

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Persistent corneal epithelial defect is caused by keratoconjunctivitis sicca, exposure keratitis, neurotrophic keratitis, limbal stem cell failure, and ulcer after infection.1 Particularly, the deficiency of the essential tear components, such as epidermal growth factor (EGF) and vitamin A, and of neurotrophic factors, such as acetylcholine and substance P, may exacerbate the lesions.2 Presently, general treatments for persistent corneal epithelial defect are the application of therapeutic contact lenses, medical treatment, such as the instillation of artificial tears, and surgical treatments including cyanoacrylate glue, conjunctival flap, tarsorrhaphy, and amniotic membrane transplantation.
Autologous serum contains the substances required for the maintenance of corneal and conjunctival epithelium, such as EGF, vitamin A, transforming growth factor-β (TGF-β), fibronectin, substance P, nerve growth factor (NGF), and other cytokines, and thus it is able to facilitate the recovery of the injured ocular surface.1,3 Therefore, autologous serum eyedrops may be applied clinically for the treatment of persistent epithelial defect including neurotrophic keratopathy, and it has been applied effectively for the treatment of severe dry eye including Sjogren's syndrome, superior limbic keratoconjunctivitis, and recurrent corneal erosion.1,3-8 However, in regard to autologous serum, its shortcomings are that it requires repeated blood collection from patients, and that it is sometimes accompanied by discomfort or by treatment refusal by some patients. Also, it is difficult to obtain blood from patients with poor general condition or blood dyscrasia.
Umbilical cord serum also contains EGF, vitamin A, acidic and basic fibroblast growth factor (FGF), NGF, and other growth factors as well as tear components. Fetal bovine serum is widely used in the laboratory to promote cell growth in culture and is known to promote the migration of corneal cells in vitro and to modulate the clonal growth and differentiation of cultured limbal and corneal epithelium.5,9,10 Therefore, considering these above mentioned shortcomings of autologous serum, umbilical cord serum in place of autologous serum shows greater promise in various ocular surface diseases including persistent corneal epithelial defect.
Under the assumption that umbilical cord serum contains various growth factors and tear components, we investigated the efficacy of umbilical cord serum eyedrops on persistent epithelial defect of the cornea.
Materials and Methods
Persistent corneal epithelial defect was defined as a corneal defect with a minimum diameter of 2 mm along the greatest axis persisting for at least 2 weeks without improvement in spite of conventional treatments such as tear supplements and bandage contact lenses.10 Patients with progressive corneal epithelial defect caused by immunological causality such as rheumatoid arthritis and Mooren's corneal ulcer, suspicious impending perforation, acute ocular infection or inflammation, drug toxicity, and abnormalities in the eyelid or eyelashes were excluded from the study population, as were pregnant or lactating women. Fourteen eyes of 14 patients with persistent epithelial defect were recruited. Informed consent was obtained from each subject enrolled. Institutional review board / ethic committee approval was obtained from the Chonnam National University Medical School Institutional Review Board, and the study protocol followed the guidelines of the Declaration of Helsinki.
Umbilical cord blood was obtained from mothers with vaginal or caesarean section delivery after obtaining informed consent. Laboratory data for hepatitis B and C virus and human immunodeficiency virus (HIV) were examined twice at 8 and 38 gestational weeks. After fetal delivery, 100 ml of the umbilical cord blood was collected by inserting a syringe attached with an 18 gauge needle to the umbilical vein. Umbilical cord blood was clotted for 30 minutes at room temperature. After centrifugation at 1500 rpm for 5 minutes, the serum was isolated carefully and then diluted to 20% concentration with unpreserved normal saline solution. To prevent the degradation of vitamin A by ultraviolet light, it was aliquoted into sterile 5ml bottles wrapped with aluminum foil.
Patients were instructed to keep an opened bottle in a refrigerator (4℃) and to store unopened eyedrop preparation bottles in a freezer (-20℃). The maximum storage time was 3 months. Patients were also instructed to instill umbilical cord serum eyedrops 6 times a day in addition to the prior artificial tears. To assess the safety of the umbilical cord serum eyedrops, bacterial and fungal cultures were performed on samples (n=4) of used and stored sera.
