

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Compared with such conventional methods as optic disc analysis and visual field examination, the analysis of the peripapillary retinal nerve fiber layer thickness (RNFLT) by optical coherence tomography (OCT) is advantageous in making the diagnosis of pediatric glaucoma because the measurement is objective and shows reproducible results. Thus, the importance of this method has been documented in many reports.1-7 For its clinical application, it is important to determine the normal value of the normal RNFLT, yet only the adult (older than 18) thickness of the peripapillary RNFL is currently known, which is not applicable to children. Therefore, studies on the normal value for children are now ongoing and a new equipment for the quantitative and qualitative analysis of the peripapillary RNFLT has been developed. In addition, various factors have been reported that may influence the analysis of the RNFLT by OCT. According to the histological study of optic nerves by Quigley et al.8 and Jonas et al.9 as the size of the optic disc area (ODA) becomes larger, the number of optic nerves becomes greater, and Caprioli and Miller10 have reported that as the ODA becomes larger, the optic disc rim area is also increased. Budenz et al11 have reported in a study conducted on adults older than 18 years that as the axial length becomes shorter and as the ODA becomes larger, the RNFLT has a tendency to become thicker, and it is possible that obtaining a small measured value of the peripapillary RNFLT in patients with axial myopia may be an error, but any correlation of the axial length to the ODA could not be confirmed.
Therefore, in this study, we assessed the pattern of change of the ODA according to refractive errors and the differences of the axial length in normal children between the age of 4 years and 15 years. Further, we examined the effect of the consequently altered distance of the circular scan of OCT and the optic disc margin on the measurement of the peripapillary RNFLT.
Materials and Methods
From June 2006 to February 2007, we determined the uncorrected visual acuity and performed refraction, slit lamp examination, fundus examination and OCT on 102 eyes of 51 children (age range: 4 to 15 years) who visited our hospital.
The refractive error value was obtained by the spherical equivalent through a cycloplegic refraction test, and the children were divided into 3 groups according to their refractive status level: ≥ -0.50 Dsph. and < +0.50 Dsph were designated as the emmetropic group, the hyperopic group was ≥ +0.50 Dsph. of the spherical equivalent value, and the myopic group was < -0.50 Dsph. The subjects with amblyopia, strabismus, anisometropia, astigmatism higher than 2.00 D, a unilateral or bilateral cup/disc ratio higher than 0.5 on fundus examination, a difference of the cup/disc ratio of the two sides higher than 0.2 and the cases with a history of ophthalmic surgery or ocular trauma were excluded from this study.
The RNFLT was measured using the optical coherence tomography, STRATUS OCT (OCT, Version 4.0.1, Carl Zeiss Meditech, Dublin, CA, USA). Prior to testing, the pupils of the children were dilated by applying 0.5% proparacaine hydrochloride (Alcaine®, Alcon, Purrs, Belgium) to the eye once and 1% tropicamide (Ocutropic® Sam I1 Pharma., Korea) and 2.5% phenylephrine hydrochloride (Mydfrin®, Alcon, Texas, USA) to the eye three times at 10 minutes intervals; the eyes of the subjects were fixed and examined by the internal fixation method. Considering that the subjects were children, the RNFLT was measured along the optic disc margin according to the Fast RNFL Thickness Protocol to shorten the test time while enhancing the efficacy. Concerning the results of the RNFLT, the mean thickness was measured along the concentric center of the optic disc margin, and the thickness of the four areas (the superior, inferior, nasal and temporal sides) was determined. In addition, the superior, inferior, nasal and temporal sides were divided by 30 degrees into 3 compartments and the 12 areas were classified by the RNFLT as measured in each area. The correlation of the distance from the optic disc margin to the circular scan (OD-CS) and thickness measured in each area was then analyzed.
We measured the ODA, as well as OD-CS by scan analysis of the optical coherence tomography. The analysis of the results of the RNFL Thickness (Single Eye), which were obtained after performing RNFL Thickness (Single Eye), was done by applying the Adobe Photoshop CS2 (Adobe Systems Inc., San Jose, CA, USA) program. The video fundus images obtained during the circular scan were pretreated. From the pretreated images, by entering the term "area" in the AutoCAD 2008(Autodesk Inc., San Rafael, CA, USA) program, the location along the circular scan and the optic disc margin higher than a minimum 60 points was designated by the mouse pointer and each relative area was then calculated. With arbitrarily using the calculated relative area, the radius of the circular scan was designated as r1, and since the optic disc is not a perfect circle, the mean radius of the disc area was assigned as r2, and applying the modification r1=10.87/2π and r2=A × (10.87/2π), the radius of the circular scan and the mean radius of the optic nerve disc were obtained (A=optic disc area/circular scan area).
