was noted. At the time of initial diagnosis, the corrected visual acuity was 20/20 in the right eye and 20/100 in the left eye. Intraocular pressure was 13 mmHg bilaterally. A slit lamp exam demonstrated no significant findings in the anterior segment including the cornea, anterior chamber, and anterior vitreous body.
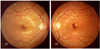
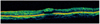
On fundoscopy, there was a dumbbell-shaped macular bleed with a well-defined margin in the left eye (Fig. 1). Optical coherence tomography demonstrated that a highly reflective shadow was present in the macular area (Fig. 2). There was nothing unusual in the patient history other than a recent oratorical contest. The clinical course was closely monitored, and drug therapy was initiated.
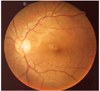
One month after presentation, the patient had an improved uncorrected visual acuity of 20/20 in the right eye and 20/25 in the left eye. On fundoscopy, the pre-retinal bleeding observed at the time of initial diagnosis had resolved (Fig. 3). Fluorescein angiography demonstrated no significant findings (Fig. 4).
Discussion
The Valsalva maneuver decreases venous return to the heart by exhaling against a closed glottis; this leads to an increase in abdominal and intrathoracic pressures. The decreased venous markedly lowers cardiac output. Inspiration with a closed glottis increases venous return. This markedly increases the cardiac output within several minutes, thus increasing arterial pressures.1
The venous system of the head and neck lack a functional valvular system. Therefore, if abdominal or intrathoracic pressures are suddenly raised with a closed glottis, this pressure increase would be directly transferred to the vascular system of the head and neck.
This increase in arterial pressure has effects on the eye. A marked increase in intraocular pressure provokes spontaneous rupture of capillary vessels surrounding the central fossa. This can result in a loss of visual acuity in otherwise healthy eyes.14 The resulting retinal hemorrhage spontaneously resolves within several weeks to several months in most cases and is not accompanied by notable complications.15
In the current case, retinal bleeding occurred in a 17-year-old man who had no significant past history, immediately following an oratorical contest. Presumably, an excessive amount of oration caused a sudden increase in venous pressure, resulting in valsalva retinopathy.

 XML Download
XML Download