

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Nonalcoholic fatty liver disease (NAFLD) includes simple fatty liver, nonalcoholic steatohepatitis, cirrhosis, and hepatocellular carcinoma (1). In western countries, the prevalence of NAFLD has increased to as high as 30%, and this disease has become the most common chronic liver disease (2). A study on NAFLD diagnosed with sonography reported that the prevalence of this disease in Korea is estimated to be as high as 16%–33% (3,4).
NAFLD is known to be related to obesity, type 2 diabetes, and metabolic syndrome (1,5). Furthermore, there have been several data showing that insulin resistance (IR) and visceral adipose tissue are associated with the pathogenesis NAFLD (6,7).
In recent years, vitamin D has commonly been associated with NAFLD. A biopsy study of NAFLD showed that subjects with NAFLD had lower levels of serum 25-hydroxyvitamin D3 [25(OH)D3] than healthy controls, and that low 25(OH)D3 levels were related to the severity of the hepatic histology of NAFLD subjects (8). Moreover, a recent meta-analysis reported that vitamin D deficiencies were 26% more common in NAFLD patients than in healthy persons (9).
Several studies indicated that vitamin D deficiency is related to metabolic syndrome, obesity, and IR (10,11). Because of the relationship of NAFLD with obesity and metabolic syndrome, the association of vitamin D deficiency with NAFLD could be linked to metabolic factors. However, several researches indicated the existence of an independent association between vitamin D levels and NAFLD. Recent cross-sectional studies of Korean population evidenced inverse associations between serum 25(OH)D3 levels and NAFLD after adjustment for metabolic syndrome or metabolic factors (12,13). Another study on a population-based cohort in Ansan, Korea (n = 1,081), suggested that a low vitamin D level is related to NAFLD after controlling for visceral fat in subjects with diabetes or IR (14). However, it is difficult to find a large population-based study in which both metabolic syndrome and visceral fat are considered.
Furthermore, according to the population-based study, NAFLD is more prevalent in men (3), and vitamin D deficiency is more frequently detected in women (15). However, there are only a few studies that have considered sex a factor that affects the association of vitamin D deficiency and NAFLD.
Therefore, the aim of the current study was to analyze the association of vitamin D deficiency and NAFLD after adjustment for metabolic syndrome and visceral fat. Additionally, this study aimed to investigate the independent association between vitamin D deficiency and NAFLD in a large population according to the sex of the subjects.
MATERIALS AND METHODS
Study population
In the present study, we investigated the participants in a health-screening program at the Healthcare System Gangnam Center and the Health Promotion/Disease Prevention Center of Seoul National University Hospital, Seoul, Korea.
The study population consisted of 12,835 eligible subjects who had undergone blood tests for serum 25(OH)D3 levels, abdominal sonography, and computed tomography (CT) for visceral fat mass. Furthermore, the exact data for alcohol consumption from January 1, 2008 to July 31, 2015 were recorded. The exclusion criteria were as follows: subjects who tested positive in serological tests for hepatitis B or C virus (n = 680); those who drank excessive alcohol, as defined by an average alcohol intake of 210 g/week in men (n = 1,617) or 140 g/week in women (n = 214), according to the American Association for Study of Liver Diseases guideline (5); those with evidence of a disease that could have an influence on the liver (n = 1,582), such as liver cirrhosis, cardiovascular disorder (i.e., stroke, angina, and myocardial infarction), cancer, and chronic kidney diseases; those who were taking medications that can affect the 25(OH)D3 level, such as medication for osteoporosis and vitamin supplementation (multivitamin and/or vitamin D) (n = 926); those who underwent multiple health check-ups during the study period (n = 216; only the first-visit data were analyzed); and those with any missing essential information (n = 86), such as systolic blood pressure (SBP), diastolic blood pressure (DBP), triglyceride, high-density lipoprotein (HDL), fasting glucose, body mass index (BMI), and waist circumference (WC). After the application of these exclusion criteria, the final study population comprised 7,514 subjects (5,278 men and 2,236 women) (Fig. 1).

Diagnosis of NAFLD
NAFLD was diagnosed by using abdominal ultrasonography (Acuson, Sequoia 512; Siemens, Mountain View, CA, USA) carried out by well-trained radiologists. A diagnosis of fatty liver was made if hepatorenal contrast and liver brightness were observed (16).
Anthropometric and laboratory measurements
The height and weight of the subjects were measured while they were wearing a light gown. The WC was measured at the midpoint between the lower costal margin and the iliac crest. The BMI was calculated as the weight in kilograms (kg) divided by the square of the height in meters (kg/m2). After resting for >10 minutes, blood pressure was measured in a sitting position. Blood test was performed after an overnight fast, for measurements of serum glucose, total cholesterol, triglyceride, HDL, insulin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), gamma glutamyltransferase (GGT), calcium, phosphorus, hepatitis B surface antigen, antibody to hepatitis C virus, and 25(OH)D3 levels. Serum 25(OH)D3 levels were measured by radioimmunoassay (DiaSorin, Stillwater, MN, USA). IR was calculated as fasting glucose (mM/L) × fasting insulin (μU/mL)/22.5 by using the homeostasis model (homeostasis model assessment of insulin resistance [HOMA-IR]) (17).