For the measurement of the axial length, 0.5% proparacaine hydrochloride solution was applied to both eyes one time each, and the patients were asked to stare at a fixation point that was marked 6 meters away, and the axial length was measured using the B.V. International Echograph Model Compact Class I-Type B. Both eyes were each measured 10 times consecutively. The initial 10 measurements was ignored, and the mean value (S.D<0.08) of the next 10 consecutive measurements was recorded as the axial length of the subject. To reduce measurement errors, all the test were performed by one single experienced examiner.
For statistical analysis, the Minitab program (version 14.20, Minitab Inc., State College, Pennsylvania, USA) was used. For comparison between the two groups, independent T-tests were applied, one way-ANOVA testing was applied for the F-test, and the correlation of the independent variables and dependent variables was analyzed by Pearson's correlation tests. For multiple comparisons, the Normality Test was performed as the principle test, and for the data that did not show a normal distribution or for groups with less than 10 individuals, the nonparametric test method and Kruschal-Wallis test were used. The association between the independent variables and the dependent variables were assessed by regression analysis, and the R2 was calculated. P-values less than 0.05 were considered to be statistically significant.
Results
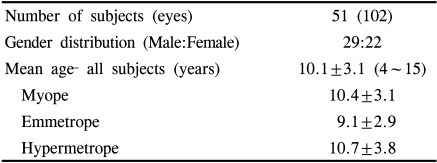
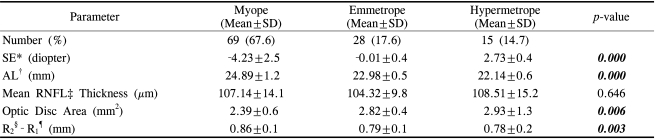
There were 29 males (56.9%) and 22 females (43.1%). Their mean age was 10.1±3.1 years (range: 4 to 15 years). Hyperopia was noted in 15 eyes, emmetropia was noted in 18 eyes and myopia was noted in 69 eyes. The hyperopia group was 10.7±3.8 years old, the emmetropia group was 9.1±2.9 years old, the myopia group was 10.4±3.1 years old and there was no statistically significant difference among the three groups (p=0.550) (Table 1).
The mean of the spherical equivalent all subjects was -2.5±3.4 Dsph., the hyperopia group mean was +2.7±1.4 Dsph., the emmetropia group mean was 0.0±0.4 Dsph. and the myopia group mean was -4.4±2.4 Dsph.
The mean axial length of the hyperopia group was 22.1±0.6 mm, that of the emmetropia group was 23.0±0.5 mm and that of the myopia group was 24.9±1.2 mm; a statistically significant difference among the three groups was detected (p=0.000). The mean peripapillary RNFLT of the hyperopia group was 108.5±15.2 µm, that of the emmetropia group was 104.3±9.8 µm and that of the myopia group was 107.1±14.1 µm, and a significant difference among the three groups was not detected (p=0.646). The mean optic disc area of the hyperopia group was 2.9±1.3 mm2, that of the emmetropia group was 2.8±0.4 mm2 and that of the myopia group was 2.4±0.6 mm2; a significant difference was shown (p=0.006). In addition, the mean OD-CS of the hyperopia group was 0.78±0.2 mm, that of the emmetropia group was 0.79±0.1 mm and that of the myopia group was 0.86±0.1 mm; a statistically significant difference was shown (p=0.003) (Table 2).
