

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Polypoidal choroidal vasculopathy (PCV) is a choroidal vascular disease characterized by an inner choroidal vascular network ending in an aneurysmal bulge or outward projection visible clinically as a reddish orange, spheroid, polyp-like structure.1-3
PCV can remain clinically asymptomatic in its quiescent form, with nonleaking asymptomatic polyps. Occasionally, PCV causes insidious visual loss owing to serosanguinous detachment of the retinal pigment epithelium and neurosensory retina affecting the macula, or causes acute and severe visual loss secondary to massive submacular or vitreous hemorrhage due to spontaneously ruptured vessels.4,5 Treatment for PCV is not yet well established. Asymptomatic PCV is recommended for observation and the polyps may resolve spontaneously over time.5,6 Although various treatment modalities for PCV with exudative and hemorrhagic complications such as direct thermal laser photocoagulation, tissue plasminogen activator (t-PA) injection with gas displacement, submacular surgery, and macular translocation surgery have been proposed, the beneficial effects are still in doubt owing to recurrence or poor long-term results.7-11 Recently, photodynamic therapy (PDT) has been proposed as a standard treatment modality with its favorable outcome, nevertheless its application has been found to be limited owing to difficulty in treating all wide spread multiple polyps and the possibility of subsequent massive submacular hemorrhage.12-14
Favorable results have been reported with intravitreal injection of bevacizumab (Avastin®, Genentech, Inc. South San Francisco, CA) to treat choroidal neovascularization.15-18 Although the pathogenesis of PCV is still not fully understood, it has been suggested that vascular endothelial growth factor (VEGF) may have a similar role in PCV as it does in choroidal neovascularization (CNV) owing to marked increases in VEGF concentration in aqueous humor and histologic examination in active PCV eyes.19,20 The aim of the present study was to determine the efficacy and safety of intravitreal bevacizumab, alone or in combination with PDT, for the treatment of PCV.
Materials and Methods
The retrospective interventional case series study included medical records of 12 eyes of 11 patients with symptomatic PCV who were either newly diagnosed or failed in previous treatment and treated PCV at Asan Medical Center, Seoul, Korea, from January 2006 to October 2006. The study was approved by the Institutional Review Board at the Asan Medical Center and informed consent was obtained from all patients. Patients with new or recurrent subretinal pigment epithelial orange-red vascular lesions associated with exudative changes were included. To confirm the diagnosis of symptomatic PCV, all patients underwent fluorescein angiography (FA), indocyanine green angiography (ICGA), and optical coherence tomography (OCT) analyses. All patients also underwent a comprehensive ocular examination, including best-corrected visual acuity (BCVA), slit-lamp biomicroscopy with intraocular pressure measurement and indirect ophthalmoscopy.
Patients received either an intravitreal injection of bevacizumab alone (Group 1) or an intravitreal injection of bevacizumab combined with PDT on the same day (Group 2) according to informed patient's choice. For intravitreal injection, 1.25 mg of bevacizumab was given using a 30-gauage needle after topical anesthesia. For combination therapy, PDT was performed to cover the entire lesion of symptomatic PCV lesions in a standard manner and the 1.25 mg intravitreal bevacizumab injection was then administered.
Follow-up evaluations were made at 1 week, 6 weeks and then every 2-3 months after treatment. BCVA, funduscopic exam, and OCT tests were performed at every visit, and FA/ICGA was assessed at the ~3 month visit or earlier if necessary. FA/ICGA findings were reviewed to confirm the regression of active PCV, and visual acuity and tomographic findings were recorded to assess the efficacy of the treatment. Side effects related to the procedure were also evaluated.
