

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Inflammatory bowel disease (IBD) is a chronic, disabling disorder of the gastrointestinal tract. In the treatment of IBD, anti-tumor necrosis factor (anti-TNF) therapy significantly increased remission rates of IBD (123456). Anti-TNF therapies have similar efficacy and safety profiles, however, they differ in modes of administration and dosing schedules. Intravenous anti-TNFs, such as infliximab, are usually administered once every eight weeks by a trained healthcare professional (1256). For intravenous anti-TNFs, patients are required to attend clinics for administration and clinical observation, but the patient and/or family members have minimal responsibilities for the administration of the drug. Subcutaneous anti-TNFs, such as adalimumab, are usually administered once every two weeks (3456). For subcutaneous anti-TNFs, patients are not required to attend clinics at specific times, allowing flexibility in hospital visits. However, patients are required to be responsible for the administration of the drug. In this regard, physicians should discuss with their IBD patients about the anti-TNF options.
Shared decision-making should be considered when different treatment options may have different effects on the quality of life (QOL) of patients (78), as it can increase the effectiveness of treatment. In this regard, different modes and schedules of anti-TNF therapies may offer potential opportunities for shared decision-making to IBD patients (56). Peake et al. (9) reported that subcutaneous anti-TNFs were preferred over intravenous anti-TNFs in 36 Crohn's disease (CD) patients, but Allen et al. (10) reported the contrary preference in 78 IBD patients. Both studies were limited as they were inconsistent and based on a single center with a small number of patients (910). Recently, Kim et al. (11) reported the intravenous anti-TNF therapies were preferred over subcutaneous anti-TNFs in 189 CD patients. Patient and physician preferences for anti-TNFs may be different between Western and Asian countries, as many factors, such as lack of insurance reimbursement, high medical costs, concerns about tuberculosis infection and cultural background, may have different influence on the preference to anti-TNFs in Asian patients (910111213). Furthermore, Asian patients may have a different preference for being involved in shared decision-making, as it may be influenced by demographic factors, knowledge about IBD, their experience and relationship with healthcare professionals (14). Preference studies for anti-TNF therapies in Asian IBD patients should be warranted, considering the increasing prevalence of IBD in Asian countries (15161718).
The aim of this study was to evaluate the predictive factors for preferences to anti-TNF therapies and shared decision making for IBD patients in Korea.
MATERIALS AND METHODS
Patients
Between March and August in 2015, consecutive adult IBD patients, who received care for at least 6 months regardless of anti-TNF therapies, were invited to participate in this study at four university hospitals in Korea. IBD patients were interviewed by the study coordinators to collect information on the following variables: age, sex, tobacco/alcohol use, duration of IBD, marital status, employment status, education level, income level, medical treatment, and prior hospitalizations or surgeries. Demographic, clinical, and disease-related characteristics of IBD patients were compared according to their preferences of anti-TNF therapy. Patients were administered two questionnaires: ‘Patient preferences to anti-TNF therapy’ (Appendix 1 and 2) (910) and ‘Crohn's and ulcerative colitis questionnaire-8 (CUCQ-8)’ (Appendix 3 and 4) (19). Subjects were excluded if they were unable to comprehend the questionnaire or had an active psychiatric disorder.
Development of anti-TNF information sheet
A drug information sheet was provided to accompany the questionnaires mentioned above. The information sheet provides patients with reliable, accurate, and unbiased information to help them choose an appropriate anti-TNF therapy based on information provided by the Crohn's and Colitis Foundation of America (http://www.ccfa.org/resources/biologic-therapies.html). It was designed to enable patients to answer the study questionnaire as accurately and reliably as possible. The key topics in the drug information leaflet were: 1) indications of anti-TNFs for IBD; 2) summaries of the intravenous and subcutaneous anti-TNFs; and 3) key differences between the two anti-TNFs, especially in terms of their mode and schedule of administration. The quality of the information presented about the anti-TNFs was assessed using a validated tool that is used by health professionals and consumers to judge the quality of written health information (20). The information sheet and questionnaire were confirmed as reliable and valid by four health professionals who were not involved in this study. The questionnaire’s readability was tested using the Korean reading scale by researchers and patients not involved in the current study before starting the study. To establish whether patients would be able to understand the information sheet and questions, ten volunteers (hospital visitors and relatives of the patients) were randomly selected to check a pilot questionnaire and information sheet. In response to their comments, slight changes were made to the wording.
