

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Laser epithelial keratomileusis (LASEK) is a surgery that corrects refractive errors to a desired level by creating a corneal epithelial flap, irradiating the exposed Bowman's layer with excimer laser, and then re-placing the flap,1,2 with the use of therapeutic contact lenses after surgery. With regards to recovery after LASEK, the scar healing process and epithelium recovery may differ depending on whether the epithelial flap survives or not. In the cases wherein the epithelial flap adheres and survives, the shedding of the epithelium's monolayer structure occurs gradually for 3-4 days after LASEK surgery, and the epithelial cells are shed to the underside of therapeutic lenses gradually.3
Generally, therapeutic contact lenses perform the role of accelerating scar healing and protecting the corneal surface mechanically as well as reducing the discomfort caused by the abnormality on the corneal surface and maintaining appropriate humidity on the corneal surface.4,5 In addition, therapeutic contact lenses have to be selected based on their appropriateness for therapy, taking into consideration the oxygen permeability, water content, raw materials, diameter, thickness, the base curve, the peripheral curve, the rim, and other factors.4-7
After LASEK surgery, for the corneal epithelium to recover, selection of appropriate therapeutic lenses is required. Among other factors, it is required to select the appropriate base curve radius since the keratometry value changes after LASEK surgery. Therefore, in our study, the effect of the base curve radius (BCR) on the corneal healing period after LASEK surgery was examined.
The Subject and Methods
The subjects were 47 patients (92 eyes) who wore therapeutic lenses after LASEK surgery performed by a single surgeon from October 2004 to December 2005 at Seoul national university hospital. Pre-operative examinations performed including a slit-lamp examination, manifest refractive errors, cycloplegic refractive errors, tonometry, fundus examination, pupil size, Schirmer test, corneal topography, wavefront analysis, corneal pachymetry, and keratometry. Patients who underwent refractive surgery previously, with dry eye syndrome, cataract, keratoconus, glaucoma, retinal disease, optic neuropathy, connective tissue disease, or systemic diseases were excluded.
LASEK surgery was performed by spreading the palpebral fissure with a speculum, administering 0.5 % proparacaine hydrochloride (Alcaine®, Alcon, USA), placing an alcohol solution cone 8.5 mm in diameter (J2905, Janach, UK) on the cornea, diluting with distilled water, placing 20 % alcohol solution on the cone, waiting for 30 seconds, adding balanced salt solution, and washing sufficiently. Subsequently, using an epithelial microhoe (J2915A, Janach, UK), the corneal epithelium was resected smoothly. And at later time, the corneal epithelial flap was gathered at 12 o'clock direction using a spatula. At the time of resection, the basement membrane was resected carefully from the Bowman's layer. Cases whose corneal epithelial fragment was not created as a complete flap were excluded from the subject group. After the irradiation with excimer laser (Star S4, VISX, Santa Clara, USA), the corneal epithelial flap and the corneal stroma were washed sufficiently with buffer solution and carefully placed in the original site with a spatula. After LASEK surgery, therapeutic lenses, of which the base curve radius (R1) was within 8.6 - 9.0 mm range, were selected randomly and worn. The characteristics of therapeutic lens used in our study are summarized in Table 1. Patients were examined 1 day, 4 days, 6 days, and 8 days after surgery. Also, eye drops of 0.1 % Fluorometholone (Fluorometholone®, Santen, Japan), Levofloxacin (Cravit®, Santen, Japan) were administered 4 times per day, and until the defect of the corneal epithelium recovered completely, the eyes were examined without removing the corneal epithelial flap.
We calculated the estimated BCR (R2) by calculating keratometry value on corneal topography after surgery, using the diopter conversion table. According to the differences of BCR (R1) and the estimated BCR (R2), they were divided into group A and group B. Group A was defined as the group with lenses that had a BCR larger than the BCR calculated by postsurgical keratometry (flat group: R1>R2); group B was the group with lenses that had a BCR smaller than the BCR calculated by postsurgical keratometry (Steep group: R1<R2). The age, gender, corneal curve radius, and the corneal epithelial healing period of the two groups were compared.
Statistical analysis was performed using the SPSS v12.0 (SPSS Inc., Chicago, USA). An independent T-test was used for comparing the two groups and for the cases showing significant results in univariant regression analysis, multivariant regression analysis was performed. Cases with a p value less than 0.05 were considered significant.
Results
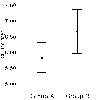
The subject group had a total of 47 patients (92 eyes); group A had 53 eyes and group B had 39 eyes. In group A, the healing period after LASEK surgery was on average 5.8±1.7 days; in group B, the corneal epithelial healing period after LASEK surgery was on average 6.7±2.1 days, a statistically significant difference (p=0.04, independent T-test, Figure 1).
In addition, the difference in the mean value between the BCR of therapeutic lenses and the BCR anticipated after surgery (R1-R2) in group A was 0.5 mm. In group B, the difference was -0.4 mm. Even though age, gender ratio, and the BCR of the contact lens used were not different, the preoperative keratometry, postoperative keratometry, and the ablation depth between the two groups were significantly different (Table 2 and 3). To examine the effect of various factors, for variables with p values lower than 0.2 in univariant analysis, multivariance regression analysis was performed. The result showed that it was not associated with other variables and a significant difference was observed only in the BCR (Table 3). In other words, when therapeutic lenses that are flatter than the BCR according to the keratometry were worn after LASEK, the healing of the epithelium was faster.
