

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Anterior chamber injection is a useful drug delivery route for controlling endophthalmitis during intraocular operation. Various drugs, such as antibiotics, steroids, lidocaine, and epinephrine have been used in anterior chamber injection, but can induce endothelial toxicity. Subconjunctival injection of antibiotics and mixing antibiotics with intraocular irrigating solutions are common procedures to prevent postoperative endophthalmitis after cataract operation.1-3 Theoretically, these antibiotics are expected to reduce the risk of endophthalmitis, and they have been used clinically for endophthalmitis treatment, but adequate concentration of the antibiotics (in order to prevent infection without endothelial toxicity) has not yet been fully investigated.4-7 Moreover, there are no case reports dealing with endothelial toxicity after anterior chamber injection of high dose antibiotics.
Here, we report a case of inadvertent anterior chamber and corneal stromal injection with high dose antibiotics and steroids during cataract operation, and subsequent management and complications.
Case Report
A 78 year-old woman underwent extracapsular cataract extraction with phacoemulsification via temporal clear corneal and a single superior side port incision. An intraocular lens was inserted in the bag, and viscoelastic materials were removed by irrigation and aspiration, without any complications. At the end of the operation, the nurse inadvertently handed over the wrong syringe and, and high dose antibiotics and steroids were inadvertently injected into the anterior chamber and corneal stroma through a 19G needle during the stromal hydration procedure for wound closure at the incision sites. The antibiotics and steroids given were gentamicin (20 mg/0.5 ml) and dexamethasone (2 mg/0.5 ml), originally prepared for subconjunctival injection. About 10 seconds after the injection, we recognized the mistake, and the anterior chamber was irrigated with 100ml of a balanced salt solution (CYTOSOL OPHTHALMICSTM) for one minute.
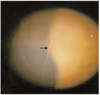
On postoperative day one, the patient complained of blurred vision and foreign body sensations. Severe corneal edema and Descemet's membrane folds invading the visual axis were seen extending from the 12 to 4 o'clock position (Fig. 1). Inflammatory cells and flares were 3+ in the anterior chamber. Best-corrected visual acuity was 0.2, and intraocular pressure was 18 mmHg by noncontact tonometer. Postoperatively, Cravit® (levofloxacin 0.5%, Santen, Osaka, Japan), 1% prednisolone, and 5% NaCl were administered every two hours. Oral prednisolone (20 mg) and ofloxacin (300 mg) were used as well. A pressure patch with ofloxacin and dexamethasone ointment was administered during sleep. The corneal edema persisted until postoperative day three, and the best-corrected visual acuity decreased to 0.15. The vision improved to 0.4 after two weeks, but the corneal edema persisted without improvement. The patient continued with the original and medications and dosages. On the third postoperative week, the best-corrected visual acuity stabilized at 0.4, and the corneal edema began to resolve. The visual acuity continued to improve to 0.7, and the corneal edema finally resolved four weeks postoperatively. However, the linear Descemet's membrane folds persisted up to postoperative week 16 (Fig. 2, 3). At the same site of the Descemet's membrane fold, corresponding endothelial damage was also observed, manifesting as a definite dark acelluar area on specular microscopy (Fig. 4). The preoperative endothelial cell density on specular microscopy was 2717 cells/mm2 and the mean cell size was 368 µm2. At postoperative month three, the mean cell size was 424 µm2 and endothelial cell density had decreased to 2358 cells/mm2. No other changes were observed after that, and the best-corrected visual acuity improved to 0.8 at postoperative month four.
Discussion
Almost every ocular drug can be potentially toxic to the corneal endothelium, and the risk of endothelial toxicity is increased when used in the anterior chamber because of its direct contact to the endothelium. Corneal endothelium is vulnerable even to osmotic change or pH change of the irrigating fluid, and is easily damaged by electrolyte imbalance. Moreover, permanent endothelial dysfunction, cystoid macular edema, pupil dilation, and glaucoma due to destruction of trabecular meshwork can occur and have been reported in severe cases.8-10 Therefore, it is important to control the concentration of the solution when antibiotics are added to the irrigating solution in order to prevent postoperative endophthalmitis.1,2,4 However, the exact nontoxic concentrations of the antibiotics and steroids have not been fully investigated.