Metabolic syndrome was defined according to the National Cholesterol Education Program Adult Treatment Panel III criteria and the Asia-Pacific criteria for WC (18). Metabolic syndrome was diagnosed if three or more of the following criteria were present: abdominal obesity (≥ 90 cm in men and ≥ 80 cm in women), elevated triglyceride level (≥ 150 mg/dL or treated for dyslipidemia), reduced HDL level (< 40 mg/dL in men, < 50 mg/dL in women, or treated for dyslipidemia), elevated blood pressure (SBP ≥ 130 mmHg, DBP ≥ 85 mmHg, or treated for hypertension), and elevated fasting blood glucose level (≥ 100 mg/dL or treated for hyperglycemia).
Measurement of the visceral fat using computed tomography (CT)
A 16-detector row CT imaging of the abdomen (Somatom Sensation 16; Siemens Medical Solutions, Forchheim, Germany) was used to evaluate the visceral fat. A 5-mm-thick slice at the umbilical level was obtained, and the visceral fat area was determined by using the Rapidia 2.8 software (INFINITT, Seoul, Korea), which detected the visceral fat area by setting the attenuation values within a range of −250 to −50 Hounsfield units.
Other clinical assessments
Medication for hypertension, dyslipidemia, diabetes was confirmed by using a self-reported questionnaire. We also surveyed lifestyle of the subjects, including alcohol consumption, smoking, and physical activity. For smoking status, the subjects were categorized as nonsmoker, ex-smoker, and current smoker. Physical activity was classified as inactive (< 600 metabolic equivalents [MET]-min/week), minimally active (≥ 600 and < 3,000 MET-min/week), and health-enhancing physical activity (≥ 3,000 MET-min/week) according to the International Physical Activity Questionnaire. This questionnaire is available online (www.ipaq.ki.se).
Statistical analysis
Statistical analyses were performed by using STATA, version 14.0 (Stata Corp., College Station, TX, USA). The general characteristics of the subjects who were grouped by NAFLD or sex were compared by using Student’s t-test for continuous data and Pearson’s χ2 test for categorical variables. We analyzed the associations between the 25(OH)D3 levels and each metabolic variable with regression models. Each model was adjusted for age, month of measurement, and physical activity because the vitamin D status is greatly affected by these factors. Three models were analyzed with multiple logistic regression to investigate the association between vitamin D deficiency and NAFLD after adjusting for variables such as age, month of measurement, smoking, physical activity, BMI, health check-up center, metabolic syndrome, and visceral fat. Vitamin D status was divided into three categories according to the 25(OH)D3 level: deficiency (< 20 ng/mL), insufficiency (20–30 ng/mL), and sufficiency (≥ 30 ng/mL). The statistical interactions were tested between sex and vitamin D in adjusted models with a multiplicative term.
As a sensitivity analysis, HOMA-IR was additionally added to the regression model in a subgroup of participants who had their HOMA-IR level measured. The women were divided into two groups (< 55 years old, ≥ 55 years old), and this enabled taking menopause into consideration in our regression model. Significance was defined as P < 0.05. All reported P values were two-tailed.
Ethics statement
The participants gave their informed consent for using their health check-up data. The present study was conducted according to the principles of the Declaration of Helsinki of the World Medical Association, and was accepted by the Institutional Review Board (IRB) at Seoul National University Hospital (IRB No. 1506-083-681).
RESULTS
General characteristics
NAFLD was found in 3,104 subjects (41.3%). The subjects with NAFLD were older and had more unfavorable metabolic profiles such as higher BMI, fasting glucose, cholesterol, and blood pressure. The NAFLD group had more visceral fat (150.0 cm2 vs. 94.6 cm2) and a higher prevalence of metabolic syndrome (36.1% vs. 9.5%). Furthermore, they were more inactive and more likely to be current smokers. The men showed more unfavorable metabolic profiles such as higher BMI, fasting glucose, blood pressure, visceral fat, and chronic current smoker. Women were less physically active than men, and a higher proportion of women than men had vitamin D deficiency (< 20 ng/mL; 57.6% vs. 44.2%). The characteristics of the study population are presented in Table 1.
Table 1
General characteristics
Continuous variables are expressed as mean ± standard deviation.
