

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Blepharitis is a relatively common disorder that manifests various clinical signs such as foreign body sensation, tearing and dry sensation, etc. The complete treatment of this condition is believed to be difficult because of abnormal meibomian gland function and changes in the normal flora of conjunctiva. Consequently, the course is often chronic, frustrating both clinicians and patients. Meibomian gland dysfunction is a common type of chronic blepharitis and although it is so common it can be easy to overlook clinically. Because symptoms can improve with appropriate treatment, it is very important to identify the disorder in patients who complain of dry eye symptoms.
Chronic meibomian gland dysfunction particularly affects the lipid layer of tear film, destabilizing the tear film and quickening the tear film's evaporation, and ultimately causes many disorders of the external eye, including dry eye syndrome.1
In order to treat this dysfunction, physicians have reported prescribing 200 mg twice-daily doxycycline (α-6 deoxy-5 hydroxytetracycline), a long acting analogue of tetracycline that inhibits collagenase and also has antichemotactic effects, thus improving patients' symptoms by stabilizing the lipid layer of tear film.2
Recently, in the field of dentistry, low-dose doxycycline hyclate (20 mg) has been used to treat and prevent periodontitis by inhibiting collagenase.3 The authors wanted to investigate the effectiveness of such therapy in the chronic meibomian gland dysfunction patients.
Materials and Methods
One hundred fifty patients were selected (55 male, 95 female) that reported to the department of ophthalmology between January and December of 2003 and newly diagnosed with chronic meibomian gland dysfunction with grade 2 or worse meibomian gland destruction or meibomian gland orifice obstruction, and whose symptoms failed to improve despite warm compression, lid massage, lid scrub, and topical eye drops or ointment therapy for more than 2 months.
With these patients, the authors conducted a randomized prospective study and obtained informed consent. Both the nurses that distributed the medication and the patients were blinded to medication and treatment group.
The patients were divided randomly into 3 groups according to dosage of doxycycline. The first group, which consisted of 50 patients (100 eyes), was given 200 mg of systemic doxycycline (doxycycline monohydrate, VIRADOXYL-N®, Jin-Yang pharmacy) twice a day. The second group of 50 patients (100 eyes) received 20 mg of systemic low dose doxycycline (doxycycline hyclate, DENTISTAR®, Ha-Na pharmacy) twice a day. The third group, consisting of 50 patients (100 eyes), received placebo.
According to pharmaceutical data, when a high-protein or high-lipid diet is ingested with doxycycline, the drug absorption can be reduced and maximum concentration of the drug in the blood is reached very slowly. Accordingly, the authors instructed the patients to take the capsules twice a day, before breakfast and bedtime. Before treatment began, the patients were asked to record their symptoms, including irritation, discomfort, foreign body sensation and ocular pain, and each patient underwent the TBUT and Schirmer test. All exams were conducted by a single physician (D.C.L.). In order to minimize any bias resulting from continual usage of eye drops, all topical therapy was stopped at least 2 weeks prior to beginning study medication. Tear break up time test was conducted as follows in both eyes. A drop of distilled water was added to fluorescein strip (Haag-Streits, Switzerland), and was instilled underneath the patient's inferior fornix. The patient was asked to blink 3 or 4 times and was examined using a slit lamp with maximum cobalt blue light. The patient was asked to open the eye widely and to look straight ahead, and the authors measured the time it took for a single black dot or line to appear on the cornea using a stop watch. The authors obtained this measurement three times and recorded the average.
10 minutes after the tear break-up time test, the Schirmer test was conducted on both eyes. The patients underwent the test without any topical anesthetic. A 5 by 35 mm sized Whatman filter paper strip was inserted in the lateral 1/3 of the inferior fornix and after five minutes, the length which had become wet by the tear film was measured.
The examination of the meibomian gland was performed after these two tests because examination of the gland can affect tear break-up time and Schirmer test results. The severity of meibomian gland destruction was determined using the following procedure. After turning over the lower lid, a transilluminator was placed underneath the lid's skin, and the meibomian gland tubules were observed through the slit lamp. The authors noted whether the tubules were arranged nicely into the shape of grapes. If everything was normal, a grade 0 was given. If 25% of the meibomian gland was destroyed, a grade 1 was given. A 25-50% destruction of the gland received a grade 2 and more than 50% destruction was classified as grade 3.
