

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hydrogels that are used in retinal reattachment surgery are hydrophilic materials formed by a 3-dimensional polymer network. Miragel (MIRA, Waltham, Mass, USA) is a soft, elastic and smooth material, and it is one of the most widely used hydrogels. It consists of co-poly (methylacrylate-2-hydroxyethy acrylate) cross-linked with ethylene diacrylate and 15% water. It was first introduced in the late 1970s and initially, it was thought to offer several advantages over the silicone materials that were then used.1,2 It was soft, elastic and considered less likely erode through the conjunctiva. The material did not contain any dead space and it could absorb and slowly release antibiotics; this minimized the risk of infection. However, the explant was withdrawn from the market in the 1990s because of the late complications occurring 7 to 11 years after the surgery.3-6 These problems include erosion into the globe, extrusion of the explants, formation of a periorbital mass and a progressive diplopia.
In this paper, we report a case of the development of a progressive diplopia associated with restricted extraocular movement and the presence of a pseudotumor 9 years following the use of a Miragel explant. This case presents the first Miragel-associated, long-term complications reported in Korea.
CASE REPORT
A 28-year-old female visited my clinic with a palpable mass lesion on the superonasal aspect of her right globe, and she had a progressive diplopia over past few years. She had received scleral encircling surgery with a 3.3*5.5 mm Miragel explant (MIRA, Waltham, Mass, USA) for the tractional retinal detachment associated with pars planitis 9 years previously.
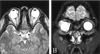
On examination, her visual acuity was 20/30 OD and 20/20 OS and the retina was well attached. The protruding mass lesion was palpable beneath the superonasal aspect of her right upper lid. The magnetic resonance imaging revealed an enlargement of the Miragel explant; this implied that the mass lesion was caused by the extrusion of the explant. (Fig.1 A,B) The extraocular movement of her right eye was severely restricted in all directions, especially upon adduction and elevation. (Fig. 2A) The progressive diplopia and limited extraocular movement were thought be caused by the mechanical restriction associated with Miragel explant and so, we decided to remove the explant.
At surgery, the Miragel material was found to be encapsulated with a thick fibrous capsule and it was extremely friable and tending to disintergrate when we tried to hold it with forceps. (Fig. 3) A tedious and complete removal of the encircling material was done, along with the dissection and removal of the fibrous capsule on the explant.
The removed Miragel material demonstrated that the buckle had swollen up to 2.06 times its original size. Scanning electron microscopy revealed a deteriorated material with micropores; the explant was distorted in shape and irregular in size.(Fig. 4 A,B)
At 1 month postoperatively, the retina remained well attached and the patient's visual acuity was 20/25 OD. The follow up Hess screen test documented a much-improved extraocular movement (Fig. 2B), and also, a cosmetic improvement was achieved.
DISCUSSION
Scleral buckling material evolves from the autologous fascia lata to attach to the non-absorbable synthetic agents, such as polyethylene, silicone, and hydrogels. The hydrogels, including Miragel, were initially thought to be ideal substitutes for the other synthetic material because their structural and chemical characteristics. The explant was as effective in buckling as solid silicone rubber and silicone sponge. Altering the state of hydration could vary the degree of swelling and this increased the buckling height in the immediate postoperative period. Hydrogels were soft, elastic and considered less likely to erode through the conjunctiva. In addition, the material was assumed to be less prone to infection because it did not contain any dead space and it could absorb and slowly release water-absorbable antibiotics.1,2 However, the long-term complications of the Miragel material began to emerge 7 to 11 years following the surgery.3-6 The complications included erosion into the globe, extrusion of the explants and a progressive diplopia. The material has shown to be structurally unstable and this leads to excessive water absorption, swelling and disintergration.2-4 These complications necessitated the removal of buckling material. At surgery, the explants were seen as translucent and gel-like materials that were extremely friable, and this made it hard to remove them with a conventional method of using scissors and forceps. This resulted in a particle retention on removal of the scleral buckling element. According to the report by Marin, the alteration of the material is associated with a deterioration of its chemical composition.2 Micro-Fourier transform infrared spectroscopic analysis of recovered implants demonstrated the hydrolytic degradation of the implant; this led to a swelling greater than the original polymer.3 In our present case, the Miragel explant that was removed from the patient had swollen to 2.06 times its original volume. This resulted in a restriction in extraocular movement and the formation of a mass-like lesion.
Considering the historical data and the late complications observed in the present case, the hydrogel explants can no longer claim to provide advantages over other conventional scleral buckling materials. The hydrogel explants have been withdrawn from the market since the 1990s. As these complications usually occur 7 to 11 years following the surgery, it is highly recommended for the ophthalmologists who have used hydrogel materials in retinal surgery to be aware of these problems and do regular follow ups for the patients with hydrogel explants.



 XML Download
XML Download