

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Mortality in hemodialysis (HD) patients is higher than in the general population, and cardiovascular disease (CVD) is the leading cause of death (1). This has placed a socioeconomic burden on countries worldwide (2). There are several reasons why HD patients have higher mortality rates. First, risk factors such as hypertension, diabetes, and dyslipidemia are more common in this patient group than in the general population (3). In addition, the uremic milieu in HD patients may accelerate vascular calcification (4), which is a powerful predictor of mortality in dialysis patients (5). Vascular calcification is divided into two categories in HD patients: coronary artery calcification and extra-cardiac calcification (6). The former is a predictor of future cardiac events and can lead to extra-cardiac vascular calcification (7). Thus, monitoring vascular calcification is important in assessing the future risk of cardiovascular and all-cause mortality. Clinical data on vascular calcification were obtained by imaging tests such as simple abdominal X-ray films and computed tomography (CT) scans, and quantified using vascular calcification scores (VCSs). Many biochemical markers associated with vascular calcification have been investigated, such as high-sensitive C-reactive protein (hsCRP), interleukin 6 (IL-6), fetuin-A, and matrix Gla protein (MGP) (8). Similarly, we reported the possibility of associations between soluble receptor for advanced glycation end products (sRAGE) and S100A12 (extracellular newly identified RAGE-binding protein, EN-RAGE) and vascular calcification (9).
Advanced glycation end-products (AGEs), Maillard reaction products, are the result of glycation and are upregulated under hyperglycemic and increased oxidative stress conditions (10). RAGE, a member of the immunoglobulin superfamily, is expressed on cell surfaces and binds to AGEs and other ligands, such as S100/calgranulins, amphoterin, and high-mobility group box 1 (11). Its expression levels are elevated in diabetes and chronic kidney disease (CKD), and its activation leads to inflammatory responses, apoptosis, and prothrombotic activity (12). Thus, RAGE may be associated with atheromatous calcification (13). S100A12, as a ligand for RAGE expressed on macrophages, lymphocytes, and endothelial cells, has a role in atherosclerosis in HD (14). Several studies have already described correlations between CKD and CVD (15, 16). These results may be mediated via the advanced glycation end products RAGE (AGE-RAGE) pathophysiological pathway (12).
Recently, there have been several reports on the correlation between CKD and S100A12 or sRAGE, including in end-stage renal disease (ESRD) (17181920). Theoretically, RAGEs would be expected to be elevated in patients with CKD and to be correlated with cardiovascular mortality, expanded to all-cause mortality. However, previous reports have not shown consistent results regarding this hypothesis. Here, as an extension of our previous report on the correlation between vascular calcification and RAGEs (9), we investigated the relationship between S100A12 and sRAGE and mortality in long-term HD patients.
MATERIALS AND METHODS
Study design and patients
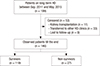
In this prospective observational cohort study, we analyzed 199 outpatient HD patients who visited our HD unit between September 2011 and May 2015. Patients were enrolled in our study if they: 1) had been on HD for at least 3 months; 2) agreed to participate in the study with written informed consent; 3) were free of any complicating condition that could affect serum sRAGE, S100A12, and other inflammatory cytokine levels, such as indwelling catheter, any underlying malignancy, active liver disease, or infection.
All patients were followed up from 9 September 2011 to 19 May 2015 or until death. The observational period of total patients was 44 months with a range of 1 to 44 months. During the follow-up period, 27 subjects died (7 due to infection, 6 due to CVD, 3 due to complications associated with malignancy, 11 due to other causes). In total, 53 patients were excluded from the study (11 received a renal transplant, 33 were transferred to other dialysis clinics, 9 were lost to follow‑up; Fig. 1). Medical records from all patients were reviewed by a single physician. Survival was defined from the day of examination to death or the last follow-up.
Clinical parameters and laboratory analyses
Clinical parameters were obtained based on a medical history interview and a review of the medical records, and included age, the duration of dialysis (months), smoking status, previous CVD history, prescription drugs, and the type of vascular access. Single-pool Kt/V urea (spKt/V urea) was calculated using the Daugirdas equation (21). We checked the systolic and diastolic pressure just before the HD session and calculated the body mass index (BMI) using dry weight.
