

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The incidence of first deep vein thrombosis (DVT) in the general population is about 5 per 10,000 person years (1). DVT can lead to pulmonary embolism through multiple mechanisms in the short-term, and chronic venous insufficiency can also be developed from DVT with the incidence of 20%–50% as a long-term sequelae (2). Chronic venous insufficiency after a diagnosis of DVT can be defined as post-thrombotic syndrome (PTS). Conventional anticoagulation therapy has been widely used for DVT, and is the recommended primary treatment modality (34). However, this treatment has not been associated with the rapid resolution of symptoms or the recanalization of the venous occlusion in more extensive cases, such as in iliofemoral DVT (56). Moreover, it is also associated with the long-term disability that accompanies PTS (7). For the more rapid resolution of DVT, several modalities have been introduced, including surgical thrombectomy, catheter-directed thrombolysis, and manual aspiration thrombectomy. Although there have been many studies on the clinical effectiveness of surgical thrombectomy (89) and catheter-directed thrombolysis (1011), there are few reports about the clinical outcomes of manual aspiration thrombectomy combined with the catheter-directed thrombolysis. In this paper, we designed it as a pharmacomechanical endovascular intervention (PMI) (12). Therefore, the aim of our study was to analyze the clinical effectiveness and long-term outcomes of PMI compared to conventional anticoagulant treatment for patients with iliofemoral venous thrombosis.
MATERIALS AND METHODS
Patients
To assess the clinical effectiveness of PMI, we retrospectively reviewed the medical records of patients diagnosed with iliofemoral DVT. Those patients were diagnosed with acute (1 to 14 days) and subacute (15 to 30 days) DVT in our institution regardless of thrombus extension into the below common femoral veins (by duplex ultrasound, computed tomography [CT] venography, and conventional venography), from January 2004 to December 2013. To avoid statistical bias, we selected patients with the onset of symptoms within 30 days.
Initially, detailed information regarding the anticoagulant treatment and endovascular treatment were given to all patients, and the patients were selected the modality of treatment by themselves. Patients who were diagnosed with May-Thurner syndrome (MTS) with iliofemoral DVT were excluded. In addition, patients who had any risk for thrombolysis or anticoagulation (i.e., who had a history of surgery within 2 weeks, cerebrovascular accident within 6 months, and severe hypertension), who had a hematologic disorder affecting the coagulation cascade, who had stent insertion only without thrombectomy, and whose DVT was caused by pregnancy or tumor obstruction were also excluded. The included patients were divided into a group that received PMI followed by anticoagulant drugs (PMI group), and a group receiving anticoagulant treatment alone (ACA group). We then compared the risk factors, effectiveness of treatment, morbidity and mortality, residual DVT-free rate, readmission-free rate, and PTS-free rate during the follow-up period. Follow-up was performed at 2 weeks after discharge, and then every 2–3 months thereafter. Duplex ultrasound or CT venography was routinely performed within the initial 6 months and when there was a suspicion about the patency of venous flow.
Anticoagulant therapy (ACA group)
In accordance with the widely-used anticoagulant protocols, intravenous heparin loading and continuous infusion were performed to attain a therapeutic activated partial thromboplastin time (aPTT) that was 1.5–2.5 times the control aPTT (34). Anticoagulant therapy was then converted to the oral anticoagulant warfarin with a target international normalized ratio (INR) of 2.0–3.0 in all patients. In 6 patients, an inferior vena cava (IVC) filter was inserted via the right internal jugular vein at the beginning of anticoagulation therapy for about 4 weeks. All the inserted IVC filters were removed successfully within 4 weeks after the insertion. We recommended the use of compression stockings for over 2 years.
Pharmacomechanical endovascular intervention (PMI) group
After local anesthesia, an introducer sheath was inserted through the appropriate vein under ultrasound guidance, preferably via the ipsilateral popliteal vein under the prone position. At the discretion of the operator, the calf or femoral veins were also options for venous access. At the start of the PMI, an intravenous bolus of unfractionated heparin (UFH) based on body weight (80 IU/kg) was infused. An IVC filter was inserted in patients with a thrombus in the IVC and possessing the possibility of thrombus migration to the pulmonary artery. In 36 patients, an IVC filter was inserted via the right internal jugular vein before intervention. All the IVC filters were removed successfully within 4 weeks after intervention. Venography was performed to determine the extent of the thrombus. A Desilets-Hoffman sheath (COOK, Bloomington, IN, USA), which is an end-hole sheath, was used for aspiration intervention. If the aspiration intervention was difficult, urokinase infusion with a guiding catheter was performed. Urokinase was infused during the procedure in 52 patients (92.9%) in the PMI group, with a mean dosage of 200,000 units (100,000–600,000 units). PMI was repeatedly performed with venography. After the removal of the thrombus from the affected iliofemoral veins, we completed the procedure and maintained a continuous UFH infusion on the general wards. In PMI group, eight patients underwent stent insertion according to the irregularity of the affected iliofemoral vein. In cases of suspected residual thrombus after PMI, we infused urokinase continuously via the venous sheath overnight. If residual DVT or venous stenosis was diagnosed by duplex ultrasound and CT venography during the admission, we performed a repeat procedure before discharge. All patients took warfarin for at least 6 months, maintaining an INR of 2.0–3.0. We also recommended the use of compression stockings for over 2 years.
