

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Fibrofolliculoma is a clinically asymptomatic, 2-4 mm, skin-colored, dome-shaped smooth papule. It usually arises in the form of multiple lesions in adults in different areas such as the scalp, forehead, face, and neck. According to histology, the lesion is a fibrotic hamartoma characterized by infundibular epithelial proliferation and perifollicular fibrous proliferation. The lesion was first described by Birt et al. in 1977, and 15 cases have been reported since then.1 The reported cases were all multiple lesions; all had autosomal dominant inheritance and presented as trichodiscoma, acrochordons, and connective tissue nevus. Histological exams revealed the lesions to be clinical entities somewhere between perifollicular fibroma and trichofolliculoma.2
Solitary fibrofolliculoma was first reported by Scully et al. in 1984. They described a lesion arising in the mandibular area of a 62-year-old female.
Contrasted with multiple lesions, solitary fibrofolliculoma is rare, nonhereditary, and unassociated with other skin abnormalities.3 We herein report the first case of a solitary fibrofolliculoma found in the eyelid, exhibiting typical clinical and histological features in an otherwise-healthy 37-year-old woman.
Case Report
Clinical History
A 37-year-old female patient reported to the OPD with a palpable lesion in the central part of the right upper eyelid. The lesion had been palpable for one year before the patient visited the authors' clinic, and the patient had already visited a local clinic. With a diagnosis of chalazion, the patient had received incisional curettage twice, but the condition had not improved and had recurred several times.
Ophthalmic examination performed in the authors' clinic revealed that the patient's visual acuity was 20/20 bilaterally. The 5×5 mm lesion arose in the upper lid and was scarlet and smooth. It was a bean-sized and relatively solid nodule; palpation did not elicit any pain (Fig. 1A). The anterior segment was otherwise normal, as were the results of the fundoscopic examination.
Under local anesthesia, a pentagonal wedge resection was performed, including removal of 3 mm of extra lid tissue from the margin of the lesion and reconstruction of the upper eyelid. The authors observed the lesion carefully, marked a 10×10 mm pentagonal area including the lesion on the upper lid, and made a full-thickness excision of the marked area. The authors then performed lateral cantholysis, pulled on the upper lid laterally, temporally sutured the lid margin with 6-0 black silk, aligned the lid plate, and stabilized the lid plate with a 6-0 absorbable suture (half thickness). The upper lid margin was then sutured at 3 lines (the meibomian gland orifice, the gray line, and the lash line) with 6-0 black silk. The excision was finished after the skin suture with 6-0 black silk. The stitches were removed 5 days after the operation.
One week after the operation, slit lamp examination revealed multiple corneal erosions as well as abrasion. Lid fissure narrowing also occurred, resembling the clinical findings of ptosis. Antibiotic eye drops and artificial tear drops were prescribed.
Two weeks after the operation, the patient complained of pain in the right eye, and on slit lamp, the authors could see corneal erosion spreading throughout the cornea. Lid fissure had widened since the 1-week postoperative exam. The patient was given a therapeutic soft contact lens and analgesics, and the authors recommended continuous use of eye drops.
One month after the operation, the patient's ocular pain had improved, and she had no particular discomfort. Slit lamp examination revealed that the patient's cornea had healed, and swelling in the upper lid and lid fissure improved as well.
Eleven months after the operation, the height of the right upper lid was almost identical to that of the left.
During the past two years, the shape of upper lid has been holding up very well, and the lesion has not yet recurred (Fig. 1B).
Histopathologic Findings
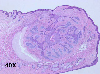
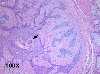
Histological examination revealed a well-defined tumor mass involving a group of adjacent pilosebaceous follicles and proliferative epithelial cords and spurs in the center, with a surrounding fibromucinous mesenchymal component (Fig. 2). Characteristic proliferating infundibular epithelial strands with perifollicular fibrous reaction anastomosing to form an epithelial network were also observed (Fig. 3). Pathological examination confirmed the diagnosis of fibrofolliculoma. The authors reexamined the patient's skin on the face, neck, axillae, upper trunk, and groin but obtained no particular findings. The patient indicated that she had no family history of multiple skin papules or any skin diseases. The authors made the final diagnosis of solitary fibrofolliculoma.