Results
The patient characteristics and clinical data of group 1 and group 2 are listed in Table 1 and Table 2. The 11 patients (ten men and one woman) were aged 45-80 years (mean 63±7 years in group 1 and 53±7 years in group 2). Cases 1 and 8 in group 1 and case 9 in group 2 received prior PDT (9, 4, and 22 months before treatment of bevacizumab, respectively). Case 11 in group 2 had received prior gas tamponade with t-PA due to massive submacular hemorrhage at presentation. Case 4 had previously received gas tamponade with t-PA due to massive submacular hemorrhage followed by prior PDT. All patients who had received prior treatment switched treatment to intravitreal injection of bevacizumab with/without combined PDT owing to persistent or recurrent PCV. All patients except cases 5, 7 and 11 received repeated intravitreal bevacizumab at 6 week intervals owing to persistent subretinal fluid, as shown by OCT analysis, or leakage, as shown by FA/ICGA analysis. Intravitreal bevacizumab was well tolerated in all patients. There were no procedure-related complications in any of the patients.
Mean follow-up duration was 17 weeks (range, 12-27) in group 1 and 15 weeks (range, 13-22) in group 2. The mean number of intravitreal bevacizumab injections was 2.2 in group 1 and 2.5 in group 2. Mean BCVA improved in both groups from 20/63 to 20/40 in group 1 and 20/63 to 20/32 in group 2. Of all eyes, BCVA improved by ≥2 lines in seven (58%) eyes, and there was a moderate gain in vision in four (33%) of these eyes (BCVA improved by ≥3 lines). Three (25%) eyes had stable vision, with BCVA at the last follow-up being within 1 line of the initial BCVA level. Resolution of fluid and hemorrhages in clinical examination, and absence of leakage on repeat FAs or resolved pigment epithelial detachment (PED) and/or subretinal fluid (SRF) on OCT examinations could be seen in 10 (83%) eyes. Regression of the polypoidal vessels and interconnecting vessels were seen in most cases at the last follow-up.
Case Report (Cases 3 and 4)
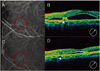
A 63-year-old man was referred to our clinic with a 5 month history of reduced visual acuity in the right eye. At the first visit, his visual acuity was 20/63 in the right eye and 20/20 in the left eye. Based on the findings in FA and ICGA, he was diagnosed as having PCV in his right eye and was treated with PDT covering whole active lesions. Four weeks after PDT, funduscopic examination of the right eye revealed extensive subretinal hemorrhage with a reduced visual acuity of 20/320. The right eye with massive subretinal hemorrhage was treated with intravitreal t-PA (50 µg) and 0.3 ml of 100% C3F8. Postoperative prone positioning was maintained for 72 hours. Two weeks after administration of t-PA injection and gas, funduscopic examination of the right eye showed dispersed and reduced subretinal hemorrhage (Fig. 1). At one month follow up, he complained a decreased vision to 20/50 in his untreated, left eye. The OCT examination demonstrated subfoveal serous elevation and FA/ICGA confirmed new active PCV in his left eye (Fig. 2). Both eyes were treated with an intravitreal injection of 1.25 mg bevacizumab, two injections in the right eye and three injections in the left eye, at 6 week intervals. The final visual acuity was 20/320 in the right eye with fibrovascular scarring and 20/32 in the left eye with minimal subfoveal serous elevation.