Statistical analysis
We used the χ2 test to compare categorical variables and the independent sample t-test for continuous variables. Several long-term results during the follow-up period were analyzed by the log-rank test. A P value less than 0.05 was considered to show statistical significance. The analysis was performed using the Statistical Package for Social Sciences (SPSS) software package (Version 22.0; SPSS Inc., Chicago, IL, USA).
RESULTS
Patients’ characteristics
The records of a total of 102 patients (male:female = 53:49; age range, 19–91 years old) were reviewed and divided into PMI (n = 56) and ACA (n = 46) groups. The median follow-up duration was 30.6 months (range 12.3–117.2; interquartile range [IQR] 34.0 months), with no difference between the groups (ACA: median 31.5, range 12.7–117.2, IQR 31.8 months; PMI: median 29.4, range 12.3–104.1, IQR 39.3 months; P = 0.674).
We performed a statistical analysis of sex, age, and body mass index (BMI) between groups. With the exception of age, there was no statistically significant difference between the groups (Table 1). Mean age was higher in the PMI group than in the ACA group (P = 0.035). Risk factors for DVT, such as chronic renal failure, smoking, trauma, surgery-associated immobilization, malignancy (not directly causing venous occlusion or thrombus), inflammatory bowel disease, history of hormone therapy (including oral contraceptives), and hematologic disease (not affecting the coagulation system, including anemia, lupus anticoagulant, hypereosinophilic syndrome, and Behcet’s disease) were assessed in both groups. There was no significant difference in risk factors between the groups (Table 1).
Table 1
Comparison of risk factors between two groups
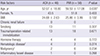
ACA = anticoagulation treatment only group, PMI = pharmacomechanical endovascular intervention BMI = body mass index.
*Statistically significant (P < 0.05); †Hematologic disease: hematologic disease which did not affect the coagulation system such as anemia; ‡Malignancy: malignancy which did not caused direct venous occlusion or thrombus.
Symptoms duration and diseased vein
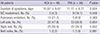
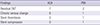
The involved veins and the duration of symptoms were compared between the two groups (Table 2). There was no significant difference in the duration of symptoms, rate of IVC involvement, and the incidence of pulmonary embolism. The side of involved veins did not show statistical difference either.
Table 2
Symptoms duration and involved vein
Procedures during the hospital stays
The mean PMI procedure time was 139.63 ± 6.45 minutes (40–300 minutes) and the patients in the PMI group received an IVC filter more often than patients in the ACA group (ACA: n = 6; PMI: n = 36; P < 0.001). During PMI, we performed a combined procedure, such as balloon angioplasty (n = 6 [10.7%]) or stent insertion (n = 8 [14.3%]) for fear of re-occlusion. For five patients (8.9%) who had suspected remnant thrombus on final venography, we underwent overnight catheter-directed thrombolysis.
Clinical outcomes during the hospital stays
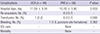
In PMI group, six patients (10.7%) underwent an additional procedure for a confirmed residual thrombus or venous stenosis during hospitalization. These included thrombectomy (n = 4), balloon angioplasty (n = 3), and stent insertion (n = 3) in the iliac vein. Most additional procedures were performed within 1 week (3.5 ± 1.36 days; range 1–14 days) from the initial procedure day.
There was no morbidity or mortality during hospitalization. Although not significant, the incidence of transfusion was higher in the PMI group, which was due to procedure-related blood loss. Table 3 shows patient hospitalization data.