Discussion
LASEK is a refractive surgery that has been used frequently together with LASIK and PRK. Previous reports have suggested that complications associated with the corneal flap in LASIK could be avoided by use of LASEK, that it is applicable to patients whose corneal thicknesses are thin,1 and that the frequent pain or subepithelial haze after PRK could be reduced.8 It is considered that reasons causing the less subepithelial haze are that after LASEK surgery, the scar healing process is similar to PRK, nonetheless, it allows the faster migration of epithelial cells, and thus ultimately, less cellular reaction in the stroma is induced. The cytokine that is involved in the subepithelial haze, TGF-β 1 was detected to be less in the tear than PRK. The epithelial flap plays a physical barrier function and thus reduces the secretion of reflex tearing, consequently, the contact with Fas ligand and other cytokines inducing stromal reactions present in the tear was reduced.9-11 Nevertheless, some researchers claimed that the subepithelial haze after PRK and LASEK was not different, and the postsurgical visual acuity immediately after LASEK was rather poor, because of edema in the epithelial cell flap itself. It did not adhere well to the stroma, and over time it was destroyed naturally, replaced with the new epithelium growing from the vicinity. Hence, the regeneration was ultimately slower than PRK.2 Such corneal scar healing is a reaction associated with various cytokines, growth factors, receptors, and the stroma, and thus there is speculation that the activated corneal stromal cells ultimately induce stromal opacity. Therefore, appropriate healing after refractive surgery is necessary to minimize the development of opacity; For this to occur, the necessary local objectives are: to reduce the patient's postoperative pain by the rapid healing of corneal epithelium, to block excess signal transduction required for healing, and to maintain appropriate corneal cell activity.12,13 To that end, therapeutic lenses have been used after LASEK surgery.
The first therapeutic lenses were designed by Ridley and during the subsequent 20 years, techniques to produce the lenses' raw materials and application techniques have been improved.5 The cornea uses oxygen dissolved in tear film and, when therapeutic contact lenses are worn, oxygen is supplied to the cornea only by diffusion through the lens itself. In regard to oxygen's diffusion ability, the raw material of the lens itself is a variable; nevertheless, it is also influenced by the BCR, the peripheral base curve, the rim, etc. If therapeutic lenses were worn for a long time, side effects caused by hypoxia did develop5 and mechanical trauma was induced on the cornea and contact lenses with high water content induced more corneal surface dryness in dry eye syndrome patients.
Generally, the diameter of therapeutic lens and BCR are important for the lens application and therapeutic function and for the cases wearing soft contact lens, a curve radius flatter than 3-5D is selected. In addition, at the time of wearing the lenses, the movement of the lens on the eye by 0.5-1.0 mm is ideal. However, in the cases with the maceration of epithelial cells, if the application was for treatment, a tight application, where lens movement is small and the base curve is slightly steep, is more beneficial than a looser lens to shorten the re-epithelization period. However, a tight application could induce hypoxia, and therefore after corneal re-epithelization the lens has to be switched to a basic alignment. Recently, to accelerate the epithelial healing after corneal refractive surgery, therapeutic lenses have been frequently used. At the time, since the center area of the cornea is flatter than the vicinity, lens application is different from the general therapeutic application of contact lenses. If keratometry value of the central area of the cornea becomes flatter than that after surgery, a space between the cornea and the lens is created. Consequently, it is applied loosely in the central area and the re-epithelization process would not be effectively facilitated. Therefore, in such cases, if a flatter therapeutic lens was used, the central area forms a relatively tight application, and accelerates re-epithelization. On the other hand, if overly flat lenses were used, the movement of the therapeutic lenses increases substantially and it may impede the healing of the epithelium. Therefore, taking into consideration the alignment of both the central and peripheral area, lenses in which movement is small and a slightly tight application to the central area should be selected. As seen in our study as well as others, if the difference of the BCR of the lens used and the postsurgical curve radius were approximately 0.4-0.5 mm, it could help facilitate epithelium healing.
In regard to therapeutic lens use associated with refractive correction surgery in Korea, Sohn et al14 found that immediately after the epikeratoplasty, the difference of the corneal epithelium regeneration time was not found to be equal to that of a pressure patch. After PRK, according to Choi et al15 the corneal epithelial defect showed faster regeneration in the group using therapeutic contact lens versus pressure patches. Yeom et al16 who used amniotic membrane after LASEK surgery, claimed that a significant difference in the mean epithelium regeneration time was not observed; nonetheless, the visual acuity 6 months after surgery was better in the amniotic membrane group than in the group that used therapeutic lenses. In addition, with regard to the mechanism, it was speculated that the amnion serves as a mechanical barrier and secretes growth factors. Therapeutic lenses also act by a similar mechanism, and in particular, they play a role as a mechanical barrier. In the study by Gemoules,17 it was reported that after LASEK surgery, instead of soft therapeutic lenses, RGP lenses were used and better visual acuity could be anticipated in those patients whose prognosis was thought to be poor due to high aberration.
In conclusion, a flat therapeutic lens, of which the difference between the BCR of the lens and the BCR by postsurgical corneal topography is approximately 0.5 mm, compresses the central area appropriately and thus reduces the edema of the corneal epithelium, thereby facilitating the adherence of the corneal epithelial flap. However, if an overly flat lens is used, its movement on the corneal surface can become excessive and thus can deteriorate the stability of the flap.



 XML Download
XML Download