The VCS was obtained by one physician blinded to the clinical information of each patient. We reviewed plain X-ray images of the lateral lumbar spine and calculated the VCSs, as described by Kauppila (22).
All blood samples were obtained prior to a mid-week HD session after overnight fasting and microcentrifugation for measurements. Serum was separated from blood samples within 1 hour of collection and stored at −70°C until analysis. All biochemistry parameters, including complete blood cell count (hemoglobin, white blood cell [WBC] count, and platelets), albumin, urea nitrogen in serum, hemoglobin, calcium, phosphorus, total cholesterol, triglycerides, high-density lipoprotein, hsCRP, and parathyroid hormone, were measured by standard laboratory techniques using an automatic analyzer (ADVIA 2400 Chemistry System; Siemens, Berlin, Germany). To quantify the serum concentrations of sRAGE (Human RAGE Immunoassay; R & D Systems) and S100A12 (CircuLex S100A12/EN-RAGE ELISA kit; CycLex, Nagano, Japan), commercially available ELISA kits were used, as described in our previous report (9).
Statistical analyses
Values with normal distributions are expressed as means ± standard deviations (SDs) for continuous variables, and values with high inter-individual variability are expressed as medians and interquartile ranges. Comparisons among groups were analyzed using Student’s t‑test. S100A12 and sRAGE values were transformed to a natural logarithmic scale because they were not normally distributed. The correlations between S100A12 and sRAGE with selected parameters were evaluated using Pearson’s and Spearman’s correlation coefficient, as appropriate. Survival analyses were conducted with the Cox proportional hazard model. Univariate and multivariate Cox regression analyses results are presented as hazard ratios (HRs) and 95% confidence intervals (CIs). All statistical analyses were performed using the SPSS software version 20.0 (SPSS Inc., Chicago, IL, USA). For all statistical analyses, P < 0.05 was considered to indicate statistical significance.
RESULTS
Characteristics of patients at inclusion
The clinical characteristics of the 199 enrolled patients are shown in Table 1. The observation period was 44 months. The mean age of enrolled patients was 57.1 ± 13.7 years and they included 108 (54.3%) men. The median duration of HD was 34 months (19–73, interquartile range). The mean BMI was 22.7 ± 3.4 kg/m2 and 85 patients were smokers. In addition, 98 (49.2%) patients suffered from diabetes and 72 patients (36.2%) had CVDs. The spKt/V urea of 191 (96%) patients was > 1.2. In total, 154 (77.4%) patients received HD via an arteriovenous fistula. The mean plasma S100A12 was 410.3 ± 318.1 ng/mL (median: 301.3 ng/mL), but there were no significant differences between survivors and non-survivors (survivors, 403.2 ± 313.8 ng/mL; non-survivors, 455.6 ± 346.8; P = 0.495). The mean sRAGE level was 2.4 ± 1.6 ng/mL, but there was also no significant difference between survivors and non-survivors (survivors, 2.4 ± 1.7 ng/mL; non-survivors, 2.4 ± 1.3 ng/mL; P = 0.482).
Table 1
Baseline characteristics and Pearson correlations with S100A12 and sRAGE

S100A12 = extracellular newly identified RAGE-binding protein, sRAGE = soluble receptor for advanced glycation end products, BMI = body mass index, HD = hemodialysis, CVD = cardiovascular disease, SBP = systolic blood pressure, DBP = diastolic blood pressure, AVF = arteriovenous fistulas, HDL-C = high-density-lipoprotein cholesterol, LDL-C = low-density-lipoprotein cholesterol, VCS = vascular calcification score, WBC = white blood cell, hsCRP = high-sensitive C-reactive protein, IL-6 = interleukin 6.
*r, Pearson’s correlation coefficient for continuous variables and Spearman’s correlation coefficient for categorical variables; †Median (interquartile range); ‡P < 0.05; §P < 0.01.
