

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The changes in astigmatism which occur after cataract surgery with suture placement are different from those in surgery without suture placement (self-sealing incision).1-3 In cataract surgery with suture placement, surgeons should consider suture-induced astigmatism and the effects of suture removal, as well as incision-induced astigmatism.
Various modulations have been undertaken to reduce postoperative astigmatism.4,5 Aside from modulations which vary incision length and location, corneal incisional tunnel length can be a factor in reducing postoperative astigmatism. In sutured surgery, suture removal is an another factor that needs to be considered when attempting to reduce astigmatism. The effects of these modulations may be different in the preoperative astigmatism axis-stratified group.
We evaluated the effects of preoperative astigmatism and corneal incisional tunnel length on postoperative astigmatism. We also evaluated the effects of preoperative astigmatism, corneal incisional tunnel length, postoperative astigmatism, and the time to suture removal in post-suture removal astigmatism.
Materials and Methods
We performed a retrospective chart review of 130 eyes in patients who underwent uneventful phacoemulsification cataract surgery between September 2007 and September 2008.
Exclusion criteria included previous ocular surgery, traumatic cataract, pterygium, surface irregularities, unreliable keratometric readings, and connective tissue disorders.
Complete ophthalmologic evaluations were performed preoperatively, one month postoperatively, and one month after suture removal. Suture removal was attempted within the one month postoperative follow-up period; however some patients were lost to follow-up during that time.
We collected data regarding sex, age, and automated keratometry before surgery at one month postoperatively and at one month after suture removal. We also recorded the corneal incision tunnel length (measured with calipers during surgery) and the time to suture removal. Although postoperative changes in astigmatism are known to occur even in the late postoperative period,6 we assumed a one-month window was sufficient for evaluating early postoperative changes.7
Surgical method
All surgeries were performed by a single surgeon using a divide-and-conquer technique and retrobulbar anesthesia. A 3.2 mm clear corneal incision was made approximately 0.2 mm anterior to the edge of the limbal vessels. The axis of the incision and suture was approximately 105 degrees (superotemporal in right eyes and superonasal in left eyes) in all eyes. A shallow precut was made, after which lamellar dissection was performed to create a corneal tunnel. A stab incision was then made. The wound length was measured with calipers to ensure that the proper intracorneal tunnel length was achieved. Several factors can affect the tunnel length including the sharpness of the blade, the angle of blade approach, and the thickness of the corneal tissue.8,9
After the phacoemulsification and cortex removal were completed, an acrylic intraocular lens (IOL) was inserted. At the conclusion of the surgery, a single 10-0 nylon suture was placed radially with simple apposition of the wound, without tension or gaping.
Astigmatism analysis
The preoperative astigmatisms were divided into four groups according to the differences between the preoperative astigmatism axis (flattest axis) and the incision axis (105 degrees) as follows: Group I, 0 ≤ absolute value of the difference ≤ 15 degrees; Group II, 15 < absolute value of the difference ≤ 45 degrees; Group III, 45 < absolute value of the difference ≤ 75 degrees; and Group IV, 75 < absolute value of the difference ≤ 105 degrees (Fig. 1). Therefore, an incision made at 105 degrees in Group I was an incision made at the flattest meridian. On the other hand, an incision made at 105 degrees in Group IV was an incision made at the steepest meridian. We analyzed the magnitudes and axes of the induced astigmatisms after surgery and after suture removal in each preoperative astigmatism axis-stratified group (Groups I, II, III, and IV).
The four variables for the magnitude and axis were defined as follows:
The values of these four variables were calculated using subtraction as follows:
POCAXIS=the absolute value of (postoperative astigmatic axis - preoperative astigmatic axis)
PSCAXIS=the absolute value of (post-suture removal astigmatic axis - postoperative astigmatic axis)
POCMAGNITUDE=the dioptric power of (postoperative astigmatism magnitude - preoperative astigmatism magnitude)
PSCMAGNITUDE=dioptric power of (post-suture removal astigmatism magnitude - postoperative astigmatism magnitude).
