

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Ablative laser skin resurfacing with either a carbon dioxide (CO2) or erbium:yttrium-aluminum-garnet laser is a well-accepted treatment modality for facial rejuvenation. Complete epidermal ablation with these systems results in loss of barrier function and an extended recovery period. Patients undergo prolonged erythema, pigmentary alteration, infection and in rare cases, fibrosis.1,2 Because of these potential risks, nonablative technology was developed as a safe alternative to ablative technology for creation of a controlled thermal injury to the dermis with subsequent neocollagenesis and remodeling of scarred skin, but the technique has limited efficacy.3 Fractional photothermolysis (FP) was recently developed as a safe and effective treatment modality. Fractional photothermolysis induces multiple noncontiguous arrays of thermal injury to create unique damage patterns called microthermal treatment zones (MTZ) and characteristically spares the tissue surrounding each MTZ.4 Because the tissue surrounding each MTZ is intact, healing is rapid due to the residual viable epidermal and dermal cells. The depth of penetration of each MTZ is energy-dependent and can be tailored to the characteristics of the treatment area and even more appropriately tailored to the condition being treated within the same anatomic region (i.e., deeper for acne scarring and more superficial for pigmentation).4 Histologic evaluation of the MTZ demonstrates homogenization of the dermal matrix and formation of microscopic epidermal necrotic debris, which represent the extrusion of damaged epidermal components by viable keratinocytes at the lateral margins of the MTZ.5 The stratum corneum remains intact during this process, thereby maintaining epidermal barrier function.4
Although there have been some reports of successful treatment of fine and moderate wrinkles using FP technology,4,6-8 there are few prospective studies in Asians. Recently, this laser technique was shown to be safe for treating melasma, acne scarring and striae in Asian skin.9,10 The purpose of this study was to evaluate the safety and efficacy of FP in the treatment of facial wrinkles in Asians.
Materials and Methods
Twenty-five patients (two men and 23 women) with Fitzpatrick skin type III-IV were enrolled in this study. Their ages ranged from 27 to 61 years (mean, 45 years). This prospective study was performed in accordance with the ethical guidelines and complied with the policies of the local institutional review board. Written informed consent was obtained from each patient. Exclusion criteria included known photosensitivity, immunocompression, pregnancy or lactation, history of hypertrophic or keloidal scarring, previous filler injections or ablative/nonablative laser skin resurfacing procedures, and the use of isotretinoin or other physical acne treatments over the previous six months. Patients who had any medical illness that could influence the wound healing process were also excluded.
Prior to each procedure, the treatment areas were cleansed of debris (such as dirt, makeup and powder) using a mild, nonabrasive detergent. No blue dye or gel was required to accentuate scar contours or to guarantee laser-skin contact. A topical anesthetic cream (EMLA; AstraZeneca, Wilmington, DE, USA) was applied to the sites under an occlusive dressing for 30 minutes and subsequently washed off. Treatment was then delivered using a 1550-nm erbium glass laser (Sellas; Dinona Inc., Seoul, Korea) equipped with a 15-mm handpiece. Fluence of 7 to 9 mJ/cm2 at densities of 100-200 MTZ/cm2 was applied to the regions in eight to ten passes to achieve a final treatment density of 1000 MTZ/cm2. Treatment parameters were adjusted based on skin type and tolerability. Three successive treatment sessions were performed at intervals of two weeks.
Patients were instructed to use a mild cleanser, thermal spring water spray mist, and moisturizer several times daily after each treatment session. Patients were counseled regarding strict sun avoidance and sunblock use after each treatment in order to minimize post-inflammatory hyperpigmentation (PIH), particularly in those with darker skin phototypes.7
Therapeutic outcomes were assessed by patient self-assessment of treatment results and standardized digital photography at three months after the final treatment. The self-assessed level of improvement from patients was evaluated using the following five-point grading scale: 0=no change; 1=slight improvement (1-25%); 2=moderate improvement (26-50%); 3=significant improvement (51-75%); and 4=excellent improvement (>75%). Patient satisfaction surveys regarding the six specific anatomic regions of visible wrinkle reduction were recorded at three months after the final treatment. Photographic documentations using identical camera settings, lighting and patient positioning were obtained before and three months after the final treatment. Independent clinical assessments of the treatment areas were conducted by three physicians blinded to the study subjects based on comparative photographs using the same grading scale: 0=no change; 1=slight improvement (1-25%); 2=moderate improvement (26-50%); 3=significant improvement (51-75%); and 4=excellent improvement (>75%). Pearson's correlation was used to examine the similarity of scoring between the three independent observers. The median value of the three scores in each patient was determined to be the final score of the physicians' assessment.
All participants were asked to report any local or systemic side effects associated with laser treatment. A pain scale of 0-10 was used to determine the level of pain during the laser treatment. No oral analgesic or anxiolytic medications were used.
Results
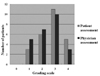
All patients completed the study, including the three-month follow-ups. At three months after the final treatment, five patients (25%) reported grade 4, 11 (44%) grade 3, and six (24%) grade 2 as their self-assessed level of improvement (Fig. 1). As for the physicians' assessment of clinical photographs, positive correlations at three months of treatment were observed between observer 1 and 2 (r=0.835, p<0.001) and observer 1 and 3 (r=0.777, p<0.001), as well as between observer 2 and 3 (r=0.471, p=0.018). At three months after the final treatment, 13 patients (52%) showed grade 3 or higher improvement (Fig. 1). Patient satisfaction surveys paralleled the physicians' assessments. Three patients with grade 1 in both the self- and physicians' assessments were all older than 55 years of age and had presented with relatively deep wrinkles.