Correlation analyses between S100A12 and sRAGE with clinical parameters
The results of the correlation analysis are shown in Table 1. There were no correlations between S100A12 and sRAGE and demographic parameters such as age or gender. There was a positive correlation between S100A12 and sRAGE (r = −0.148, P = 0.037). Plasma S100A12 in patients with diabetes was greater than in those without diabetes (r = 0.146, P = 0.040) and plasma S100A12 of the cohort was positively associated with the WBC count, hsCRP, and IL‑6 (WBC count, r = 0.167, P = 0.018; hsCRP, r = 0.299, P = 0.006; IL-6, r = 0.159, P = 0.025). However, sRAGE was not associated with diabetes or inflammatory cytokines (Table 1). sRAGE in the cohort with an arteriovenous graft was higher than the arteriovenous fistula group (r = −0.149, P = 0.036) and sRAGE was negatively associated with the VCS (r = −0.207, P = 0.003).
Cox regression survival analyses with S100A12 and sRAGE
Variables, associated with overall mortality and predict of CVD, were shown Table 2 by univariate cox regression analysis. The parameters associated with overall mortality (HRs; 95% CI; P value) were age (HR 1.055; 95% CI 1.024–1.087; P < 0.001) diabetes (HR 2.333; 95% CI 1.047–5.198; P = 0.038), previous history of CVD (HR 3.214; 95% CI 1.472–7.021; P = 0.003), serum albumin (HR 0.366; 95% CI 0.143–0.934; P = 0.035) and hsCRP levels (HR 1.399; 95% CI 1.070–1.830; P = 0.014). However, there were no significant difference of survival according to plasma S100A12 (HR 1.300; 95% CI 0.796–2.123; P = 0.294) and sRAGE (HR 1.074; 95% CI 0.587–1.967; P = 0.816). Plasma S100A12 and sRAGE could not have a utility for occurrence of CVD (Table 2).
Table 2
Univariate analyses of factors associated with overall mortality and development of CVD
CVD = cardiovascular disease, OR = odds ratio, CI = confidence interval, HD = hemodialysis, BMI = body mass index, hsCRP = high-sensitive C-reactive protein, S100A12 = extracellular newly identified RAGE-binding protein, sRAGE = soluble receptor for advanced glycation end products, IL-6 = interleukin 6, VCS = vascular calcification score.
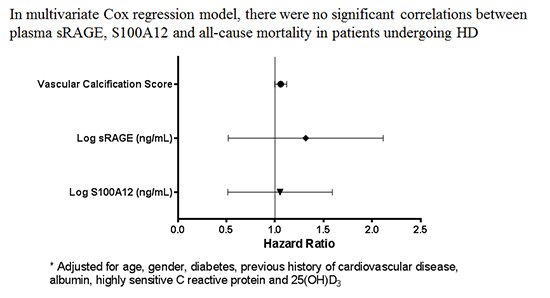
We designed four multivariate Cox regression models to assess whether S100A12 and sRAGE could predict all-cause mortality (Table 3). We adjusted the model using traditional predictors of all-cause mortality and significant markers in the univariate analysis. In all of the models, plasma S100A12 (HR 0.960; 95% CI 0.566–1.630; P = 0.881) and sRAGE (HR 1.155; 95% CI 0.612–2.183; P = 0.656) were not associated with mortality in HD patients (Table 3).
Table 3
Adjusted HR for overall mortality according to levels of S100A12, sRAGE, and VCS

Model 1, adjusted for age and gender; Model 2, adjusted for Model 1 plus diabetes and previous history of cardiovascular disease (CVD); Model 3, adjusted for Model 2 plus albumin, high-sensitive C-reactive protein (hsCRP) and 25(OH)D3.
S100A12 = extracellular newly identified RAGE-binding protein, sRAGE = soluble receptor for advanced glycation end products, VCS = vascular calcification score, HR = hazard ratio, CI = confidence interval.
DISCUSSION
There have been several studies on the association between S100A12 and mortality in patients undergoing HD (17181920). Our results did not reveal any relationship between S100A12 and sRAGE and overall mortality in patients undergoing HD, in contrast to previous studies. Rather, the existing traditional predictors, including age, diabetes, CVD, hsCRP, and albumin, predicted overall mortality in HD. In our results, S100A12 was correlated with inflammatory markers but not with the VCS. In contrast, sRAGE was correlated with the VCS but not with inflammatory markers. In addition, S100A12 was negatively correlated with sRAGE.
