

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Peripheral anterior synechiae (PAS) refers to a condition in which the iris adheres to the angle. PAS can develop in various ocular conditions, including: ocular inflammation, a post-traumatic condition, after cataract surgery, or with an iris bombe in a pupillary block glaucoma. In acute angle-closure glaucoma (ACG), repeated or prolonged episodes of appositional closure of the angle may eventually lead to PAS formation. Moreover, asymptomatic synechial closure of the angle may result in chronic ACG, especially in Asian people.1-3
The classifications of ACG are various and arbitrary. PACG may not be a single entity, but a number of different disorders share a final common pathway involving the formation of irreversible synechial adhesion between the peripheral iris and the trabecular meshwork.4 Few studies have attempted to evaluate PAS morphologically. Therefore, we undertook this study to evaluate the characteristics of PAS overall and according to the different ACG subtypes.
Materials and Methods
Patient information was collected from the charts of all patients who were diagnosed as having PACG at the Korea University Hospital between 1994 and 2004. Patients who had undergone intraocular surgeries were excluded. Patients with PACG were divided into four subtypes according to Kim and Jung's classification system (Table 1).5 Acute ACG was diagnosed in eyes with high IOP (intraocular pressure), a gonioscopically closed angle, and acute symptoms such as ocular pain, redness, and blurred vision. Chronic ACG was diagnosed in eyes with a closed angle and changes to the optic disc and visual field. Angle closure hypertension was diagnosed in eyes having a closed angle and raised IOP levels (>21 mmHg) but without changes to the optic disc and visual field. ACG suspect was diagnosed in eyes with an occludable angle but no other ocular abnormality. Dynamic gonioscopy was performed by one author (YYK).6-7 The examination was carried out at the lowest level of ambient illumination using a Goldmann-type three-mirror lens (Model OG3MS, Ocular instruments. Inc., USA). Redirection of a patient's gaze to a mirror and exertion of pressure on the cornea were done to widen the angle, and this allowed for the clear identification of the angle status. Spaeth's convention was used to grade the drainage angle.
PAS was classified according to the adhesion width. PAS limited to 15 degrees was designated as narrow PAS, a spread from 15 to 30 degrees as medium PAS, and a spread greater than 30 degrees as broad PAS. The entire angle width was divided into twelve sectors of 30 degrees using an adaptation of the system described by Inoue et al (Fig. 1).8 Sectors 12 and 1 were designated as the "superior part", sectors 2-5 as the "nasal part", sectors 6 and 7 as the "inferior part", and the remaining four sectors as the "temporal part".
Statistical analyses were performed using SPSS version 10.0 (Windows; SPSS Inc., Chicago, IL). The prevalence and width of PAS according to PACG subtype were compared using the chi-square test and Fisher's exact test respectively. The extent of PAS in PACG subtypes was compared by an ANOVA test. Correlation and linear regression analysis were used to evaluate the relationships between the highest IOP levels and the extent of PAS prior to medication or the other forms of treatment.
Results
Two hundred and forty-four eyes of 155 PACG patients (35 males and 120 females) were enrolled in this study. The average age of patients at the time of last visit was 65.1 ± 8.6 years. All patients were Korean. There were 123 right eyes and 121 left eyes tested. The numbers of eyes in each PACG subtype were: 94 ACG suspect, 10 angle closure hypertension, 73 chronic ACG, and 67 acute ACG. PAS was most prevalent in eyes with angle closure hypertension (9/10, 90%) and least prevalent in eyes classified as ACG suspect (20/94, 21.3%) (Chi-quare test, P<0.0001). The prevalence of PAS in eyes with acute ACG was 70.1% (47/67) and 80.8% in eyes with chronic ACG (59/73) (Table 2).
Two hundred and eight incidents of narrow, medium, and broad PAS were found in the 244 eyes. In eyes with acute or chronic ACG, broad PAS was more frequent than narrow PAS, whereas in eyes of the angle closure hypertension or ACG suspect, narrow PAS was more frequent than broad PAS (Fisher's exact test, P<0.0001) (Table 3).
The width of PAS was statistically different with respect to PACG subtype (ANOVA test, P<0.05) (Table 4). Eyes with chronic ACG had the highest average degree of angle-closure with PAS, whereas those in the ACG suspect had the least average degree of angle-closure (multiple comparison, Duncan test, P<0.05). The difference between angle-closure hypertension and chronic ACG with respect to average degree of angle-closure with PAS was also significant (multiple compa-rison, Duncan test, P<0.05).