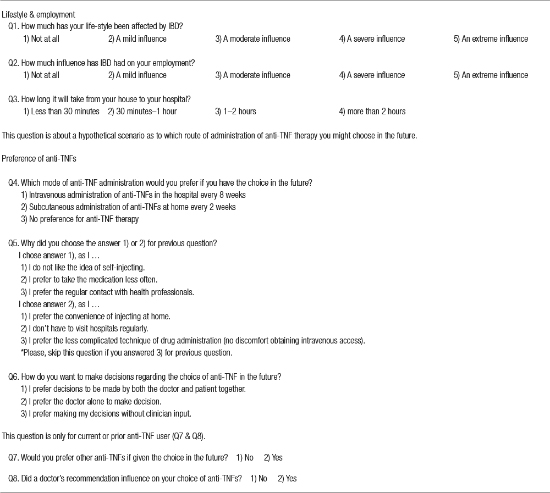
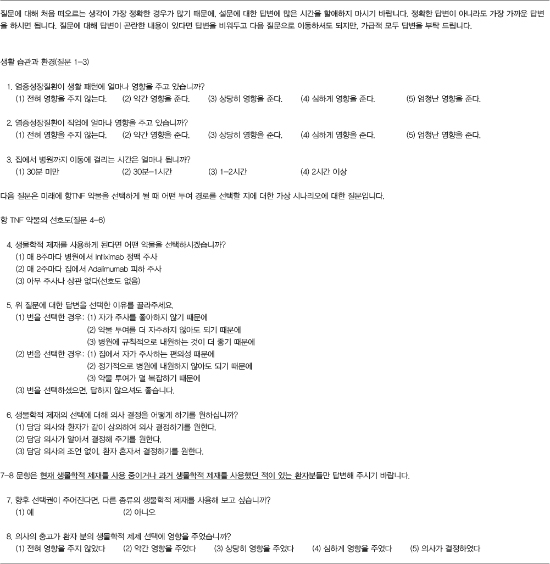
The questionnaires for preferences and QOL
The ‘Patient preferences for anti-TNF therapy’ questionnaire was designed to pose specific questions about the patient’s anti-TNF therapy, their preference for intravenous or subcutaneous anti-TNFs, and the reasons for these preferences. Patients were asked, in a hypothetical scenario, which anti-TNF administration they would prefer if given the choice in the future. It followed a predominantly closed-ended question format. The questionnaire asked patients about: 1) the influence of IBD on their lifestyle or employment; 2) preferences for anti-TNFs in terms of their mode and schedule of administration; and 3) shared decision-making. For the choice of anti-TNF therapy, the possible responses were: 1) Group A = preference for intravenous anti-TNFs at the hospital every 8 weeks; 2) Group B = preference for subcutaneous anti-TNFs at home every 2 weeks; or 3) Group C = no preference for any anti-TNF therapy. The patients were asked for the reasons for their choices. In addition, patients who had previously been administered any anti-TNFs were asked whether they would choose the same or an alternative route of administration in the future, if indicated.
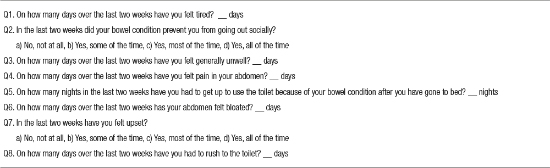
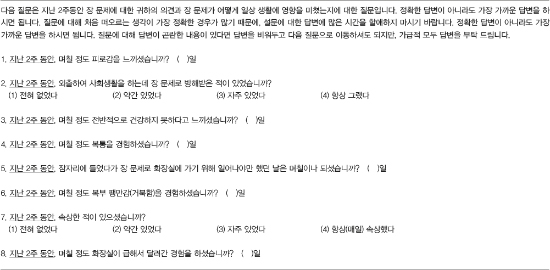
CUCQ-8 is a short, valid, reliable tool to measure QOL in all IBD patients (19). The CUCQ-8 questionnaire includes questions about a patient’s bowel problem and how these problems have affected their life over the last two weeks. The CUCQ-8 assesses subjective feelings of tiredness, being unwell, or upset, the presence of abdominal pain or bloating, the need to rush to the toilet or get up at night to use the toilet, and being prevented from going out socially due to a bowel condition. As validity, internal reliability, reproducibility, and responsiveness of CUCQ-8 were confirmed in IBD patients (19), disease-related QOL was measured with CUCQ-8 in this study.
Statistical analysis
Continuous variables are expressed as the mean ± standard deviation (SD) or median (range), and categorical variables are presented as the number of patients and percentage. Demographic and clinical variables in the three groups were compared using analysis of variance for continuous variables and a χ2 test for categorical variables. A multivariate logistic regression analysis was used to determine independent predictors of a preference to mode of anti-TNF administration. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated with adjustments for all of the relevant variables with significant univariate differences between groups (P < 0.05). Two-tailed P values < 0.05 were considered statistically significant. Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 18.0 for Windows (SPSS Inc., Chicago, IL, USA).