Montan et al.11 studied doses and exposure durations of cefuroxime when injected in the anterior chamber, reporting that 1 mg/0.1 ml of cefuroxime is safe and maintains a high concentration for one hour postoperatively. Kang et al.12 studied gentamicin toxicity in different concentrations on three types of human corneal cells under culture and suggested that the safe local concentration of gentamicin for endothelial and stromal cell was 1 mg/ml in the human eye. With increasing concentration of gentamicin (from 2 mg/ml to 4 mg/ml), the toxicity of gentamicin to the corneal cells was in direct proportion to its concentration and duration of incubation. The toxicity was the greatest on endothelium; the stroma was affected the least. Petroutsos et al.13 reported that endothelial toxicity occurred when 1 mg/ml of gentamicin was injected into the anterior chamber in rabbit eyes. Medin14 used a weight recording system to demonstrate the possible toxic effect of gentamicin on the endothelium of rabbit corneas stored in organ culture. They reported gentamicin toxicity of from concentrations of 3.0 mg/ml and higher. Lin et al.15 reported that 15% cell damage was found in tissue cultured bovine endothelial cells when exposed to 1.6 mg/ml of gentamicin. Damaged cells recovered their normal morphology after 24 hours. When the concentration of gentamicin was doubled, cell damage reached 40%, and the recovery of cellular morphology was much slower. They concluded that gentamicin should be rationally and carefully used in the intraocular space. Mester and Stein16 studied the effect of gentamicin concentration on rabbit endothelial cells and reported that 0.50% gentamicin was toxic to endothelium, but 0.25% gentamicin was not significantly different as compared to the control.
Besides irreversible damage to the corneal endothelium and corneal edema, high concentrations of gentamicin solutions can induce retinal hemorrhage, edema, and obliteration of the retinal vasculature when injected in the vitreous, resulting in optic atrophy, retinal pigment degeneration, or neovascular glaucoma.17,18 In our case, the toxicity of the gentamicin to the corneal endothelium was expected to be significant due to the fact that the concentration of the gentamicin injected in anterior chamber and corneal stroma was 40 times more than that of previously mentioned studies.
Wang et al.19 tested the cytotoxicity of five antibiotics (amphotericin-B, colistin-M, sulbenicillin, amikacin, cephradine) and a steroid (betamethasone) to cultured porcine corneal endothelial cells and demonstrated that the steroid was less toxic to the endothelium than other antibiotics.
In our case, the inadvertent injection of antibiotics and steroids resulted in severe corneal edema from 12 to 4 o'clock position involving the visual axis, along with extensive Descemet's membrane folds. The corneal edema persisted until four weeks postoperatively. We used a hypertonic solution of about 1720 osm/L (5% NaCl) topically to reduce the stromal edema. This concentration is known to be nontoxic,20,21 and the solution was effective in our case. On postoperative week 12, the Descemet's membrane folds were observed by specular microscopy and persisted 16 weeks after the operation. In our case, corneal edema and the Descemet's membrane fold were probably due to inadvertent corneal stromal injection with high dose gentamicin and dexamethasone rather than injection directly into the anterior chamber. The duration of exposure and the concentration of the drugs were negligible, due to prompt irrigation of the anterior chamber with balanced salt solution. We found the localized endothelial defect on specular microscopy manifesting as a definite dark acelluar area, which corresponded to the area of the Descemet's membrane fold and site of inadvertent stromal injection. Also, irrigation with a balanced salt solution might play a role in causing corneal edema.
On postoperative week four, the corneal edema resolved, and best corrected visual acuity improved to 0.7. Our case showed relatively good visual prognosis despite the high concentration of the injected antibiotics and steroids. This favorable outcome might be due to the immediate irrigation of the anterior chamber with balanced salt solution. As such, long-term endothelial exposure to high dose antibiotics and steroid can be avoided. The immediate irrigation was possible because the balanced salt solution was prepared before the operation. Hansany and Basu22 demonstrated that a 0.1 mg/ml concentration of gentamicin was not toxic to the corneal endothelium until seven days postop, but after seven days corneal endothelial toxicity was demonstrated for that concentration. This study suggested that duration of drug exposure (rather than drug concentration) is also an important factor for corneal endothelial damage. Therefore, considering our case and this study, we can conclude that immediate irrigation of the anterior chamber is important in preventing corneal endothelial damage when high dose antibiotics and steroids are injected in anterior chamber by mistake during cataract or other intraocular surgery. To dilute the intrastromal antibiotics and steroids, we considered stromal injection of a balanced salt solution, but this was not performed because separation of Descemet's membrane from stroma can occur.
McDonald et al.23 insisted that clear communication between the surgeon and nursing staff, in addition to precise labeling of every injectable solution, is necessary to prevent accidents, such as this. Antibiotics in particular can be confused with a balanced salt solution. In addition, it is wise to draw up injectable antibiotics just before injection, and to use different gauge needles for the different solutions, which could easily be recognized by physician under the microscope.
In our case, we reported a favorable visual outcome with immediate irrigation of the anterior chamber with a balanced salt solution after the inadvertent injection of high dose antibiotics and steroids. However, to prevent such an accident during surgery, strict precautions (mentioned previously) and clear communication between surgeons and nursing staff, including scrub nurses, are considered to be of great importance.



 XML Download
XML Download