In order to evaluate the factors which only affected the magnitude of the astigmatism and not the axis, we excluded data which showed an axis shift (45 < POCAXIS ≤ 135 degrees, or 45 < PSCAXIS ≤ 135 degrees). The group without axis shift was named GroupWAS. We analyzed the factors which affected postoperative astigmatism and post-suture removal astigmatism in each GroupWAS (Group IWAS, IIWAS, IIIWAS, and IVWAS).
A keratometric cylinder was used for analysis (RK-F1; Canon,Tokyo, Japan). The axis of astigmatism does not have a significant influence on visual acuity.10-13 Because of this, our study did not use vector analysis. Instead, we calculated changes in the magnitude of astigmatism without regard to the axis using simple subtraction of each value.10-13 Changes in the astigmatism axis were calculated using subtraction of each value. The absolute value of the net change was then used.
Data were analyzed using SPSS ver. 1.5 (SPSS Inc., Chicago, IL, USA). Multiple regression analysis was used to determine changes in the absolute values of the postoperative astigmatism compared to the preoperative astigmatism and corneal incisional tunnel length in each GroupWAS. Multiple regression analysis was also used to determine changes in the absolute value of post-suture removal astigmatism compared to the absolute value of preoperative and postoperative astigmatisms, corneal tunnel length, and time to suture removal in each GroupWAS. Variables were selected by the "enter" method of the program. A logistic regression model was used to identify variables that were associated with the prevalence of postoperative astigmatism axis shift and post-suture removal axis shift.
Results
Changes in the magnitude and axis of corneal astigmatism in the four groups
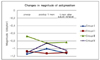
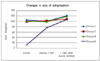
Figs. 2 and 3 show the changes in the magnitude and axis of the mean preoperative corneal astigmatism one month postoperatively and one month after suture removal in the four groups.
Table 1 compares the changes in the magnitude and axis of astigmatism after cataract surgery and suture removal in the four groups. There was a significant postoperative axis change (POCAXIS) in Group IV. This indicates that the significant postoperative axis changes occurred when the incision and suture were located on the steepest meridian (p < 0.05).
Table 2 shows the frequencies of the postoperative axis shift and post-suture removal axis shift in the four groups. There were no differences in the frequency of axis shift among the groups (p > 0.05).
Variables which affected the degree of postoperative astigmatism and post suture removal astigmatism in the four GroupsWAS
We used a multiple linear regression model to evaluate the impact of various risk factors on the absolute values of postoperative astigmatism and post-suture removal astigmatism in each GroupWAS. A test for multicolinearity was conducted prior to the selection of these variables.
In Group IWAS, we evaluated the impact of various risk factors on the absolute values of the postoperative astigmatism. Table 3-1A shows an increase in the absolute value of postoperative astigmatism as the absolute value of preoperative astigmatism increased (p=0.006). There was also an increase in the corneal tunnel length (p=0.02). We evaluated the impact of various risk factors on the absolute value of post-suture removal astigmatism. Table 3-1B shows an increase in the absolute value of post-suture removal astigmatism as the absolute value of postoperative astigmatism increased (p=0.048). There was also a reduction in the absolute value of post-suture removal astigmatism associated with a later suture removal time (p=0.002).
In Group IIWAS, we evaluated the impact of various risk factors on the absolute values of postoperative astigmatism. Table 3-2A shows an increase in the absolute value of postoperative astigmatism as the absolute value of preoperative astigmatism increased (p=0.006). We evaluated the impact of various risk factors on the absolute values of post-suture removal astigmatism. Table 3-2B shows a reduction in the absolute value of post-suture removal astigmatism that was correlated with later suture removal time (p=0.015).
In Group IIIWAS, we evaluated the impact of various risk factors on the absolute values of postoperative astigmatism. Table 3-3A shows an increase in the absolute value of postoperative astigmatism as the absolute value of preoperative astigmatism increased (p=0.003). There was also a reduction in postoperative astigmatism that was associated with an increase in the corneal tunnel length (p=0.001). We evaluated the impact of various risk factors on the absolute value of post-suture removal astigmatism. However, Table 3-3B shows that no significant correlations were found.
