

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Retinal capillary hemangioma (RCH) is an uncommon benign vascular tumor of the retina that can occur sporadically or in association with von Hippel-Lindau (VHL) syndrome. It was first described by Fuchs in 1882.1-3 RCH is the most frequent and the earliest manifestation of VHL disease. Therefore, an ophthalmologist is frequently involved in the care of patients with VHL.4 It is not clear whether RCH that occurs without a family history5 is most commonly sporadic or most commonly represents an initial manifestation of VHL.6,7 RCH lesions often lead to visual loss secondary to hemorrhage into the vitreous, retina, or subretinal space. They can also lead to macular edema or exudative retinal detachment.8 Various forms of therapy have been attempted, but all have inherent problems with efficacy or with side effects such as transiently increased exudation or epiretinal membrane formation.8 A wide variety of treatment methods have been described for angiomatous lesions of the retina.8 Laser photocoagulation is effective for small angiomatous proliferations but is not effective for large lesions, particularly those associated with pronounced exudation and hemorrhage.8 Even without overlying media opacity, thermal laser photocoagulation probably has a limited depth of treatment, leaving a large amount of viable and potentially problematic vessels.9 Cryotherapy may be more effective in eventually closing the vessels in thicker lesions, but this treatment is associated with a transient increase in the amount of exudation present.10 Radiation therapy has been used, but it has the potential for causing significant long-term complications. Photodynamic therapy (PDT) with verteporfin has been used for the treatment of choroidal neovascularization in age-related macular degeneration.10 When activated, verteporfin appears to cause oxidative damage to the vascular endothelial cells.9 This damage leads to vascular occlusion, although the surrounding tissue is preserved.8
We report the first case of retinal capillary hemangioma treated with verteporfin photodynamic therapy combined with intravitreal triamcinolone injection.
Case Report
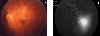
A 15-year-old female presented with metamorphopsia in the left eye for 7 days. Her best-corrected visual acuity (BCVA) was 20/20 in the right eye and 20/50 in the left eye. The intraocular pressure was within normal limits bilaterally, and the results of anterior segment examinations were unremarkable. The right fundus was normal. The left fundus revealed mild macular edema and hard exudates (Fig. 1A). At the 5 o'clock periphery lay a circumscribed exophytic retinal capillary hemangioma approximately 2.5 disc diameter (DD) with a prominent dilated and tortuous feeding artery and draining vein (Fig. 1B). Fluorescein angiography was performed, and fluorescein was evident in the dilated feeder arteriole (Fig. 1C, 1D). The retinal tumor had fine capillary filling, which rapidly became homogeneous (Fig. 1C).
The drainage vein became prominent in the venous phase, while the tumor demonstrated progressive hyperfluorescence with late leakage of dye into the surrounding structures (Fig. 1C). Optical coherence tomogram (OCT) of the fovea demonstrated cystic intraretinal edema (Fig. 1E).
B-scan ultrasonography demonstrated a well-demarcated exophytic retinal lesion without choroidal effects (Fig. 1F). The patient had no family history of ocular or systemic disease. Since retinal capillary hemangioma seemed a likely diagnosis, a systemic examination for VHL syndrome - including magnetic resonance imaging of the brain, abdominal computed tomography scan, and urine tests for catecholamines - was performed. Results were negative. Genetic testing for VHL syndrome was not performed.
Three days after initial PDT, intravitreal triamcinolone (IVTA) was planned. Verteporfin photodynamic therapy was performed using 6 mg/m2 body surface area (BSA) of intravenous verteporfin delivered over 10 minutes. Fifteen minutes after the start of infusion, a laser light at 689 nm delivered 50 J/cm2 at an intensity of 600 mW/cm2 over 83 seconds using a spot size of 7500 μm directed to the hemangioma with a Mainster widefield contact lens.10
Three days after PDT, the patient returned to the hospital for IVTA. BCVA declined to 20/160 in the left eye and cystic intraretinal edema worsened, shown by optical coherence tomogram of the fovea (Fig. 2B). A pre-injection single drop of povidone-iodine (5%) solution was applied to the eye followed by thorough cleaning of the eyelashes and application of a lid speculum. 0.5% proparacaine hydrochloride drops (Alcaine®, Alcon) was applied topically. Triamcinolone acetonide in a single-use bottle (40 mg/ml, 1 ml bottle) was drawn into a 1-cc tuberculin syringe after cleansing the top of the bottle with an alcohol wipe. A separate 30-gauge needle was placed onto the syringe, which was then inverted to remove air bubbles. The excess triamcinolone was discarded until 0.1 ml (4 mg) remained in the syringe. The stab was given 3.5 mm from the limbus (pas plana) in the inferotemporal quadrant. The needle was removed simultaneously with the application of a cotton-tipped applicator over the entry site to prevent regurgitation of the injected material. Indirect ophthalmoscopy was used to check for central retinal artery (CRA) pulsation, a drop of topical antibiotic solution was administered, and the eye was patched. The patient was put on a post-injection course of topical antibiotic eye drops for a week.
Twelve days after PDT, BCVA had improved to 20/100 in the left eye and the retinal capillary hemangioma had undergone partial involution (approximately 2.5 DD). The feeder and draining vessel diameters had decreased by approximately 50% and 30%, respectively (Fig. 3A). Optical coherence tomogram of the fovea demonstrated improvement of cystic intraretinal edema (Fig. 2C).