RESULTS
During the study period, 322 patients completed the questionnaires. IBD patients included 217 (67.4%) men and 105 (32.6%) women, and 148 (46.0%) CD and 174 (64.0%) ulcerative colitis. Their mean age was 39.7 ± 14.2 years, and mean duration of IBD was 5.9 ± 5.2 years.
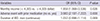
Table 1 shows the preferences to anti-TNF therapies in IBD patients. IBD patients preferred intravenous over subcutaneous anti-TNF therapies with a 2.4:1 ratio. The main reason given for a preference to intravenous anti-TNF was ‘I don’t like the idea of self-injecting’ (73.4%), and the main reason given for subcutaneous anti-TNF was ‘the convenience of injecting at home’ (73.1%). In this study, 58.4% of patients preferred shared decision-making. Approximately 2/3 (63.1%) of patients who had previously or currently receiving anti-TNFs reported that they wanted to change to the alternative anti-TNF regimens, if given the choice in the future.
Table 1
Preferences for anti-TNF therapy in patients with IBD

Group A means ‘preference for intravenous anti-TNF at the hospital every 8 weeks,’ Group B means ‘preference for subcutaneous anti-TNF at home every 2 weeks,’ and Group C means ‘no preference for any biological therapy.’
TNF = tumor necrosis factor, IBD = inflammatory bowel disease.
*Thirty-four cases in group A; and †15 cases in group B did not answer this survey item.
Demographic, clinical, and disease-related characteristics of IBD patients were compared according to the patients’ preference to anti-TNF therapies. Demographic and clinical characteristics of IBD patients was similar, however, higher income level was significantly different between three groups (Table 2). Disease-related characteristics of IBD patients were also compared between three groups (Table 3). Disease-related characteristics was also similar different between three groups, except for prior use of immunomodulators or anti-TNFs, adverse events with prior medication, hospitalizations for IBD, disease duration and much (≥ moderate) influence of IBD on their life style. In general, QOL, as measured by the CUCQ-8, was similar between three groups.
Table 2
Demographic and clinical characteristics of patients with IBD in relation to their preferences for anti-TNF therapy
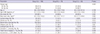
Group A means ‘preference for intravenous anti-TNF at the hospital every 8 weeks,’ Group B means ‘preference for subcutaneous anti-TNF at home every 2 weeks,’ and Group C means ‘no preference for any biological therapy.’
IBD = inflammatory bowel disease, TNF = tumor necrosis factor, CD = Crohn's disease, UC = ulcerative colitis.
*Continuous variables were expressed as median (range); †Exchange rate is quoted at 1,161 won to the dollar as of October 8, 2015.
Table 3
Disease-related characteristics of patients with IBD in relation to their preferences for anti-TNF therapy

Values are presented as mean ± standard deviation (SD) or number (%). Group A means ‘preference for intravenous anti-TNF at the hospital every 8 weeks,’ Group B means ‘preference for subcutaneous anti-TNF at home every 2 weeks,’ and Group C means ‘no preference for any biological therapy.’
IBD = inflammatory bowel disease, TNF = tumor necrosis factor, SD = standard deviation, QOL = quality of life, CUCQ-8 = Crohn's and ulcerative colitis questionnaire-8.
In a subgroup analysis comparing group A and B after excluding group C, patients with higher income levels, patients who experienced adverse events with prior medication and patients with a longer disease duration preferred subcutaneous anti-TNF therapy (P = 0.043, P = 0.000, and P = 0.029, respectively). To determine predictors for preference to subcutaneous over intravenous anti-TNF therapy, we performed a logistic regression analysis adjusted for income level, adverse events with prior medication and disease duration, which showed univariate differences between group A and B. In this analysis, high income level (OR 2.0; 95% CI 1.1–3.5; P = 0.026) and an adverse event with prior medication (OR 4.0; 95% CI 2.2–7.2; P = 0.000) were found to be independent predictors for preference to subcutaneous anti-TNF therapy (Table 4).