The degree of meibomian gland orifice obstruction was determined as follows. The patients were asked to look upwards and, with the index finger, the author pressed along the lower lid margin until meibomian expression could be witnessed. Under the slit lamp, the author examined the ease of meibomian expression as well as the color and turbidity of the expression and assigned a grade of 0 through 3 (Table 1).4 When the grade was worse than two in the respective category, the meibomian gland was said to have been destroyed or its orifice obstructed.
One month after performing these initial exams, the authors repeated all exams in each group to objectively ascertain any improvement in symptoms.
The authors gave patients a list of seven questions (Table 2) describing symptoms of typical dry eye syndrome,5 and recorded the number of questions marked by the patients. In order to ascertain improvements in subjective symptoms, the author categorized each patient into one of four different grades: complete remission, partial remission, no change and aggravation. The authors also recorded any signs of side effects of drug ingestion during each follow up visit.
PC-SPSS (version 10.0) was used for statistical analysis, specifically the ANOVA, paired t-test and chi-square tests. A p-value of less than 0.05 was designated as statistically significant.
Results
Among 150 patients, 55 were male and 95 female, and the average age was 47.2±12.36 years. After one month, 3 patients in the control group, 4 patients in the high dose group, and 4 patients in the low dose group were lost during follow up or stopped medication due to side effects. There was no statistically difference in gender or age between the 3 groups (Table 3).
Because all the patients exhibited a similar degree of meibomian gland dysfunction in both eyes at baseline, both eyes were included in the same group.
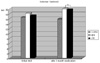
Before doxycycline was given, the tear break up time was 7.80±2.12 seconds for the control group, 7.78±2.07 seconds for the high dose group, and 7.82±2.16 seconds for the low dose group. There was no statistical difference among these groups (p>0.05, ANOVA). After doxycycline was given, the results were as follows: 7.84±2.02 seconds for the control group, 9.42±2.87 seconds for the high dose group, and 9.54 ±1.58 seconds for the low dose group.
There was no statistical difference in TBUT score in the control group before and after the treatment period (P=0.881, paired t-test). In contrast, both the high and low dose groups showed a statistically significant difference in score after treatment, when compared to baseline (p<0.05, paired t-test). However, the post-treatment scores were not significantly different between the high and low dose groups (P=0.992, ANOVA).
After doxycycline medication, there was a statistically significant difference between the control group and high dose/low dose group (p<0.05, ANOVA) (Fig. 1).
Before doxycycline medication was given, Schirmer test results were as follows: 16.57±4.43 mm for the control group, 18.13±3.87 mm for the high dose group, and 17.27±4.16 mm for the low dose group. There was no statistically significant difference among these groups (p>0.05, ANOVA). After medication, the results were as follows: 15.89±4.34 mm for the control group, 19.98±4.05 mm for the high dose group, and 19.65±5.02 mm for the low dose group.
There was no statistically significant change in Schirmer test results in the control group after the treatment period (P=0.347, paired t-test). Both the high and low dose group showed statistically significant changes in score after the medication was given (p<0.05, paired t-test). However, the post-treatment scores were not significantly different between the high and low dose groups (P=0.624, ANOVA).
After doxycycline treatment, there was a statistically significant difference between the control group and high dose/low dose group (p<0.05, ANOVA) (Fig. 2).
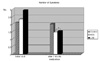
Before the treatment period, the number of symptoms reported per patient was as follows: 2.10±1.06 for the control group, 2.33±0.97 for the high dose group, and 2.92±0.77 for the low dose group. After the treatment period, the results were as follows: 2.01±1.23 for the control group, 1.45±0.62 for the high dose group, and 1.53±0.52 for the low dose group. For the control group, the number of reported symptoms did not change significantly after the treatment period (P=0.558, paired t-test). However, the high and low dose groups both showed statistically significant reductions in symptoms after the medication (p<0.05, paired t-test), although there was no significant difference between groups (P=0.304, ANOVA).
After doxycycline medication, there was a statistically significant difference in number of reported symptoms between the control group and high dose/low dose group (p<0.05, ANOVA) (Fig. 3).
Among the patients in the control group, the degree of improvement in the subjective symptoms was as follows: the no change group was the most numerous with 36 patients (76.59%), while the partial remission and aggravation groups were made up of 5 patients (10.64%) and 6 patients (12.77%), respectively. In the high and low dose groups, 30 patients (65.22%) and 32 patients (69.57%) were designated as the partial remission group, respectively, while the no change group contained 9 high dose patients (19.57%) and 11 low dose patients (23.91%). The aggravation group contained 5 patients in the high dose group (10.87%) and 2 patients in the low dose group (4.35%), and the complete remission group contained 2 patients (4.35%) and 1 patient (2.17%) from each dose class, respectively. There was no statistically significant difference between the two groups (P=0.288, chi-square test) (Fig. 4).