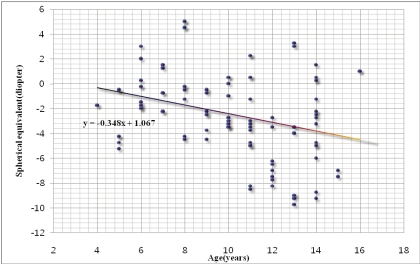
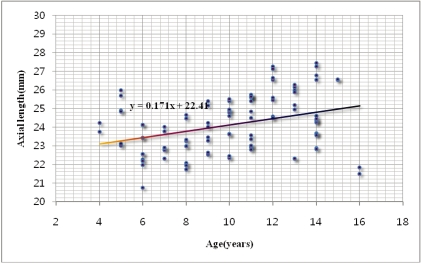
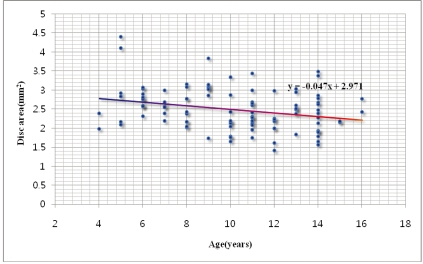
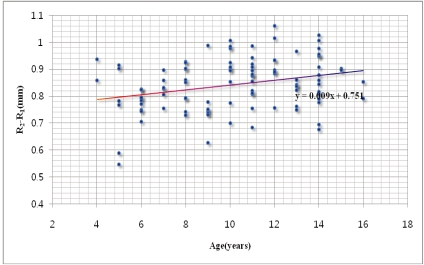
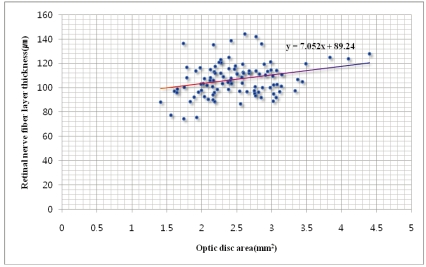
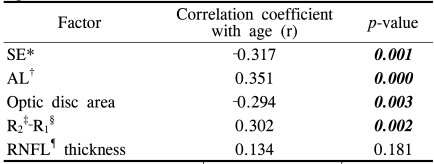
As the children's age increased, a trend for a decrease of the spherical equivalent from hyperopia to myopia was shown and the axial length had the tendency to be increased (r=-0.317, p=0.001, r=0.351, p=0.000) (Fig. 1, Fig. 2). Correlations of the ODA and the OD-CS with age were detected (r=-0.294, p=0.003, r=0.302, p-=0.002) (Fig. 3); nevertheless, these were not significantly correlated to the mean peripapillary RNFLT (r=0.134, p=0.181) (Table 3, Fig. 4).
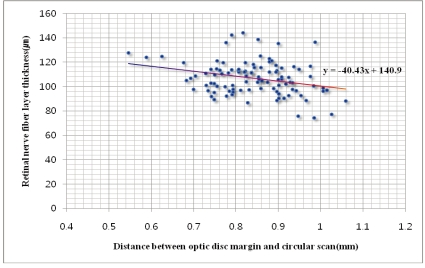
In addition, as refractive error changes from hyperopia to myopia and as the axial length becomes longer, the ODA became smaller and the OD-CS showed a tendency to be increased (r=-0.442, p=0.000, r=0.471, p=0.000) (Table 4), and the ODA and the average RNFLT showed a statistically low correlation (r=0.221, p=0.025) (Fig. 5) Further, the OD-CS showed an inverse correlation to the mean retinal nerve fiber layer thickness (r=-0.248, p=0.012) (Fig. 6). Univariate regression analysis showed that the results of the regression equation for the relationship of the RNFLT was 131-29.3 (r2-r1).
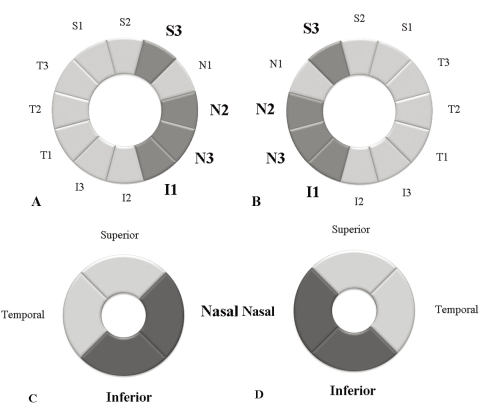
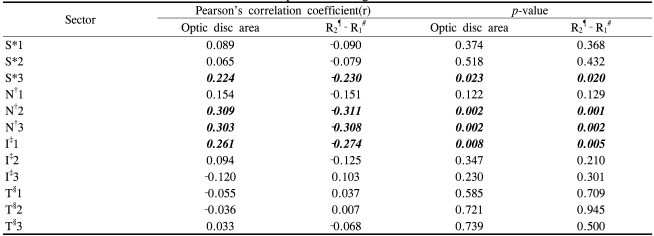
The RNFLT, as measured by dividing the peripapillary margin into 4 areas by 90 degrees, was shown to be significantly correlated to the optic disc area only in the inferior area and the nasal area (inferior side: r=0.281, p=0.006, nasal side: r=0.269, p=0.004), and the OD-CS showed the same results (inferior side: r=-0.301, p=0.002, nasal side: r=-0.285, p=0.005) (Table 5). Statistically significant correlation was shown on the correlation analysis of the RNFLT, as measured by dividing the optic disc by 30 degrees into 12 areas, with the ODA and the OD-CS, but only in the S3, N2 and N3 areas and the I1 disc area (Fig. 7) (Table 6).