In Group IVWAS, we evaluated the impact of various risk factors on the absolute values of postoperative astigmatism. Table 3-4A shows a reduction in the absolute value of postoperative astigmatism as the corneal tunnel length increased (p=0.00). We evaluated the impact of various risk factors on the absolute value of post-suture removal astigmatism. Table 3-4B shows an increase in the absolute value of post-suture removal astigmatism as the absolute value of postoperative astigmatism increased (p=0.01). There was also an increase in the absolute value of post-suture removal astigmatism that correlated with later suture removal time (p=0.00).
Variables associated with the prevalence of the postoperative axis shift and post-suture removal axis shift
We used a logistic regression model to identify the variables that were associated with the prevalence of the postoperative astigmatism axis shift and post-suture removal axis shift.
Results of the logistic regression analysis that was used to identify the variables which were associated with the prevalence of the postoperative axis shift are shown on Table 4. The variables included in the analysis were not significant.
Logistic regression analysis identified variables that were significantly associated with the prevalence of post-suture removal axis shift (Table 5). The odds for a post-suture removal axis shift decreased with a shorter corneal tunnel length (less than 1.5 mm). The odds for an axis shift increased with early suture removal (before one month postoperatively) and with a low absolute value for the magnitude of postoperative astigmatism (POABS · MAGNITUDE < 1.00 D).
Discussion
Cataract surgery has been transformed into a true refractive surgical procedure.4 To improve uncorrected visual acuity (UCVA), one must not only deal with spherical ametropia, but also with astigmatism. The corneal component of astigmatism depends on various factors, such as the type and location of the surgical incision, the suturing material used, suture placement, and the postoperative use of steroids.1,4 Some options exist for modulating astigmatism during cataract surgery. These options include creating an incision to reduces preexisting astigmatism through manipulation (location, length, and construction) and concomitant incisional surgery.4,5,13 Although the correction of more severe astigmatism requires additional intervention (limbal relaxing incisions, arcuate keratotomies, or toric IOLs), mild to moderate corneal astigmatism can be corrected or improved by modifying the parameters of the incision (length, distance from the corneal center, and the corneal meridian, e.g., on-axis incision).6
Incision locations include the 12 o'clock position, between the 9 and 12 o'clock positions, and at the temporal and steep meridians. Incision location can have a dramatic influence on the astigmatic effect. In clear corneal surgery, placement of the incision on the steep axis, whether superiorly, temporally, or obliquely, can help to reduce the astigmatism within the meridian.4 However, the induced astigmatic effect is different between temporal and superior incisions.4,14 Oblique incisions have been shown to have an intermediate effect.4 The reasons behind these effects have not yet been explained.4,15,16 The typical human cornea is approximately 1 mm wider than it is tall. A superior incision may be slightly closer to the corneal apex than is a temporal incision. This could cause it to have a greater effect on the central corneal curvature. The distractive forces of blinking and gravity may account for the differences in the superior and temporal wounds. It is also possible that there are differences between the tissues of the superior and temporal cornea and that of the limbus. It is not known if wound healing in the temporal cornea differs from that in the superior cornea.
An on-axis clear corneal incision is another approach which attempts to reduce preoperative astigmatism. With this technique, it is vital that the astigmatism meridian be identified preoperatively and that the surgical incision used for flattening the steeper corneal meridian be placed exactly on that meridian.6,17
If the clinician wishes to avoid changing the position of the microscope and phacoemulsification machine, he or she could attempt an oblique incision. This can happen when the surgeon is sitting at the patient's head during the procedure, as in our study. An incision performed horizontally at 180 degrees provides comfortable access to both eyes. Thus, for a right-handed surgeon who is sitting at the head of the patient, the horizontal incision is superonasal in the left eye and superotemporal in the right eye.18
When the incision was located obliquely between the 9 o'clock and 12 o'clock positions, the magnitude of the astigmatism was significantly smaller and more stable than that seen in conventional superior incisions.19 These findings suggest that corneal astigmatism after cataract surgery is affected by the mechanical forces of the eyelid and extraocular muscles.19
The magnitude of preoperative astigmatism can affect postoperative astigmatism. One study reported that no eye with a preoperative astigmatism of 1.2 diopters or greater became astigmatism-free postoperatively, even when the surgeons attempted to modulate the astigmatism through different incision locations. These results were found even when the incision was made at the steepest meridian.19 However, another study reported that higher degrees of preexisting astigmatism were associated with a greater effect from modulating the incision size.4 In our study, the magnitude of the preoperative astigmatism affected the magnitude of the postoperative astigmatism in Groups IWAS, IIWAS, and IIIWAS (p < 0.05, Table 3-1A, 3-2A, 3-3A, respectively). A larger magnitude of preoperative astigmatism was associated with a larger magnitude of postoperative astigmatism. This indicates that incisions other than those in the steepest meridian (Group IVWAS) have little modulating effect on astigmatism in patients who have a large preexisting astigmatism. For the post-suture removal astigmatisms in Groups IWAS and IVWAS, the magnitudes of the postoperative astigmatism affected the magnitude of the post-suture removal astigmatism (p <0.05, Table 3-1B, 3-4B, respectively). A larger postoperative astigmatism was associated with a larger post-suture removal astigmatism. In our study, the magnitude of the preoperative astigmatism did not effect the magnitude of the post-suture removal astigmatism.