Twenty-two days after PDT, BCVA had improved to 20/40 in the left eye and the retinal capillary hemangioma had regressed approximately 1.5 DD. The feeder and draining vessels were straighter but the diameter remained the same (Fig. 4A). Fluorescein angiography demonstrated decreased early filling and late leakage of the hemangioma (Fig. 4C). The optical coherence tomogram demonstrated restoration of the foveal contour (Fig. 2D).
Three months after PDT, BCVA had improved to 20/30 in the left eye and the retinal capillary hemangioma had regressed approximately 1.0 DD (Fig. 5B). The macular hard exudate and edema had improved (Fig. 5A).
Five months after PDT, BCVA had improved to 20/25 in the left eye and the macular hard exudates had disappeared (Fig. 6A). Regular follow-up of the patient is planned.
Discussion
Retinal capillary hemangiomas (RCH) are capillary angiomatous harmatomas of the retina and optic nerve head.4 Capillary hemangioma (angiomatosis retinae) of the retina occurs in two ophthamoscopically distinct forms: the peripheral lesion (known as the von Hippel tumor) and the juxtapapillary tumor.4 These tumors can occur anywhere in the fundus, although most commonly they are peripheral and endophytic.9 Either type of tumor may be either an isolated retinal vascular abnormality or one of the many systemic abnormalities in von Hippel-Lindau disease (VHL).4
Regardless of systemic association, the retinal tumors appear identical clinically and histopathologically.4 But patients with solitary retinal capillary hemangioma present a serious dilemma because RCH may or may not be associated with VHL disease. In a recent study, the probability of VHL disease in patients with solitary retinal capillary hemangioma was mathematically estimated to be 30% to 46%, but it varied from 45% in the preteen patients to less than 1% in those over 60 years old.11,12 Because the patient described in this paper is a young woman who showed peripheral exophytic retinal capillary hemangioma, she must be regularly and systemically examined for VHLsyndrome.
Most RCH progressively enlarge and there is progressive subretinal exudation, frequently leading to total retinal detachment and eventual blindness.13 Therefore, early detection and treatment of RCH is associated with good visual outcome.14 In general, the decision to treat RCH and the method of management is determined by the size, location, and associated findings, such as the extent of subretinal fluid, evidence of retinal traction, and overall effect or threat of clinical findings on the visual potential of the eye.2 Most commonly, RCH is managed by observation, laser photocoagulation, cryotherapy, plaque radiotherapy, and vitreoretinal surgery.2 All treatment options were discussed in detail with the patient. Because of the risk of hemorrhage and proliferative vitreoretinopathy with cryotherapy, and the limitations of laser photocoagulation in the presence of a large hemangioma with extensive subretinal fluid, vertepofin photodynamic therapy (PDT) was offered to the patient. The successful use of PDT in RCH has been reported by several authors.8,10 Atebara described three sessions of PDT for RCH in one patient, which resulted in decreased leakage during fluorescein angiography, but did not mention the degree of the tumor involution.10 Rodriguez-Coleman et al. reported two patients treated with PDT who showed marked and rapid regression of the angiomatous proliferation of vessels, but made no mention of the change in tumor size.8
Verteporfin PDT in the treatment of exudative RCH has theoretical advantages over conventional treatments of laser photocoagulation and cryotherapy.15,16 But the use of direct photocoagulation can potentially cause hemorrhage and exudative retinal detachment (ablatio fugax).4,17,18 On the other hand, the infrared-wavelength laser of PDT effectively penetrates through subretinal fluid and deeper into a large hemangioma than does laser photocoagulation.19 PDT may be less likely to result in hemorrhage and PVR than would cryotherapy.19 PDT actually represents the combination of pharmacologic therapy and laser-based therapy.20 Photosensitizers have biophysical properties well- suited to the thrombotic closure of abnormal neovascularization while preserving normal physiologic vessels.20
Photosensitizers also bind selectively to abnormal neovascularization, the vessels of which express more lipoprotein receptors than do normal mature vessels.20
During this patient's therapy, a temporary increase in macular exudation occurred after PDT, but other complications such as exudative retinal detachment were not found. Intravitreal triamcinolone acetonide was performed as a treatment for the increased exudation, whether the vascular tumor itself or the PDT caused the increase.21
Corticosteroids have a significant anti-angiostatic capacity.22 The primary mechanism of action of angiostatic steroids appears to be in aiding breakdown and blockage of the formation of capillary endothelial basement membranes.22 Triamcinolone acetonide appears to modulate the permeability and adhesion of human choroidal endothelial cells in culture.23 Penfold et al. demonstrated that cytokine-induced expression of intracellular adhesion molecule-l is down-regulated by triamcinolone acetonide.23 Wang et al. demonstrated that matrix metalloproteinases were down-regulated following incubation with triamcinolone, suggesting that the active remodeling of the extracellular matrix necessary for neovascularization can be inhibited.24 Ciulla et al. showed that intravitreal triamcinolone acetonide completely inhibited laser-induced choroidal novascularization in rats.25 These experiments provide rationale for using triamcinolone acetonide to treat choroidal neovascularization in exudative macular degeneration and other retinal vascular diseases. RCH is a benign vascular tumor of the retina;1-3 therefore, the rationale for this approach is to decrease the number of photodynamic treatments by combining the angiostatic properties of triamcinolone aetonide with the vascular occlusion induced by ocular PDT.
In this report of a single case of retinal capillary hemangioma with short follow-up, verteporfin PDT combined with intravitreal triamcinolone acetonide appeared to cause involution of the hemangioma with reduction in macular edema and improvement in visual acuity. The authors believe the treatment modality used in this case was more effective than verteporfin PDT alone would have been.





 XML Download
XML Download