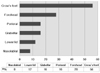
In multiple questionnaires about specific anatomic regions of visible wrinkle reduction, crow's feet was most commonly chosen (56%, 14/25) (Fig. 2). At three months after treatment, 16 out of 20 patients (80%) who had melanocytic pigmentation reported an improvement in skin tone evenness with removal of unwanted melanocytic proliferation. Five out of five patients (100%) who had significant acne scars reported a substantial improvement that included softening of scar contours as well as reduction of scar depth.
Case 1
The patient was a 40-year-old woman with Fitzpatrick skin type III. Fluence of 9 J/cm2 at a density of 100 MTZ/cm2 was applied to the regions in ten passes. The result was evaluated by both the patient and the physicians as grade 3 improvement. The skin showed tightening with a loss of crow's feet (Fig. 3A and 3B).
Case 2
The patient was a 48-year-old woman with Fitzpatrick skin type III. Fluence of 9 J/cm2 at a density of 100 MTZ/cm2 was applied to the regions in ten passes. The result was evaluated by both the patient and the physicians as grade 3 improvement. Improved skin tone evenness and a shallowing of nasolabial folds were observed (Fig. 4A and 4B).
The laser treatment was generally well tolerated. All participants experienced treatment-related pain with a mean pain score of 5.1 (range, 3 to 8). There was no need for extra anesthesia or sedation. Side effects were limited and transient. All participants reported mild erythema for approximately 2-3 days. For most patients, social engagements were limited for only 1-2 days. One patient developed transient PIH and crust after two cycles of laser treatment using 100 MTZ (Fig. 5A). But three months after the final treatment, the hyperpigmentation disappeared completely without requiring the use of any bleaching agent such as hydroquinone or other topical retinol (Fig. 5B). Other possible complications, such as vesiculation, scarring, and infection, were not reported.
Discussion
Our data demonstrate that FP is a safe, effective and noninvasive technique to induce improvement of skin tone and skin tightening with a reduction in wrinkles. This new technology has resulted in a procedure that has minimal downtime with reliable, predictable results. Fractional photothermolysis is effective for both the epidermis and dermis with minimal side effects, leaving the stratum corneum intact. Epidermal healing at the sites of injury occurred in 24 hours.5 Only 15 or 20% of the surface area is generally treated at each treatment session, and this leads to rapid healing aided by the surrounding normal skin. Therefore, controlled, limited dermal healing initiates a cascade of events in which normalization of the collagenesis/collagenolysis cycle occurs. Delivery of high fluence permits deeper heating of the dermis to maximize tissue effect.
The results of our study are consistent with previous reports in Caucasians using fractional resurfacing for wrinkles.4,6-8 Manstein et al.4 reported a mild to moderate improvement of periorbital wrinkles in 30 subjects at one and three months after four consecutive treatments. Geronemus7 noted a less impressive result in deeper rhytide using FP, as we could see in our study.
The side effects of treatment in the study reported were transient and limited to erythema and edema, except for one case of transient PIH. Post-inflammatory hyperpigmentation tends to be more common in Asians following laser surgery.10 The rate of PIH was as high as 100% in a review of 500 consecutive patients who underwent CO2 laser resurfacing.1 The melanocytes of dark-skinned patients tend to be hyperactive to stimuli such as inflammation. In a retrospective study of 37 Chinese patients who were treated with fractional resurfacing for acne scarring, skin rejuvenation, and pigmentation, the overall rates of PIH in wrinkles/pigmentation and acne scarring were 12.4% and 7.1%, respectively. The risk of PIH among dark-skinned patients tends to be lower with fractional resurfacing than with laser resurfacing.11 Similarly, only one case (4%) of PIH transiently developed in our study.
More recently, Jih and Kimyai-Asadi12 published data from 50 patients with rhytides who responded to Fraxel (SR750; Reliant Technologies, Mountain View, CA, USA) treatment using a pulse energy of 8 mJ with a density setting of 250 MTZ/cm2 for a final treatment density of 1500 to 2000 MTZ/cm2. We used similar pulse energies of 7-9 mJ with a lower density setting of 100-200 MTZ/cm2 for a final treatment density of 1000 MTZ/cm2, in consideration of the depth of wrinkles and tolerability to laser treatment.
In a recent study, FP treatments were performed on the eyelid area13 at a significantly higher energy of 17 to 20 mJ and a lower density of 125 MTZ/cm2. The use of high energy and low density seemed to be more effective for the treatment of wrinkles of the eyelid area. Satisfaction was reported to be greater in Asian patients at higher energies, but not higher densities, as increased densities were more likely to produce complications when compared to increased energies.14 As Asian skin is relatively thicker than Caucasian skin, if a patient is tolerable, higher pulse energies are more effective at improving rhytides and skin texture. However, in this study, we did not use high energy, as energy over 10 mJ caused too much pain for the patients.
Indeed, one weakness of this study was the lack of long-term follow up. Although our study was designed to evaluate the short-term results and complications of FP, further prospective long-term work is essential for the development of improved methods for better results and to identify the potential long-term manifestations.
In conclusion, fractional resurfacing is a safe and effective option for the treatment of wrinkles and skin rejuvenation in Asians. The skin shows improved skin tone evenness and skin tightening with a reduction in wrinkles. Acne scars also showed improvement. Resurfacing with FP results in both the rejuvenation of skin and a high patient satisfaction and self-esteem. The treatment parameters must be continually refined to optimize outcomes and minimize side effects.



 XML Download
XML Download