NAFLD = nonalcoholic fatty liver disease, BMI = body mass index, WC = waist circumference, HDL = high-density lipoprotein, SBP = systolic blood pressure, DBP = diastolic blood pressure, 25(OH)D3 = 25-hydroxyvitamin D3, HEPA = health-enhancing physical activity.
*Defined according to the National Cholesterol Education Program Adult Treatment Panel III criteria; †Classified according to the International Physical Activity Questionnaire; inactive, < 600 MET-min/week; minimal, 600–3,000 MET-min/week; HEPA, ≥ 3,000 MET-min/week.
![]()
Correlation between serum 25(OH)D3 levels and metabolic variables
After adjusting for age, month of measurement, and physical activity, the serum 25(OH)D3 levels were found to be negatively correlated with BMI and WC in women only, and positively correlated with HDL and negatively correlated with visceral fat in both sexes (Table 2).
Table 2
Adjusted regression coefficients between the 25(OH)D3 level and the metabolic variables
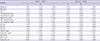
Each model was adjusted for age (continuous), month of measurement (January to December), and physical activity (inactive/minimal activity/health-enhancing physical activity).
25(OH)D3 = 25-hydroxyvitamin D3, SE = standard error, BMI = body mass index, WC = waist circumference, HDL = high-density lipoprotein, LDL = low-density lipoprotein, AST = aspartate aminotransferase, ALT = alanine aminotransferase, GGT = gamma glutamyltransferase, SBP = systolic blood pressure, DBP = diastolic blood pressure.
![]()
Vitamin D deficiency and NAFLD
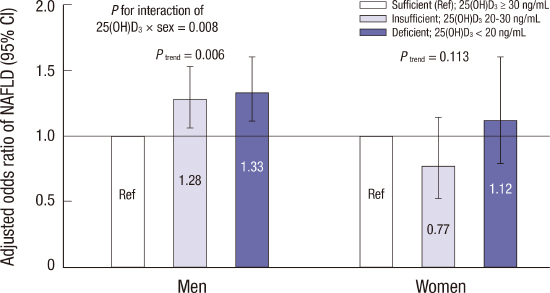
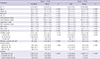
Table 3 shows that the odds ratio (OR) for NAFLD increased sequentially with a deteriorating vitamin D status in all models. Vitamin D insufficiency and deficiency were associated with NAFLD even after controlling for both metabolic syndrome and visceral fat (OR [95% CI] for NAFLD, 1.18 [1.00–1.39] in the insufficiency group and 1.29 [1.10–1.52] in the deficiency group compared with that in the sufficiency group; P
trend across vitamin D status = 0.002). The relationship between vitamin D deficiency and NAFLD was influenced by sex. We observed a significant interaction between sex and the vitamin D status (P < 0.05). In men, both vitamin D insufficiency and deficiency were associated with NAFLD (OR [95% CI] for NAFLD, 1.28 [1.06–1.53] in the insufficiency group and 1.33 [1.11–1.60] in the deficiency group compared with that in the sufficiency group; P
trend across vitamin D status = 0.006). However, vitamin D status was not significantly associated with NAFLD in women after adjustment for possible confounders (Fig. 2).
Table 3
The association between NAFLD and serum 25(OH)D3 levels

Model 1: adjusted for age (continuous), BMI (continuous), month of measurement (January to December), smoking (nonsmoker/ex-smoker/current smoker), physical activity (inactive/minimal activity/health-enhancing physical activity), and health check-up center (HPDPC/HCSGC); Model 2: model 1 + metabolic syndrome (present/absent); Model 3: model 2 + visceral fat (continuous).
NAFLD = nonalcoholic fatty liver disease, 25(OH)D3 = 25-hydroxyvitamin D3, OR = odds ratio, CI = confidence interval, BMI = body mass index, HPDPC = Health Promotion Disease Prevention Center, HCSGC = Healthcare System Gangnam Center.
![]()
 | Fig. 2aOR of NAFLD according to 25(OH)D3.
Logistic regression aOR (95% CI) of NAFLD according to the serum 25(OH)D3 level compared with the sufficient (≥ 30 ng/mL) reference group by sex (light gray bar: insufficient [20–30 ng/mL]; dark gray bar: deficient [< 20 ng/mL]). The regression model is adjusted for age (continuous), BMI (continuous), month of measurement (January to December), smoking (nonsmoker/ex-smoker/current smoker), physical activity (inactive/minimal activity/health-enhancing physical activity), health check-up center (HPDPC/HCSGC), metabolic syndrome (present/absent), and visceral fat (continuous).
aOR = adjusted odds ratio, NAFLD = nonalcoholic fatty liver disease, 25(OH)D3 = 25-hydroxyvitamin D3, CI = confidence interval, BMI = body mass index, HPDPC = Health Promotion Disease Prevention Center, HCSGC = Healthcare System Gangnam Center.
|
Sensitivity analysis
In the subgroup of participants who had their insulin level measured, HOMA-IR was added as a confounder in the regression model. Similarly, the relationship between vitamin D deficiency and NAFLD was observed in men only (Supplementary Table 1). Additionally, when we analyzed the two groups of women (younger or older than the menopausal age of 55 years), the association was not statistically significant in both groups; however, women ≥ 55 years old showed a trend of a positive correlation between vitamin D deficiency and NAFLD (Supplementary Table 2).