Discussion
To diagnose glaucoma in those cases for which the peripapillary retinal nerve fiber layer thickness was measured by the Fast RNFL Thickness Protocol (3.4) of OCT during 1.92 seconds, a circular scan 3.4 mm in diameter is performed in the optic disc area. Therefore, regardless of the disc diameter of the subject, the scan always measures the RNFLT at a constant site, and by comparing this value with the already known normal values of each area of the optic disc, those cases with thinner than normal values in a specific area are diagnosed with loss of the retinal nerve fibers due to glaucoma.
There have been several reports that as the patient's age becomes higher and as the refractive error becomes more myopic and the axial length increases, the RNFLT has a tendency to decrease.5,6,11-16 And Song et al16 have shown that as age becomes higher, the ODA has a tendency to be increased in children. Budenz et al11 recently reported such a tendency for the peripapillary RNFLT, and they proposed several hypotheses for this association. They reported that the refractive error and the axial length of the subject are constantly correlated to the ODA, and as the ODA becomes larger, the number of retinal nerve fibers is increased and so the peripapillary RNFLT may be measured to be thick. In addition, depending on the size of the optic disc, the distance from the circular scan to the disc margin varies, and the RNFLT becomes thinner as it became more distanced from the disc margin; thus, there may be such a tendency because of errors when measuring the thickness. However, in that study, statistical correlation of the axial length to the disc area could not be confirmed.
Histologically, according to the study reported by Quigley et al8 and Jonas et al9 as the disc area becomes larger, the number of retinal nerve fibers is increased. Caproli and Miller10 have reported that as the disc area becomes larger, the optic disc rim area becomes larger. In addition, Johnson et al17 have reported that in monkeys, as the ODA becomes larger, the number of retinal nerve fibers is increased and particularly with aging, and so they reported the reduction of the RNFLT with aging. Nevertheless, retinal tissues are very sensitive to conditions such as tissue hydration, and numerous variations may be generated in the analysis of the retinal nerve fibers. Indeed, contradictory results has been shown in several studies, and so the direct application of in vitro research results directly to in vivo settings may have some limitations.18-21
There have not been any optical coherence tomography studies that have directly shown the difference of the RNFLT according to the disc area. On reviewing the research that has applied a scanning laser polarimetry, which measures the RNFLT located at a constant distance from the disc margin, Park and Choi22 have reported that in normal individuals, as the optic disc area becomes larger, the peripapillary RNFLT showed a tendency to be increased in all areas in the vicinity of the disc. Our study showed similar results in that as the disc area becomes larger, there was a tendency of an increased average peripapillary RNFLT.