After one month of medication, cardinal side effects were reported by 3 patients (6.38%) in the control group, 18 patients (39.13%) in the high dose group, and 8 patients (17.39%) in the low dose group. Compared to the low dose group, the patients in the high dose group reported side effects more frequently, and the difference was statistically significant (P=0.002, chi-square test) (Fig. 5).
In all three groups, gastrointestinal problems (i.e., dyspepsia, nausea, diarrhea, etc.) were the most frequently reported side effects (21 patients), followed by itchy skin, urticaria and erythematous papules (7 patients), and stomatitis (1 patient).
In total, seven patients stopped medication because of side effects: 1 patient in the control group, 4 patients in the high dose group, and 2 patients in the low dose group.
Discussion
Blepharitis is a relatively common disorder which manifests various clinical signs, and the complete treatment is believed to be difficult because of abnormal meibomian gland function and changes in the normal flora of conjunctiva; the disorder often goes chronic, frustrating many clinicians and patients.
Meibomian glands form lobules that center around main tubules, which exist in the upper and lower tarsus. The lipids manufactured in these glands pass through the main tubules, and they are expressed through the meibomian openings, which are located between the epithelial skin and the gray line in the tarsus, ultimately forming a lipid layer of tear film.6
This lipid layer prevents tear evaporation and tear outflow, playing in important role in the stabilization of the tear film.7 When meibomian gland dysfunction occurs, tear film becomes destabilized, giving rise to dry eye symptoms such as foreign body sensation, eye fatigue, or epiphora.7-10
McCulley et al11 reported that among patients with meibomian gland dysfunction, the amount of tear is often decreased. In addition, Zengin et al12 reported that the tear break up time decreases in these patients because the tear film has become destabilized, thus increasing tear evaporation.
In this study, in order to objectively diagnose and evaluate dry eye syndrome from meibomian gland dysfunction, the tear break up time test and Schirmer test were employed. These tests are the most commonly used exams in the diagnosis of dry eye syndrome, and their precision, reproducibility, and reliability have been reported in various studies.13-20
Specifically, Lemp and Hamil18 reported that when the degree of dry eye is severe, the tear break up time test is more reliable and reproducible, and Ki et al20 has reported that the reproducibility of measuring the BUT in dry eyes was 95%. Lucca et al21 reported that Schirmer test has 25% sensitivity and 90% specificity.
The basic Schirmer test is conducted after topical proparacaine is instilled, although the test can also be performed without any topical anesthetics. The former measures basic tear secretion while the latter combines basic as well as reflex secretion.
However, the accuracy and specificity of these tests remain controversial in diagnosing dry eye syndrome.21-24 However, because these tests are still commonly used in today's clinics, a comparison of these test results was considered clinically significant.
The treatment of meibomian gland dysfunction consists of treatment for dry eye, improvement in lid hygiene and antibiotic therapy. Lid hygiene can be improved by applying compression with warm, wet towels, thus softening the secretions which cover the lid, and by lid massage in which the patient squeezes the meibomian glands, thus expressing the contents. The patient is also asked to scrub his or her lids with cotton tips immersed with baby shampoo or lid cleanser. The patient is asked to repeat these three measures at least twice a day.
When the patient has complications such as keratitis or other very severe symptoms, antibiotic therapy consisting of erythromycin, bacitracin, or polysporin ointments can be prescribed once or twice a day, and the patient may even be given systemic tetracycline. 200 mg of doxycycline, a long acting analogue of tetracycline can be given to patients twice a day.25 However, doxycycline has numerous side effects such as gastrointestinal problems (dyspepsia, nausea, vomiting, diarrhea), dermatologic problems (macules, papules), hypersensitivity reactions (allergy, urticaria, fever), glossitis or stomatitis due to vitamin deficiency, increased tendency to bleed, liver failure, esophagitis, etc.
When low doses of doxycycline are employed to prevent or treat periodontitis in field of dentistry, the incidence of these gastrointestinal and dermatologic side effects is reported to be dramatically lower compared to a high dose group.26-28 In this study, the authors also found results consistent with these findings; the incidence of side effects was lower in the low dose group (8 patients, 17.39%) than the high dose group (18 patients, 39.13%).