Most researches focused on an association between biomarkers including S100A12 and sRAGE and outcomes have been based on accompanying atherosclerosis and vascular calcification as a part of CKD. Previous studies have reported an association between plasma S100A12 in HD patients and overall mortality (171820). However, those studies failed to identify the specific relationship between sRAGE and mortality. In one study, S100A12 showed no association with mortality; the relationship was based on an indirect association with inflammation (19). In addition, there are differences between these previous studies and our study in terms of cohort characteristics. For example, Isoyama et al. (18) included a small cohort of HD patients and thus their data are insufficient to demonstrate the efficacy of S100A12 as a predictive marker for mortality in this patient population. In comparison with other studies (171920), although our subjects had higher proportions of diabetes patients and smokers, reports by Nakashima et al. (20) and Kalousova et al. (19) showed greater proportions of death (46% and 56%, respectively) and previous history of CVD (64% and 61%) than our study (13.6% and 36.2%, respectively). Thus, in univariate analyses, there was a significant correlation between S100A12 and mortality in these previous reports because medical history is a powerful predictor of overall mortality. In addition, the significance disappeared after adjusting for other variables (19). Our results are most similar to Shiotsu et al. (17). Their populations consisted of 550 HD patients and their observation period was 22.5 months. They reported that age, serum levels of albumin, previous history of CVD, and higher levels of S100A12 (≥ 18.79 ng/mL) were correlated with overall mortality (S100A12 ≥ 18.79 ng/mL; HR 2.267; 95% CI 1.195–4.302; P = 0.012). However, we cannot directly compare our results to those results. The normal or reference serum ranges of S100A12 and sRAGE are still debated (23). In addition, the proportions of diabetes and smokers were relatively higher in our cohort than in theirs (diabetes, 49% vs. 37%; smoking, 42.7% vs. 11.8%).
In our study, S100A12 was positively correlated with diabetes, hsCRP, WBC count, IL‑6, and negatively correlated with sRAGE. However, sRAGE was negatively correlated with the VCS but not with inflammatory markers. The relationship between sRAGE and VCS was reported in our previous paper (9).
Since the discovery of AGEs and RAGEs, many studies have been conducted on their roles. The connection between the AGE-RAGE pathway and cardiovascular mortality has resulted in a focus on chronic overstimulation of that pathway in CKD (12). As renal function decreases, AGEs accumulate and RAGE may be overexpressed. However, one study reported that plasma S100A12 was not elevated in patients with decreased renal function who were undergoing HD (24). Mori et al. (14) reported that the level of S100A12 was elevated in HD patients with atherosclerosis. Taken together, these results indicate that plasma S100A12 is associated with inflammation that is not directly associated with decreased renal function.
The level of sRAGE is very high HD patients but decreases after renal transplantation (2425). These RAGEs are involved in many inflammatory processes (24262728). The vascular calcification process is closely related to inflammation, and S100A12 plays a role in it, particularly favoring microcalcification (29). In contrast, sRAGE has anti-inflammatory effects by blocking the interactions between AGEs and cell surfaces and preventing the effects of AGEs (30). Thus, sRAGE affects calcification processes. Because we could not analyze mortality according to causes of death, we do not know whether S100A12 and sRAGE affected CVD mortality. However, we found that these RAGEs do not independently predict all-cause mortality but are involved in inflammation.
There were some limitations to our study. The proportion of death was relatively small, compared to previous studies, and we excluded a good proportion of patients. Second, we used only VCS as an assessment of vascular calcification without determining carotid intimal thickness. Thus, we could not assess whether vascular calcification is associated with mortality in HD patients.
In summary, S100A12 was correlated with inflammatory markers but not with the VCS. In contrast, sRAGE was correlated with the VCS but not with inflammatory markers. Moreover, S100A12 was negatively correlated with sRAGE. Our results did not reveal any relationship between S100A12 and sRAGE and overall mortality in patients undergoing HD, in contrast to some previous studies. Rather, the existing traditional predictors, including age, diabetes, CVD, hsCRP, and albumin, predicted overall mortality in HD.
In conclusion, although plasma S100A12 was partly related with diabetes and inflammation, plasma S100A12 and sRAGE may be weak surrogate markers for predicting all-cause mortality in patients undergoing HD. Future studies are needed set meaningful ranges of plasma S100A12 and sRAGE in HD patients.
 XML Download
XML Download