Table 4
Multivariate logistic regression analysis of predictors for subcutaneous anti-TNF therapy over intravenous anti-TNF therapy
DISCUSSION
This is the largest study on the preferences to anti-TNF therapy in Asian IBD patients. In the present study, intravenous anti-TNF was preferred over subcutaneous anti-TNF with a 2.4:1 ratio in IBD patients. Korean IBD patients might be more familiar with intravenous anti-TNF than subcutaneous anti-TNF, as intravenous anti-TNF was approved five years earlier than subcutaneous anti-TNF in 2005. The main reason given for the preference for intravenous anti-TNF was ‘I don’t like the idea of self-injecting’ (73.4%), and the main reason given for subcutaneous anti-TNF was ‘the convenience of injecting at home’ (73.1%), which were consistent with previous studies (910). In the United Kingdom, intravenous anti-TNF was preferred over subcutaneous anti-TNFs (1.7:1) in 78 IBD patients (10). However, another study reported that subcutaneous anti-TNF was preferred over intravenous anti-TNFs (1.8:1) in 36 CD patients (9). A recent Korean study reported that intravenous anti-TNF was preferred over subcutaneous anti-TNF (1.7:1) in 189 anti-TNF naïve CD patients (11). Results of previous Western studies were not consistent and limited due to the small number of patients from a single center (910). The Korean study was also limited as it included only anti-TNF naïve CD patients (11). Except for IBD, patient preference for anti-TNF therapy have only been reported in patients with rheumatoid arthritis. Rheumatoid arthritis patients predominantly preferred subcutaneous over intravenous administrations (2122), as they had a limited mobility due to rheumatoid arthritis. However, IBD patients may be little influenced by disease characteristics on their preference for anti-TNF therapy.
In this study, approximately 58% of patients preferred shared decision-making. In a survey of 1,056 IBD patients in Germany, 67% of patients preferred shared decision-making (23). In a survey of 1,067 patients in the Netherlands, most (81%) patients reported that shared decision-making was a ‘very important’ process (24). Recently, Siegel et al. (2526) reported interesting survey results for shared decision-making from both patients’ and gastroenterologists’ perspectives. From gastroenterologists’ perspective, only 12% of 106 gastroenterologists had a systemic documented approach for the shared decision-making process (25). From the patients’ perspective, however, over 2/3 of 355 IBD patients reported much satisfaction from shared decision-making (26). In the present study, approximately 2/3 of patients who had previously received or were currently receiving anti-TNFs wanted to change to alternative anti-TNF therapies. Therefore, physicians should provide the shared decision-making process for their IBD patients, especially in choosing anti-TNF therapies. Lower preference rate for the shared decision-making in our study than those from Western studies (232426) might be explained by differences in health care experience, health status, decision and information preferences, and socio-demographic variables (14).
Little is known about the potential predictors for preference to anti-TNF therapy in IBD patients. In the present study, high income level (OR 2.0; 95% CI 1.1–3.5; P = 0.026) and adverse event with prior medication (OR 4.0; 95% CI 1.2–7.2; P = 0.000) were found to be independent predictors for preference to subcutaneous anti-TNF therapy. This makes sense, as subcutaneous anti-TNF therapy may be attractive to patients who are more active or in the workforce (21). Subcutaneous administration may offer patients more flexibility and convenience without need for medical appointments during business hours (27). Furthermore, subcutaneous anti-TNF therapy may be attractive to patients who experienced an adverse event with prior medication as they desire newly-developed medications. Therefore, physicians should discuss the use of anti-TNF therapy with their IBD patients considering these factors. Subcutaneous administration decreased the need for hospital visits, however, travel time to the hospital was not a predictive factor for subcutaneous preference in our study. In another study (11), however, the travel time to hospital was a predictive factor for subcutaneous preference.
The present study had several limitations. First, our study was based on IBD patients from large, tertiary referral centers, which limits the ability to generalize our findings. Our patients may have had a more complicated disease course and therefore referred to our centers. It is possible that, in a general gastroenterology community practice, with patients who perhaps have more mild cases of IBD, patients may have different preferences to anti-TNF therapy. However, anti-TNF therapy is often used for IBD patients with a more complicated disease course in large centers of Korea (28). Second, we recognize that there may be geographic and economic aspects that impact on anti-TNF therapy, which can also limit the generalizability of our findings. Therefore, the preference for anti-TNFs should be reevaluated in different countries, especially in other Asian countries. The final limitation is that our study relied on a hypothetical scenario about the choice of anti-TNF therapies, and respondents may not make the same decision in a real clinical setting.
In conclusion, high income levels and an adverse event with prior medication were independent predictors for preference to subcutaneous anti-TNF therapy. Therefore, physicians should provide shared decision-making to their IBD patients for the mode of anti-TNF administration. Further studies on the preferences to anti-TNF therapy should be reevaluated in IBD patients from other Asian countries.
 XML Download
XML Download