Discussion
Polypoidal choroidal vasculopathy (PCV) was first described by Yannuzzi et al.1 and is characterized by an abnormal vascular network of choroidal vessels with polyp-like dilations at the terminals of the branches. It is unclear whether PCV represents abnormal vessels from the choroidal circulation or is a variant of CNV. However, it is generally considered distinct from CNV of age-related macular degeneration (AMD) for several reasons. First, PCV mainly affects Asians and pigmented individuals and is associated with an earlier onset and a relatively benign clinical course.1 Second, a few histopathologic studies have revealed that, unlike CNV which is located mainly under the Bruch's membrane, polypoidal lesions and a branching vascular network are observed inside the Bruch's membrane in cases of PCV.11 Finally, although eyes affected with PCV have several retinal features in common with CNV of AMD, they also have some unique features such as a large (greater than 4-disc area) serosanguinous retinopathy, orange polyp-like structures, an absence of macular drusen, and multiple lesions scattered throughout the posterior pole including the peripapillary region.1
Since the role of VEGF in the pathogenesis of CNV was established, several studies have reported on the efficacy of anti-VEGF therapy for the treatment of AMD-related CNV.15-17 An earlier study found that pegaptanib (OSI/Eyetech, Melville, NY) slowed the rate of visual loss, and a more recent, well-controlled study demonstrated a marked improvement in visual acuity following ranibizumab (Genentech, South San Francisco, CA) treatment of exudat ANB AMD patients.22,23 Although bevacizumab (Genetech) may have a lower affinity for VEGF than ranibizumab owing to structural differences, it has been reported to be as efficacious as ranibizumab in the treatment of CNV secondary to AMD or pathologic myopia by several investigators.15-18
While the present study has a limitation with its retrospective design, non-randomized treatment groups, a small series of patients, and short follow-up time, our results as a pilot study demonstrate the benefits of intravitreal injection of bevacizumab, either as monotherapy or in combination with PDT, for the treatment of active PCV. This is not surprising considering previous reports demonstrating the role of VEGF in PCV.19,20
Although PDT is often considered a standard treatment modality for PCV owing to a high regression rate and favorable functional outcome, it is associated with several disadvantages.12,13 First, PCV often presents as multiple, widely distributed lesions, so it might be difficult to treat all lesions, including multiple polyps and interconnecting vessels, with a single beam of PDT. Treatment of leaking polypoidal dilations only without treating the entire vascular complex can result in persistence or worsening of exudation.24,25 Second, it can be difficult to treat nodules in the peripapillary area with a round PDT beam.26 Third, features commonly associated with PCV such as a large PED or a large submacular hemorrhage are not usually amenable to PDT treatment.27,28 Fourth, PCV tends to recur repeatedly so multiple PDT treatments are often necessary, which can increase the risk of long-term choroidal atrophy.29 Finally, cases of massive subretinal/suprachoroidal hemorrhage, as in case 4 in this study, have been reported soon after PDT.14,30,31 Although a direct causal association has not been proven, this devastating complication usually results in irreversible visual loss so the risk should be avoided whenever possible (Fig. 3).
Although bevacizumab is recommended as adjuvant therapy in combination with PDT for advanced cases that require prompt closure of an abnormal choroidal neovascular complex (Fig. 4), our results indicate that bevacizumab alone may now be considered a primary treatment for early, milder cases, which often occur in the other eye of a patient with an already badly affected eye (Fig. 1, 2). The bilateral example (cases 3 and 4) presented in the case report are examples of a particularly serious complication of PDT, which could be avoided by treatment with bevacizumab alone in the patient's other eye. Longer follow-up is necessary to determine whether repeat bevacizumab injections alone are sufficient to induce permanent regression of PCV, or whether combination therapy with PDT is required.
As the use of intravitreal triamcinolone as an adjunct to PDT has been shown to improve the visual outcome by downregulated expression of inflammatory mediators, and possibly VEGF, after PDT, direct inhibition of VEGF by bevacizumab in combination with PDT may provide a beneficial synergistic effect.32 In addition, direct VEGF inhibition with combination treatment would not only reduce the potential for neovascularization, but would also reduce retinal edema owing to laser burn.
This study has several limitations, including retrospective design, non-randomized treatment groups, a small series of patients, and short follow-up time. However, rapid improvement in vision as well as no significant complications after intravitreal bevacizumab treatment are encouraging, and may indicate that intravitreal bevacizumab should be considered a new treatment for active symptomatic PCV.
In conclusion, our results indicate that intravitreal bevacizumab treatment, either alone or in combination with PDT, may be a promising approach for treating active, symptomatic PCV. Further investigations including a large, controlled trial, are necessary to determine the efficacy.





 XML Download
XML Download