

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Since the first report by Foster et al,1 progressive outer retinal necrosis (PORN) has been established as a clinically distinct form of viral retinitis in AIDS patients. PORN can be differentiated from other forms of viral retinitis by its characteristic deep retinal lesions at onset, the absence of vascular inflammation, minimal ocular inflammation, frequent macular involvement, rapid progression course, and frequent perivenular clearing.2 Its diagnostic criteria were reported by Engstrom et al2 and its etiology is believed to be the varicella zoster virus (VZV).2-4 Treatment with acyclovir alone has been shown to be ineffective, but combination antiviral treatment with ganciclovir and foscarnet have been reported as more successful.2-5
Highly active antiretroviral therapy (HAART) involves a combination of protease inhibitors and reverse transcriptase inhibitors. HAART has been suggested to prevent PORN by lowering the viral load and by maintaining high CD4+ T-cell counts.6 We report a case of PORN in an AIDS patient who showed an atypical course with concurrent HAART.
CASE REPORT
A 22-year-old male patient presented with decreased visual acuity in his left eye of 10 days duration. He had had hemophilia type B and had experienced multiple intracranial hemorrhages. During a period of chronic transfusion, he had been infected with the human immunodeficiency virus (HIV). Six months before he had begun to experience vision deterioration, he had been diagnosed with zoster on his right flank area when his CD4+ T-cell count was 20 cells/µL. He had been administered intravenous acyclovir for two weeks, and HAART (zidovudine, stavudine, lamivudine, indinavir or nelfinavir) was started thereafter. A screening examination of the left eye at that time had found a clear anterior segment and a normal fundus with a visual acuity of 20/40 and a history of strabismic amblyopia. The ocular examination performed after the vision deterioration of his left eye (six months after zoster infection and HAART) revealed a visual acuity of hand motion, a totally opaque white cataract, and a trace of anterior chamber cells. In the right eye, visual acuity was 20/20 and the anterior segment and fundus appeared to be normal. Ultrasonography of the left eye showed a flat retina and a minimal vitreous opacity. At the time of the ocular examination, his CD4+ T-cell count was 210 cells/µL, and HAART was maintained to increase his CD4+T-cell count number. The patient underwent routine cataract surgery involving phacoemulsification with intraocular lens implantation.
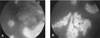
One-week postoperatively, his visual acuity was finger count with little improvement. A retinal lesion was also noted and he was referred to the retinal service. A fundus examination of the left eye showed yellowish, necrotic peripheral retinal lesions sparing the retinal vessels and opaque deep retinal lesions around the posterior pole (Fig. 1A, 1B). In the mid-periphery, some retinal lesions had a quiescent mud-cracked appearance indicating that the retinitis had been in the chronic stage and that the inflammation had started to regress without antiviral treatment. Vitreous haziness was present to a mild degree and a trace number of vitreous cells were observed. Fluorescein angiography revealed profuse leakage from the capillaries involved by the retinal lesions (Fig. 2A). Serologic testing showed positive IgG antibodies for VZV and cytomegalovirus (CMV). However, the IgM antibody tests for VZV, CMV and herpes simplex virus (HSV) were negative. The CD4+ T-cell count during this period was 380 cells/µL. Based on his clinical features, the patient was diagnosed to have PORN, even though the viral cultures and PCR analysis of the aqueous humor for VZV, HSV, CMV and EBV were negative. Intravenous acyclovir, 13 mg/kg/day, and ganciclovir, 10 mg/kg/day were administered for 2 weeks, after which he was given oral acyclovir for two months as a maintenance therapy. Fluorescein angiography 10 days after the antiviral treatment showed a reduction in the leakage from the active lesion around the posterior pole (Fig. 2B). His left visual acuity had improved to 20/200 and was maintained eight months later, when the retina still appeared to be quiescent (Fig. 3).
DISCUSSION
Necrotizing herpetic retinopathy is a continuous spectrum of diseases induced by herpes viruses. The clinical expression depends on the immune state of the host ranging from acute retinal necrosis at one extreme in patients with normal immunity to PORN in severely immunocompromised patients at the other.7 The two largest clinical studies2,4 on PORN found that the clinical course was rapidly progressive and that approximately half of the diseased patients treated with combinations of antiviral regimens had a final visual acuity of no light perception. The most common presenting symptom was a unilateral decrease in visual acuity, and an average CD4+ T-cell count, during the disease course, of 21 cells/µL (range: 0-168 cells/µL).
Compared to acute retinal necrosis and CMV retinitis, the diagnosis of PORN in this case was supported by the following findings. A retinal lesion involving the macula in an immunocompromised patient with minimal intraocular inflammation; no vasculitis; no peripheral circumferential spreading pattern; characteristic appearance of deep retinal lesion and cracked-mud appearance; previous history of zoster infection; no evidence of any other systemic CMV infection; no retinal detachment; and no involvement of the contralateral eye.
The present case was unusual in that cataract was the first manifestation of PORN. The low grade of intraocular inflammation might have played a role in the pathogenesis of cataracts in this young patient. This possibility suggests that PORN should be included in the differential diagnosis of unilateral cataract in AIDS patients, particularly in those with a previous history of zoster. Furthermore, in such cases, early cataract intervention and prompt retinal evaluation may enable the earlier diagnosis and treatment of viral retinitis and thereby improve the visual prognosis.
In this study, the CD4+T-cell counts at the time of cataract presentation and PORN diagnosis (210 cells/µL and 380 cells/µL, respectively) were relatively higher than those of previously reported cases, presumably because of the HAART and the delayed diagnosis.2-4 Considering the presence of a low CD4+ T-cell count 6 months before presentation and the complicated hypermature cataract, the retinitis may have begun several months before the visit to the retina clinic. Moreover, the amblyopic vision in the involved eye may have contributed to the delayed diagnosis.
At the time of PORN diagnosis, the peripheral retinal lesions had already started to spontaneously regress, which may have been due to the increased CD4+ T-cell count attributed to the concurrent HAART. Patients receiving HAART following treatment for CMV retinitis have been reported to have better control and to resist CMV retinitis reactivation. 8,9 Referring to the reports on the suppression of AIDS-related CMV retinitis with concurrent HAART and the role of the immune status on the development of PORN,6 it may be speculated that the retinal lesions in this case regressed under the influence of improved host immunity after HAART.
In addition, the previous intravenous acyclovir therapy of 2 weeks duration against the zoster might also have altered the course of PORN, but its role is likely to have been minimal in view of the previously reported poor response of PORN to intravenous acyclovir alone. After cataract surgery, the regression of retinitis accelerated with a combination intravenous antiviral therapy of acyclovir and ganciclovir - the deep retinal lesion at the macula became inactive, the vitreous haziness cleared with improvement of visual acuity, and no further progression was evident. We firmly believe that HAART may induce PORN regression and potentiate the effects of antiviral treatment by improving host immunity.
This case demonstrates a non-typical clinical course of PORN during HAART, and suggests that HAART might change the clinical course of PORN. Moreover, the case demonstrates that a cataract can be the first manifestation of PORN in AIDS patients.


 XML Download
XML Download