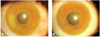
To evaluate the patients with persistent corneal epithelial defect at one week intervals, pictures of the cornea were taken after the administration of fluorescein dye at a magnification of ×10 using a slit-lamp microscope attached to a camera (F-801s, Nikon, Japan). After measuring the longest linear diameter and the longest vertical diameter of the epithelial defect area, the area of the equivalent rectangle was calculated by multiplying the two measured dimensions.11 Treatment was considered effective for epithelial defect healing within 2 weeks, partially effective for healing within 2 to 4 weeks, and ineffective for healing requiring either more than 1 month or additional measures.5
For statistical analysis, Mann-Whitney U test was performed by using SPSS.
Results
Among 14 patients (14 eyes) with persistent corneal epithelial defect, 12 patients were male and 2 were female. The mean age was 52.8 years (31-73 years), and the mean duration of follow-up was 3.8 months (2-6 months).
Persistent epithelial defect was the result of neurotrophic keratopathy in 8 eyes, chemical burn in 2, graft-versus-host disease in 1, limbal stem cell deficiency in 1, and infectious bacterial ulcer in 1. In 1 eye, persistent epithelial defect was developed after corneal transplantation. Among the 8 eyes with neurotrophic keratopathy, 3 had herpetic neurotrophic keratopathy, 4 had diabetic neurotrophic keratopathy, and in 1, persistent epithelial defect was developed after chemotherapy for nasopharyngeal carcinoma. Regarding the previously attempted conventional treatments, artificial tears had been used in all 14 eyes (100.0%), therapeutic contact lens in 3 (21.4%), and combined amniotic membrane transplan tation and therapeutic contact lens. The mean duration of epithelial defect prior to treatment was 7.2±6.3 weeks (2 - 20 weeks) and the mean area of epithelial defect was 7.86±7.32 mm2 (1.32-22.40 mm2) (Table 1).
Among the 14 eyes, the epithelial defect healed within 2 weeks (effective) in 6 (42.9%), between 2 and 4 weeks (partially effective) in 6 (42.9%), and did not heal within 4 weeks (ineffective) in 2 (14.2%). However, in the latter two cases, one of which had chemical burn and the other herpetic neurotrophic keratopathy, both eyes did eventually heal within 8 weeks. The mean healing time in the 6 eyes which showed effective outcome was 1.83±0.41 weeks and that in the 12 (85.7%) which showed effective or partially effective outcome was 2.75±1.06 weeks (Fig. 1).
The duration of epithelial defect prior to treatment was 3.5±1.2 weeks (2-5 weeks) in the 6 eyes which showed effective outcome and 10.0±7.2 weeks (2-20 weeks) in the 8 eyes which showed partially effective or ineffective outcome. The difference between the two groups was statistically significant (P=0.020). The area of epithelial defect prior to the treatment was 3.09±2.69 mm2 (1.32-8.40 mm2) in the 6 eyes which showed effective outcome and 11.45±7.76 mm2 (2.10-22.40 mm2) in the 8 eyes which showed partially effective or ineffective outcome. The difference was not statistically significant (P=0.063) (Table 2).
Bacterial and fungal cultures showed no growth in either used or stored sera. No significant complications associated with the use of umbilical cord serum were observed.
Discussion
Tears play an important role in the maintenance of healthy ocular surface, and the important tear components for the proliferation, differentiation and maturation of the normal ocular surface epithelium are EGF, vitamin A, TGF-β, acidic and basic FGF (Ed-already defined in the introduction), fibronectin, α2 macroglo ulin, and substance P.1,12-15 EGF suppresses apoptosis and may accelerate the proliferation of corneal epithelial cells, vitamin A can suppress the progression to squamous metaplasia in keratoconjunctivitis sicca, while TGF-β controls the proliferation of corneal epithelial cells and maintains cells in undifferentiated conditions.6,16,17 Fibronectin also accelerates the epithelization of the cornea, neurotropic factors such as substance P accelerate the migration of corneal epithelial cells in normal wound healing, and α2 macroglobulin plays a role in the suppression of collagenase in the cornea.1,3
Persistent corneal epithelial defect is caused by kerato-conjunctivitis sicca, neurotrophic keratitis, exposure keratitis, and limbal stem cell failure, and in addition to the general treatment methods described above, the administration of sodium hyaluronate, fibronectin, EGF, vitamin A, substance P, NGF, insulin-like growth factor-1 (IGF-1), and autologous serum has been reported to be effective.3,5,18-24
Theoretically, since serum contains EGF, vitamin A, TGF-β, fibronectin, substance P, NGF, and other growth factors, as well as essential tear components, it could supply the basic substances required for the regeneration of epithelial cells in the ocular surface. Therefore, it may be used for the treatment of ocular surface diseases including persistent corneal epithelial defect.8 It has been reported that the concentration of EGF is higher in tears, while that of vitamin A and TGF-β is higher in the serum.25 Similarly, a higher concentration of substance P, NGF, and IGF-1 has been detected in the serum.3