Doxycycline is a metal ion chelator and a broad spectrum antibiotic that prevents access of acyl t-RNA to the acceptor site on the mRNA-30s ribosomal subunit complex.
In addition to these established functions, other properties that have recently been ascribed to doxycycline include differential inhibition of the activity of members of the matrix metalloproteinase (MMP) family, inhibition of MMP synthesis, inhibition of interleukin-1 synthesis, inhibition of activated B cell function, inhibition of nitric oxide (NO) synthesis by lipopolysaccharide activated macrophages, and inhibition of collagen synthesis by cultured chondrocytes.2
Doxycycline inhibit an enzyme called collagenase. Collagenase is part of a family of proteinases called matrix metalloproteinases (MMPs). MMPs are involved in a number of physiological events, including tissue remodeling, and pathological processes such as periodontal disease, arthritis, osteoporosis and blepharitis.
MMPs are normally under tight regulation. Disruption of this regulation leads to pathologic breakdown of the connective tissues. Collagen is the major component of connective tissues in the body (bone and soft tissue such as gingiva, eyes, and skin). Collagenase is synthesized and released primarily from neutrophils in response to bacterial infection and is responsible for breaking down collagen. There are several types of human MMPs. Some important MMPs involved in diseases include the collagenases MMP-1 (produced by fibroblasts and responsible for the normal turnover of tissues), MMP-8 (produced by neutrophils), and MMP-13 (produced by bone cells).
In the inflammatory process, macrophages secrete cytokines (such as interleukin-1, tumor necrosis factor-alpha and prostaglandins) that stimulate the production of MMPs from neutrophils, fibroblasts, osteoclasts, and osteoblasts.
Doxycyclines inhibits both the inflammatory process and connective tissue breakdown through multiple mechanisms. These mechanisms include direct inhibition of active MMPs and inhibition of the oxidative activation of pro-MMPs, reduction in the secretion of cytokines and prostaglandin synthase, and an increase in pro-anabolic collagen production.
Sub-antimicrobial doses of doxycycline hyclate (SDD) 20 mg twice daily significantly reduce collagenase activity, while maintaining maximum plasma drug concentrations below the antimicrobial threshold of 1 mcg/mL, and are not sufficient to inhibit MMP-1 activity, and accordingly do not have undesirable effects on normal tissue turnover in other body systems. The mechanism of action is to inhibit hostderived MMP enzymes (collagenases and other proteinases) that are associated with collagen destruction. SDD inhibits already-active MMPs and blocks their synthesis and release. It also inhibits the production and/or activation of the pro-inflammatory cytokine IL-1 and TNF-alpha, both of which stimulate the production of collagenase.25-28
Recently, in the field of dentistry, symptoms of periodontitis have reportedly been reduced after the usage of tetracycline or doxycycline, and use of a lower dosage of doxycycline hyclate (20 mg) proved to be as effective as the conventional 100 mg dosage. Furthermore, the low dosage of doxycycline also proved to be effective in dermatologic disorders (i.e., rosacea), blepharitis, postmenopausal osteopenia, perioral dermatitis, and arthritis.26-27 In this study, the authors attempted to show that low dose doxycycline can be effective in the treatment of meibomian gland dysfunction with a reduction in the incidence of side effects.
However, the limitations of this study include the short follow up time of 1 month, and questionable patient compliance (continual ingestion of doxycycline). When a high protein or high lipid diet is ingested with doxycycline, drug absorption can be reduced. Patients were accordingly educated to take the medication on an empty stomach in order to facilitate absorption. However, bias due to patient compliance wasn't considered. It is possible that patient compliance increased in the low dose group because of fewer incidences of side effects. In addition, dysfunction of meibomian glands wasn't examined directly but rather through indirect measures such as tear break up time and the Schirmer test.
In this study, the authors witnessed improvements in dry eye symptoms after ingestion of low dose doxycycline hyclate (20 mg twice a day), which had no antimicrobial effect among patients with chronic meibomian dysfunction who were refractory to conventional therapy, including warm compression, lid massage, and topical antibiotic therapy. We also can expect the patient compliance to rise because of fewer incidence of side effects.
Further studies will be necessary to assess the efficacy of low dose doxycycline hyclate therapy.






 XML Download
XML Download