Table 3
Hospital days and complications during admission
Follow-up
Follow-up was performed for at least 12 months. During the follow-up, we checked for clinical signs of chronic venous disease using the clinical, etiology, anatomy, and pathophysiology (CEAP) classification system (13). If the clinical classification was changed, we investigated using an imaging study such as CT venography and Doppler sonography. The symptoms on admission were classified as C1 (telangiectasia, n = 1 [2.2%]), C2 (varicose veins, n = 2 [4.3%]), and C3 (edema, n = 44 [95.7%]) in the ACA group and C3 (n = 56 [100%]) in the PMI group. On the first follow-up visit, the clinical signs of CEAP were categorized as C2 (varicose vein, n = 1 [2.2%]) and C3 (edema, n = 17 [37.0%]) in the ACA group and C2 (varicose vein, n = 1 [1.8%]), C3 (edema, n = 11 [19.6%]), and C4a (eczema, n = 1 [1.8%]) in the PMI group. On final follow-up, there were patients with criteria for C2 (varicose vein, n = 1 [2.2%]), C3 (edema, n = 14 [30.4%]), and C4b (lipodermatosclerosis, n = 1 [2.2%]) in the ACA group and C2 (varicose vein n = 1 [1.8%]), C3 (edema, n = 7 [12.5%]), and C6 (active venous ulcer, n = 1 [2.2%]) in the PMI group. At the last follow-up, there were fewer patients with clinical signs of criteria for C3 in the PMI group than in the ACA group (ACA: n = 14; PMI: n = 7; P = 0.030). The median duration of taking the oral anticoagulant warfarin was 17.1 months (range 5.8–113.8; IQR 23.3 months) in all patients, with no statistical difference between the groups (ACA: median 16.6, range 6.0–113.8, IQR 22.5 months; PMI: median 17.5, range 5.8–98.0, IQR 25.3 months; P = 0.902).
Readmission rates during the follow-up period
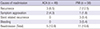
The log-Rank test for the readmission-free rate in the two groups is shown in Fig. 1, with no statistical significance between the groups (P = 0.221). The 1-, 3-, and 5-year readmission-free rates were 91.3%, 88.8%, and 88.8% in the ACA group and 85.7%, 81.5%, and 74.7% in the PMI group, respectively. Although the readmission-free rate did not show statistical significance, the ACA group had a lower incidence of readmission than the PMI group. The causes of readmission are described in Table 4. The recurrence rate was higher in the PMI group because stent-related recurrences were included in the rate. There were no significant episodes of bleeding during the follow-up period except for isolated episodes of gum bleeding and anal bleeding.
Fig. 1
Comparison of freedom free rate from readmission.
ACA = anticoagulation treatment only group. PMI = pharmacomechanical endovascular intervention.
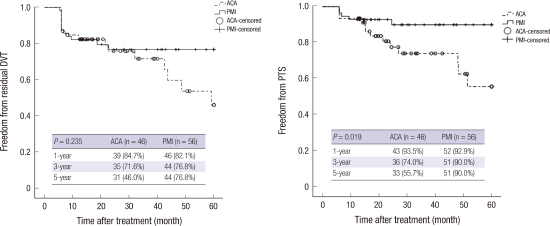
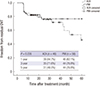
Residual DVT during the follow-up period
In this study, we defined ‘residual DVT’ as remnant thrombus in the deep vein above femoral vein level at final evaluation regardless of partial or total occlusion. The percentage of patients who did not experience a residual thrombus during the 5-year follow-up period is shown in Fig. 2. The 1-, 3-, and 5-year residual DVT-free rates did not show statistical significance between the two groups (ACA: 84.7%, 71.6%, and 46.0%; PMI: 82.1%, 76.8%, and 76.8%, respectively; P = 0.235). After 3 years of follow-up, patients in the PMI had a higher likelihood of not experiencing residual DVT. Because we diagnosed the residual DVT without intravascular ultrasound (IVUS) at final imaging evaluation, this can be a limitation in this study.
Chronic deep venous changes: PTS
The diagnosis of PTS can be ambiguous because the symptoms of PTS can range from mild to severe. In this study, we defined PTS by the chronic venous insufficiency symptoms and signs (based on the CEAP classification, C1–6) with venous flow abnormalities (confirmed by diagnostic studies such as ultrasound, venography, and CT venography). Although residual DVT, venous collateral flow, venous reflux and venous fibrosis were regarded as confirmatory findings of PTS, a patient who had these confirmatory finding without clinical symptoms and signs was not categorized as having PTS. The same definition is applied in reverse.
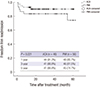
The PMI group had a significantly higher rate of patients without PTS (P = 0.019). The 1-, 3-, and 5-year PTS-free rates were 93.5%, 74.0%, and 55.7% in the ACA group and 92.9%, 90.0%, and 90.0% in the PMI group, respectively (Fig. 3). The study findings are listed in Table 5. We adjusted the PTS-free rate with a Cox-regression model, and the results showed that the rate of patients without PTS was significantly higher in the PMI group as compared to the ACA group (P = 0.047).
Fig. 3
Comparison of freedom free rate from PTS.
(A) Log-rank test for freedom free from PTS between ACA and PMI (P = 0.02).
(B) Cox-regression model for freedom free from PTS between ACA and PMI.
PTS = post-thrombotic syndrome, ACA = anticoagulation treatment only group, PMI = pharmacomechanical endovascular intervention.