DISCUSSION
In the present study, we found that vitamin D deficiency could be an independent risk factor of NAFLD among Korean men. Although a few studies have suggested an inverse association between vitamin D and NAFLD after controlling for metabolic features, these studies either had a small population (8) or only considered metabolic syndrome (12) or visceral fat (14).
The present study revealed that the association between vitamin D deficiency and NAFLD persisted even after controlling for both metabolic syndrome and visceral fat in a large population. In a subgroup analysis with measurement of insulin level, this association persisted after further adjustment for HOMA-IR (Supplementary Table 1). This could mean that vitamin D deficiency is an independent risk factor of NAFLD in men.
To our knowledge, this is the first cross-sectional study that examined the effect of the sex on the relationship between vitamin D deficiency and NAFLD while considering a sufficiently large number of healthy subjects. Most previous studies did not analyze subjects according to sex. The few studies on the sex-related effect of vitamin D deficiency on NAFLD investigated either men alone (12) or postmenopausal women (19,20), and showed a positive association between vitamin D deficiency and NAFLD.
In our study, there was a significant interaction between sex and vitamin D status. Therefore, we analyzed the association between vitamin D and NAFLD by sex, and observed a sex disparity. The positive association between vitamin D deficiency and NAFLD in men was consistent with that reported in previous studies. Additionally, we adjusted for both metabolic syndrome and visceral fat to demonstrate the independent effect of vitamin D deficiency on NAFLD. However, the association between vitamin D and NAFLD in women was not significantly correlated.
The mechanisms underlying the sex-related association between vitamin D deficiency and NAFLD are still largely unknown. A possible mechanism for the sex differences could be that sex hormones may be mediators of NAFLD. Testosterone deficiency is a risk factor of NAFLD (21). A cross-sectional study including 2,299 men suggested that vitamin D deficiency could result in testosterone deficiency (22). Furthermore, a small randomized controlled trial proposed that vitamin D supplementation tends to increase the production of testosterone in men (23). There is another biological evidence showing that the vitamin D receptor (VDR) and enzymes related to vitamin D metabolism are widely expressed in the male reproductive system (24). Thus, vitamin D deficiency could result in NAFLD through the testosterone level.
Moreover, a sex-related VDR genetic variation could be another explanation. A VDR genetic variation is known to influence the association between vitamin D status and various diseases (25). In one case-control study on the Italian population, the association between VDR polymorphism and various lumbar spinal diseases was affected by sex (26). Although there has been no clinical study to show the sex effect on the relationship between VDR polymorphism and NAFLD, this could be a plausible explanation for our finding.
Unmeasured confounders may have also affected the null findings in women. NAFLD is greatly influenced by lifestyle, such as physical activity, diet, alcohol consumption, and smoking. For some of these factors, we could not perform measurements and adjustments.
This study has some limitations. First, NAFLD was diagnosed by means of sonography instead of biopsy, which is the gold standard. Therefore, we could not differentiate between simple steatosis and nonalcoholic steatohepatitis, which have different prognosis. However, it is not appropriate to conduct an invasive procedure in a large epidemiological study (27). Second, although, through the laboratory results or questionnaire, we excluded subjects with illnesses that could affect the liver function, rare liver diseases such as hemachromatosis or Wilson’s disease were not completely excluded. Third, although the menopausal status and information on hormone replacement therapy (HRT) are very important in the analyses of female subjects, many of them did not answer the questions on their menopausal status and HRT. Furthermore, when we analyzed women of age ≥ 55 years (most of them were presumed to be in menopause considering the average menopausal age of 50 years in Korean women), there was a marginal association between vitamin D deficiency and NAFLD (OR, 1.57; 95% CI, 0.96–2.58; Supplementary Table 2). This association should be confirmed with a well-designed prospective study. Fourth, owing to the cross-sectional design of this study, the causal relationship between vitamin D deficiency and NAFLD could not be defined. Also, the study subjects were participants in a health-screening program conducted by a university hospital, so this study’s findings have limited generalizability.
Despite these limitations, this is the first study to clarify the sex-related association of vitamin D deficiency and NAFLD after controlling for metabolic syndrome and visceral fat. Further prospective studies are needed to identify the causal relationship between vitamin D status and NAFLD, and well-designed randomized clinical trials could show whether vitamin D supplement can improve NAFLD.
 XML Download
XML Download