Some studies have found a distinct difference between the right and left eyes. However, other studies have found no differences in the amplitude of flattening between the right and left eyes.18,20-22
The architecture and construction of the wound can also have an influence on its astigmatic effect.4 Single-plane incisions are the most astigmatically neutral, especially when made in the horizontal meridian. Grooved incisions have architectural characteristics similar to those seen in transverse relaxing keratotomy. Because of this, they have a greater astigmatic effect compared to single-plane incisions.4 Axis shift does not always reduce the visual acuity of the patient.
There is debate as to which type of astigmatism, if any, is preferable after cataract surgery. Some researchers believe that with-the-rule astigmatism gives a better range and depth of vision and is better tolerated visually.4 Others believe that low myopic against-the-rule astigmatism provides better near UCVA compared to an equal amount of with-the-rule astigmatism.4 If the magnitude of astigmatism is significantly reduced, the patient's visual acuity could improve, even if axis shift occurs. However, it is generally accepted that reducing astigmatism without significantly changing the axis is well tolerated and should be the goal. Overcorrection, with a resultant 90-degree axis shift, is not as well tolerated.
Tejedor and Murube,23 in a study of patients with a steep corneal axis between 70 and 110 degrees, recommended at least 1.5 diopters of corneal astigmatism in a superior incision in order to avoid a shift 90 degrees away from the steep axis. Seventy-five percent of patients who had a steep axis of corneal astigmatism at 180 degrees and who underwent surgery through a temporal incision for an astigmatism axis shift of 90 degrees were found to have a preoperative astigmatism magnitude of less than 0.75 diopters.
In our logistic regression model, we could not determine if preoperative astigmatism was associated with the prevalence of postoperative axis shift or with post-suture removal axis shift. However, the following factors were found to be significantly associated with post-suture removal axis shift: long corneal tunnel length, low magnitude of postoperative astigmatism, and early suture removal.
The suture technique and material can also have an effect on astigmatism after cataract surgery. Suture technique is dependent on incision size and location.
Current phacoemulsification techniques include singlestitch and sutureless closures. Small incision cataract surgery induces less astigmatism, and the no-stitch technique seems to offer several advantages.2 Small, unsutured clear corneal incisions are preferred by many cataract surgeons in the setting of phacoemulsification. If a no-suture technique is used, meticulous wound construction must be pursued to achieve a watertight wound with no gaping.24,25 However, an increased incidence of endophthalmitis has been associated with sutureless closures.24-26 Some studies have strongly suggested that optimal protection against endophthalmitis is achieved when the wound is closed with a suture.25 There may be some differences in the development of astigmatism between sutured and non-sutured wounds. Some studies have shown that sutured wounds on the steep meridian can initially steepen that meridian. In contrast, non-sutured wounds on the steep vertical meridian can flatten it.3 Other studies have shown that a single leakage-preventing suture does not affect corneal topography or visual recovery.27 In addition, the suture depth and length can affect the development of astigmatism. In this study, because all of the sutures were performed by the same surgeon, we assumed that the effect of these factors would be minimal.