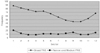
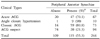
Of the 976 parts of the 244 eyes inspected (4 parts per eye), 401 had PAS. PAS was most frequently found in the superior part of the eye and least frequently in the inferior part (Table 5). Of 2928 total sectors inspected in 244 eyes (12 sectors per eye), PAS was most frequently found in sector 1 and least frequently found in Sector 10 (Fig. 2). LI was implemented in 82.7% of eyes (201 eyes). The highest IOP levels (mmHg) before LI and medication was 53.78±13.63 in Acute ACG, 26.40±2.03 in Angle closure hypertension, 37.87±16.47 in Chronic ACG, and 15.84±2.57 in the ACG suspect (Table 4). The highest IOP levels before LI and medication were found to be significantly correlated with the extent of PAS in eyes with chronic ACG (r=0.423, P<0.0001). However, no significant correlation was found in the eyes of the other subtypes (Table 6). Linear regression analysis demonstrated a mild but significant relationship between the highest IOP levels before treatment and the extent of PAS with chronic ACG (r2=0.168, P<0.0001).
Discussion
In PACG, the duration of closure by contact necessary to cause synechial closure appears to vary greatly from patient to patient. Asian irides are thicker and stickier than other ethnicities, and therefore tend to form PAS more easily.9 Gonioscopy was used to evaluate the prevalence, width, and distribution of PAS overall and within the different PACG subtypes in this study.
Gonioscopy is an important modality for the evaluation of ACG patients. It is not always easy to determine the status of the angle, especially when it may be narrow rather than open or closed. Our study found a PAS prevalence of 70.1% in acute ACG, 90% in angle closure hypertension, 80.8% in CACG, and 21.3% in ACG suspect. No PAS was found in the 14 eyes with CACG, of which four had plateau iris configurations. This suggests that the presence of PAS may be not essential for the diagnosis of chronic ACG. In eyes with ACG suspect or angle closure hypertension, narrow PAS was more frequent and the average PAS angles were lower than in eyes with chronic or acute ACG. This implies that PAS is narrow in earlier stages of PACG and becomes broader in later stages.
Several studies have evaluated the topographic distribution of PAS. Barkan10,11 mentioned that PAS tends to first occur superiorly in angle and Philips reported that PAS is most common in the superior sector.12 Inoue et al8 reported that broad PAS exceeding 30 degrees was most frequent in the superior sector and they found that narrower PAS showed no pattern of location. Mok et al13 suggested that superior and temporal portions of the angle might be the earliest sites of angle occlusion in chronic ACG, because the incidence of synechial angle closure was higher in superior and temporal quadrants than others. This phenomenon has been interpreted in several ways. Barkan10-11 suggested that it might be due to the weight of the aqueous column in the anterior chamber, whereas Philips concluded that PAS tends to occur in the superior part of the eye because it has a relatively narrower angle than other parts of a normal eye. A normal lens decentralizes superiorly to the corneal center, where the temporal border lies behind the nasal border,14 and the pressure of the upper eyelid may therefore cause the peripheral cornea to flatten in the superior part of the eye.14 In addition, the incidence of PACG increases while the anterior chamber angle becomes more narrow with age, especially in the superior quadrants in Japanese.15 In our study, of the 976 parts inspected in 244 eyes (4 parts per eye), PAS was most frequently found in the superior part of the eye.
Our results also show that the incidence of broad PAS (exceeding 30 degrees) was highest in the superior sectors, but that medium and narrow PAS were distributed throughout the 12 sectors relatively equally (Fig. 2). Inoue et al reported similar results, and suggested that the discrepancy between previous studies might have been due to the gonioscopic methods used.8 Inoue et al used pressure gonioscopy to observe the angle recess. They also mentioned that it was not easy to recognize narrow PAS with the conventional gonioscopy used by Philips, because it was mostly adherent to the posterior structure.8 We used pressure gonioscopy to investigate the nature of PAS, and our results support those of Inoue et al. If narrow to medium PAS develop and later broaden with time, the progression of PAS into broad PAS may occur more easily in the superior part than in other parts of the eye.
We compared the extent of PAS to the highest IOP levels prior to any medical or laser treatments according to the different subtypes. Aung reported that the extent of PAS was associated with higher levels of IOP in untreated eyes with chronic ACG.14 Our results also showed that the highest IOP levels before treatment were correlated with the extent of PAS in eyes with chronic ACG; however, no significant correlation was found for the other clinical subtypes. These results imply that the synechial closure of the angle is an important mechanism of raising IOP levels in eyes with chronic ACG.
In conclusion, PAS was found to be narrow in the ACG suspect and angle-closure hypertension and broader in the acute ACG and chronic ACG subtypes. PAS was most frequently found in the superior part of the eye, which may be due to related anatomical structures, such as the weight of aqueous fluid, a decentralized lens, or corneal flattening due to upper eyelid pressure. In addition, synechial closure of the angle may play an important role on raising IOP levels in the later disease stage.






 XML Download
XML Download