Discussion
Fibrofolliculoma was first described in 1977 by Birt, Hogg and Dubé.1 They reported 15 members of a family with numerous small popular skin lesions that proved to be pilar hamartous involving both epithelial and fibrous tissues associated with trichodiscomas and acrochordons. As mentioned above in this report the name "fibrofolliculoma" was introduced for the previously unrecognized tumor. Thereafter, this syndrome has been known as the Birt-Hogg-Dubé syndrome. Multiple lesions usually appear after the age of 25 and show autosomal dominant inheritance, but sporadic cases have also been reported.4
Most reports of multiple fibrofolliculomas have been associated in various combinations with trichodiscomas, acrochordons,1,2,4 perifollicular fibromas,5 and connective tissue nevus.2 Only two cases have been presented in the pure form unassociated with other significant cutaneous findings.6, 7
Solitary fibrofollicular is less common; to the authors' knowledge, only five cases have been published worldwide before this case study.3,6,10-12 Moreover, the case presented here may be the first case of a solitary fibrofolliculoma found localized in the eyelid.
Clinically, fibrofolliculoma is asymptomatic and presents with 2-4 mm lesions that are yellow-white to skin colored, smooth, and dome-shaped. The lesions look quite similar to those of other follicular neoplasms that involve mesenchymal proliferation, such as perifollicular fibroma and trichodiscoma, whose origin is purely adnexal mesodermal, without epithelial proliferation, or angiofibroma.8 In the spectrum of benign follicular neoplasms, fibrofolliculoma appears to be intermediate between perifollicular fibroma (purely of mesodermal origin) and trichofolliculoma (purely of epithelial origin).3 Therefore, a fibrofolliculoma is sometimes thought to be indistinguishable from these. However, a fibrofolliculoma frequently has visible central hair, keratotic plug, dell, or umbilication, whereas trichofolliculoma has features of telangiectasia and peripheral location of hair that may help distinguish it from fibrofolliculoma.9 Also, multiple follicular neoplasms are scattered over the face, trunk and extremities, but all of the reported solitary types involve lesions on the face.
Generally, the age of onset for solitary fibrofolliculoma is the sixth decade, in contrast to the much earlier onset (in the third decade) of the multiple hereditary form.3 However, reports of solitary fibrofolliculoma in Korea reveal that the lesion has arisen in patients between 1 and 36 years of age, indicating that the lesion can arise in patients at any age.10,11
Because patients have no recognizable or systemic symptoms and because solitary fibrofolliculoma is rare, the diagnosis can be difficult. The patient in our study had previously gone to a local clinic complaining of a painless, solitary mass, and under the diagnosis of chalazion, she had received only incision and curettage. The diagnosis of fibrofolliculoma can be easily overlooked unless one carefully examines the shape of the lesion and recognizes its distinct configuration.
Histopathologically, fibrofolliculoma has distinctive features with minor variations. The center of the lesion shows a hair follicle that is sometimes dilated and contains keratin material with a moderately well-circumscribed thick mantle of fibrous tissue surrounding it.
The infundibular follicular epithelium extends out into this fibrous mantle forming epithelial strands, cords, or spurs (Fig. 2). The infundibular follicular epithelium may just extend outward, it may rejoin the follicle and adjacent skin, or it may anastomose with each other. In the three-dimensional view, the infundibular follicular epithelium actually forms septa within the fibromatous mass, forming an "epithelial sponge." Special staining shows that the fibrous tissue stroma contains a high content of mucin substances and extremely sparse or absent elastic tissue in contrast to adjacent normal dermis.1,2
In conclusion, a solitary fibrofolliculoma is generally diagnosed by histopathological exam after excision and biopsy, and one can very easily miss the diagnosis with a simple ophthalmic examination when the patient presents with an asymptomatic lesion arising in the eyelid. Because most solitary fibrofolliculomas do not recur after a simple excisional procedure, one should operate on patients with asymptomatic eyelid lesions, after confirming the histopathologic diagnosis; the pathologist should be able to differentiate the lesion from malignant conditions such as basal cell carcinoma. Also, when this type of a lesion in the eyelid is observed, a diagnosis of fibrofolliculoma should be considered, despite its rare occurrence.

 XML Download
XML Download