Traditional radial suture closure induces significant with-the-rule cylinder changes because of the radial tension vector of the suture, although this effect will decrease with time.2,10 Although there is concern about increased endothelial cell loss and potential visual complications with approaches closer to the visual axis, incisions that are closer to the central cornea have a greater astigmatic effect.4 There are no reports to date which suggest that corneal tunnel length can affect postoperative astigmatism. However, we observed the different effects of corneal tunnel length on the magnitude of postoperative astigmatism in each group. A long corneal tunnel does not necessarily mean that the incision is in proximity to the visual axis. The internal opening of an incision may be closer to the visual axis, while the external opening that affects the astigmatism does not change.2 Hence, the mechanism behind the effect of variable corneal tunnel length on astigmatism may be different from the mechanism associated with varying the proximity of the incision to the visual axis.
Although we intended to suture without tension or gaping, short tunnel incisions required somewhat tighter sutures to prevent wound leakage. Such sutures induced larger with-the-wound cylinder astigmatism changes compared to long tunnel incisions within the incisional meridian. Because Groups IIIWAS and IVWAS were characterized by incisions on the steep meridian, the shorter tunnel wound sutures may have induced larger with-the-wound astigmatisms, although the incision on that meridian had initially flattened it. We assumed that the flattening effect of the incision would be almost the same irrespective of tunnel length because the external opening that affects astigmatism2 was placed at the same location, approximately 0.2 mm from the limbus. Although the incision further flattened the flat meridian in Group IWAS, the shorter tunnel could have reduced the flattening effect of the incision after the suturing was completed.
When a surgeon attempts any sutured incision, he or she must consider the risk of developing suture-induced astigmatism, as well as the effects of suture removal and surgically-induced astigmatism.
Suture-induced astigmatism arises from suture tension, tissue edema, and underlying surgically-induced astigmatism. However, surgically-induced astigmatism results primarily from the incision, its realignment, and wound healing.28
If the intent is to routinely remove the suture in order to lower the risk of developing suture-related postoperative complications,29 the surgeon must consider when to remove the sutures after the surgery.
In the natural course of corneal astigmatism following cataract surgery (conventional extracapsular cataract extraction with large superior incision and four sutures), most patients develop against-the-rule astigmatism during the late postoperative period. Greater with-the-rule astigmatism is desirable in the early postoperative period.7 Talamo et al.7 suggested that it might be unwise to cut the sutures in patients with early postoperative astigmatism of less than 3.0 diopters because of the instability of the corneal astigmatism. In our study, different time points were required to reduce the post-suture removal astigmatism in each GroupWAS. Late suture removal was associated with a decrease in the magnitude of postoperative astigmatism in Groups IWAS and IIWAS. Early stitch-out was associated with a decrease in the magnitude of postoperative astigmatism in Group IVWAS. According to the logistic regression model, early suture removal may be a risk factor for post-suture removal axis shift.
Based on the results of our study, we recommend a short corneal tunnel and a late suture removal in patients with Group IWAS characteristics, a late suture removal in Group IIWAS-like patients, a long corneal tunnel in Group IIIWAS-like patients, and a long corneal tunnel and an early suture removal in patients with Group IVWAS characteristics. The prevalence of post-suture removal axis shift was increased in the longer tunnel group, in the low magnitude of postoperative astigmatism group, and in the earlier suture removal group.
Corneal incision location and length are known to modulate preexisting astigmatism. However, our research indicated that in sutured surgery, corneal tunnel length may also be an important factor in reducing early postoperative astigmatism. Our research also indicated that in sutured surgery, the time of suture removal may be an important factor in reducing early post-suture removal astigmatism.
Variability in the response of corneas to cataract incisions, individual variations in wound healing, and the elastic properties of the cornea are well known factors that decrease the predictability of surgical outcomes.23 The patterns of astigmatism change in this study may differ from the cases conducted by other surgeons using other techniques and other incision locations. With accompanying individualized analysis, adequate incisional tunnel length and correct suture removal timing according to the preoperative axis of astigmatism may improve surgical results.






 XML Download
XML Download