DISCUSSION
Despite its long history in the medical literature, the etiology of venous thrombosis was only elucidated in 1856 by Virchow and Sevitt (1415), and the treatment of DVT began relatively recently in the 1930s (16). Current guidelines for the treatment of DVT of the lower extremities recommend anticoagulant therapy for the prevention of thrombus extension, pulmonary embolism, and PTS. Recent antithrombotic guidelines from the American College of Chest Physicians (ACCP) recommend anticoagulant therapy alone over catheter-directed thrombolysis, systemic thrombolysis, and operative venous thrombolysis for acute proximal DVT (17). The American Heart Association (AHA) also recommends anticoagulation as the primary treatment for iliofemoral DVT (18). Although the AHA suggested preventive strategies for PTS in 2014, the fundamental principles were based on appropriate anticoagulation treatment.
The supplementary use of catheter-directed thrombolysis, pharmacomechanical thrombolysis, and surgical thrombectomy for DVT treatment and/or the prevention of PTS should only be considered in selected patients and performed at specialized centers (2). Catheter-directed thrombolysis was recommended in select patients in a review by Gogalniceanu et al. (19). Those authors suggested that the combination of catheter-directed thrombolysis and thrombectomy might be superior to anticoagulant therapy with regards to PTS progression. However, Karthikesalingam and colleagues (12) did not show that percutaneous mechanical thrombectomy had increased effectiveness in PTS prevention.
PTS, the most common long-term complication of DVT (20), is a spectrum of symptoms, ranging from minor leg swelling to severe symptoms such as debilitating leg pain, intractable edema, and leg ulceration (21). Reduced quality of life and increased healthcare costs are some of the long-term concerns due to DVT-induced PTS (2223). Kahn and colleagues (20) identified the predictors of severe PTS, including iliac and femoral vein involvement and the persistence of symptoms after 1 month of treatment. Thus, for more rapid resolution of DVT, other therapies such as systemic thrombolysis, surgical thrombectomy, catheter-directed thrombolysis, and thrombectomy have been introduced (24). Because of excessive bleeding risk and the high failure rate of lysis, the use of systemic thrombolysis has transitioned to catheter-directed thrombolysis (625).
In our opinion, PMI is more time-effective modality in removing thrombus than thrombolysis. In addition, this is also safe procedure. In fact, many studies have reported on the effectiveness of catheter-directed techniques, but few have considered PMI. In addition, the long-term clinical outcomes about PMI with anticoagulation have rarely been reported. Therefore, in this study, we aimed to compare the long-term treatment results and prevalence of PTS after the treatment of acute and subacute iliofemoral DVT with PMI and ACA. According to a multicenter cohort study by Kahn, about 30% of DVT patients develop mild PTS, and 13% of DVT patients have moderate to severe PTS. Although the ACCP and AHA guidelines suggest anticoagulation therapy, we hypothesized that treatment with PMI may have several advantages for the early resolution of DVT in selected patients, as described above. Sevitt (15) revealed that a partial resolution of DVT in many patients in the ACA group was noted during follow-up, but recovery of normal physiologic venous function after anticoagulant treatment was rare. Furthermore, residual thrombus after catheter-directed thrombolysis is correlated with recurrent DVT (26). Although this study had some limitations that we did not used IVUS for the diagnosis of residual DVT and did not subdivide the data whether patients have a thrombus in deep vein below femoral level or not, our data revealed that the residual DVT-free rates and readmission-free rates were not differ between the groups. However, the percentage of patients who did not experience PTS was higher in the PMI group than in the ACA group during the 5-year follow-up period. The pathophysiology of PTS progression is hypothesized to be due to damage to venous valves by thrombi or thrombus-induced inflammatory mediators with residual venous obstruction, leading to increased venous pressure (16). Thus, the complete reversal of DVT within the first month of its diagnosis is very important. According to this study, the use of PMI in addition to ACA may be more effective for PTS prevention than ACA alone. Because our study was a retrospective study with small number of patients, we could not match the symptoms with the Villalta scale (27), but just applied the CEAP classification with venous flow abnormalities for PTS diagnosis. This is another limitation of our study. In addition, we prescribed anticoagulation longer periods than AHA guidance. Although we did not have any experience of complication due to the long-term use of anticoagulant agent, we cannot completely rule out the possibility of the effects of long-term anticoagulation treatment on the role of PTS prevention.
In conclusion, although PMI is invasive, we did not encounter serious morbidity or mortality according to the procedures. In addition, our study revealed that PMI decreased the PTS incidence during the entire follow-up period. Therefore, we suggest that clinicians consider PMI as an effective modality of therapy for acute and subacute iliofemoral DVTs.
 XML Download
XML Download