In 1984, Fox et al4 reported for the first time that in the treatment of Sjorgren syndrome, the application of autologous serum was effective. Subsequently, several studies have reported the treatment efficacy, stability, and safety of autologous serum in the external ocular field.1,6,15,26,27 Particularly, in regard to the effect of autologous serum on persistent corneal epithelial defect, Tsubota et al5 reported in 1999 that following application of 20% autologous serum to 16 patients, healing was observed within 2 weeks in 43.8%, and within one month in 62.5%, and that increased duration of persistent epithelial cell defect prior to treatment was associated with a slower healing rate. Poon et al1 have reported that in 15 patients who underwent application of 50% or 100% autologous serum, healing was achieved in an average of 29 days in 60.0%, and that after serum use was discontinued, epithelial defect recurred in 55.6%. Matsumoto et al3 have reported that in 11 neurotrophic keratitis patients (14 eyes), the epithelial disorders healed completely in all eyes within an average of 17.1 days after the use of autologous serum. In Korea, the treatment effect of autologous serum on alkali burn in the rabbit cornea has been reported. Among these studies, Yoo et al28 have reported that no significant difference was detected in the quantitative analysis results of the healing of the epithelium in comparison with the control group. Nevertheless, their histopathological results confirmed that the basement membrane of the epithelium was maintained better in the cases that used autologous serum.28,29
Regarding the stability of autologous serum used in persistent corneal epithelial defect, it has been reported that the concentration of its components, such as EGF, vitamin A, and TGF-β, is maintained well for up to 1 month in a refrigerator at 4℃ and up to 3 months in a freezer at -20℃.5,6 In addition, autologous serum is safe provided that the eyedrops are prepared and stored according to a strict protocol. Until now, no serious complications with the use of serum eyedrops have yet been reported.30 Regarding the safety of autologous serum, it contains antibacterial agents such as immunoglobulin G, lysozyme, and complement, enabling it to suppress the growth and proliferation of pathogens. Autologous serum could avoid the toxicity encountered with using preservatives, and experimentally it has been reported to be less toxic than unpreserved hydroxypropyl methylcellulose.1,15,26
However, the shortcomings are that autologous serum treatment may induce patient discomfort and treatment rejection due to the need to draw blood at regular intervals. Furthermore, the patient waiting time may become prolonged during the preparation of serum eyedrops, and it is difficult to obtain the blood in patients with poor general condition or blood dyscrasia. Considering these points, umbilical serum treatment has several clinical advantages over autologous serum treatment. First, by obtaining a large quantity of umbilical blood from mothers, the serum can be supplied to many patients. Second, umbilical cord serum eyedrops can be prepared in advance, thereby shortening the waiting period for the patients. Finally, even when taking the blood from the patients themselves is difficult due to poor general condition, serum treatment remains feasible. Recently, Vaipayee et al10 have reported that since umbilical serum contains a higher concentration of EGF, vitamin A, acidic and basic FGF, fibronectin, NGF, substance P, and antiproteases like α2 macroglobulin, it may be more useful for treatment of the ocular surface than autologous serum. They also reported that the recovery was faster using umbilical serum, compared to autologous serum, for persistent corneal epithelial defect refractory to medical treatment.
Given this combination of advantages for the use of umbilical cord serum, and under the assumption that umbilical cord serum also contains the tear components, we examined the effect of 20% umbilical serum eyedrops in the treatment of persistent corneal epithelial patients. The results showed that a partially or fully effective treatment result was achieved in 85.7% of patients. In addition, no significant complications related to the use of umbilical cord serum eyedrops were detected, and negative findings were obtained in bacterial and fungal cultures of the eyedrops. The shortcoming of our study is the absence of any comparison of umbilical serum with autologous serum or other treatments, which may require confirmation in a future study. Although we used 20% umbilical serum in this study, there is no agreement on the best dilution concentration of serum for use in ocular surface disease. Therefore, additional studies on the proper concentration of serum may be required.
In conclusion, the application of umbilical serum eyedrops for the treatment of patients with persistent epithelial defect was proven to be effective and safe.


 XML Download
XML Download