Park and Choi22 reported that the nerve fiber layer thickness measured in most parts of the temporal area correlated to the disc area. However, when we divided the peripapillary area to 4 quadrant areas of 90 degrees, in the nasal side and the inferior side, as the disc area becomes larger, the distance to the circular scan becomes shorter and the RNFLT measured in the nasal side and inferior side showed a tendency to be increased. When performing analysis by dividing the peripapillary area by 30 degrees into 12 areas, in some areas of the superior side and inferior area and in most of the areas of the nasal side (S3, N2, N3, I1), the measured thickness showed a tendency to be increased as the disc area becomes larger and as the distance to the circular scan becomes shorter. This was different from the results of Park and Choi22, which may be due to the fact that scanning laser polarimetry measures the RNFLT of a site with a constant distance from the disc margin. But nonetheless, the retinal nerve fiber layer thickness was measured in the site that was distanced by 1.75 optic disc diameters from the retinal optic disc margin, and so as the ODA becomes smaller and relatively thicker, it is measured to be thinner and, results different from ours may be obtained. These different results are also thought to be due to the fact that the circular scan of OCT forms a perfect concentric circle, yet the shape of the optic disc is elliptical and thus the OD-CS is not constant depending on the areas. Different from this, the scanning laser polarimetry performs the measurement in a location distanced from the optic disc margin by 1.75 optic disc diameters and this is drawn by the examiners, and so the distance from the optic disc margin to the measurement location is relatively constant. It has been reported by several Korean studies, as well as those from other countries, that the RNFLT measured by OCT varies depending on the refractive error, the axial length and the subject's age.5-7,11-15,23,24 However, when comparing the results with using various measurement equipmenst, contradictory results were shown in some cases, and Garcia-Valenzuela et al25 have shown in their study that the axial length and refractive error are not related to the RNFLT, as measured using a scanning laser polarimetry. Kim and Roh26 have reported that on the analysis of the RNFLT by applying the same measurement method, age and the RNFLT were not correlated. However, our study showed that as the refractive error changes from hyperopia to myopia, the axial length becomes significantly longer, and there is the tendency that as the axial length becomes longer, the optic disc area becomes distinctly smaller. Therefore, age, refractive error and the axial length have statistically significant correlations, and the correlation to the RNFLT that was reported by previous studies may only be due to measurement errors because the fixed circular scan diameter was too large. On the other hand, the laser polarimetry scanned a relatively constantly distance from the optic disc margin, and thus, a distinct correlation was not shown.
In our study, on the separate analysis of each area, the correlation of optic disc factors to the RNFLT of each area was shown to be different, and it may be possible that as the distance from the optic disc becomes farther, the degree of decrease of the RNFLT may be different, and indeed, the peripapillary RNFLT shows a "double hump" pattern, which may be considered to be an indirect proof of such a possibility. Therefore, new information could be obtained to decrease the false positive and false negative findings by interpretation of the amount of damage of the retinal nerve fiber layer in the S2, N2, N3, and I1 areas via a RNFL thickness analysis of the measurement of the adult RNFLT by OCT.
We did not use any color fundus images obtained from a fundus camera and the optic disc analysis program within the OCT was not used for the measurement of the optic disc area. The scan wavelength that was used for the OCT was 820 nm; the refraction level was very small when using the ultra-red type wavelength, and it hardly influenced the refractive factors of the subject,. On the other hand, visible light with a relatively short wavelength is used for the fundus images taken by a fundus camera and the measurement may be somewhat distorted due to the refractory factor of the subject. In addition,in the optic nerve head analysis of OCT centered on the optic disc, the area is calculated based on 12 reference points of the cross-sectional line scan measured by 6 radii, and measurement errors of the disc area may occur. Furthermore, in the eyes with high myopia and significant peripapillary chorioretinal atrophy that show difficult distinction of the retinal nerve disc margin, the chorioretinal atrophy may be included in the optic nerve disc and the optic disc area may be measured to be large.Also there is a possibility of error in the measurement of the optic disc with a steep slope as the OCT is scanned vertically to the optic nerve disc.26 We used the video fundus images taken during the measurement of the peripapillary RNFLT, the correlation of the circular scan of OCT to the disc area as well as the correlation between the distances, for accurate analysis. The video fundus images were taken as a supplement to determine the site of scanning, and these images were pretreated at a constant level using a commercialized Photoshop program and applying the AutoCAD program. More than 60 points were assigned to optic disc image and the area was then measured. Thus the measurement error of the area was minimized as the ratio of the optic disc area to the circular scanning area was calculated.
The limitation of our study is that the number of subjects was small, and therefore it was difficult to confirm the change of the ODA according to the refractive error and the consequent correlation of the peripapillary RNFLT. A future study with a larger number of children is required to confirm our results. In addition, the study was limited to children, and a future long term study in adults may be required.
In summary, the ODA of children showed a distinct difference according to age, the refractive error and the axial length, and the OD-CS of OCT could be distinctly altered depending on the disc area. Therefore, as the axial length is increased and a myopic refractive condition occurs, the RNFLT obtained by performing circular scanning on a fixed diameter has a tendency to be decreased in a specific ODA. It is thought that for the diagnosis of pediatric glaucoma, the RNFLT needs to be adjusted according to the above mentioned characteristics.


 XML Download
XML Download