

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Colorectal cancer (CRC) is among the leading causes of cancer-related death worldwide (1) and is also the fourth-leading cause of death among Korean cancer patients, based on a 2013 report from the Korean National Cancer Center (2). The propagation of an early endoscopic detection program and changes in environmental factors, such as an increase in the adoption of western dietary patterns, have led to continued increase of the CRC incidence in Korea.
The mutation status of BRAF, a gene that encodes a major component of the ERK/MAP kinase signaling pathway, is a molecular classification criterion for CRC. The most common type of BRAF mutation is a CTG → CAG transversion at residue 1799, leading to a substitution from glutamic acid to valine at codon 600 (V600E); this substitution occurs in CRCs, as well as in other malignancies (3). KRAS mutation is generally associated with tumors attributed to the chromosomal instability (CIN) pathway, whereas BRAF mutation is known to be associated with microsatellite instability (MSI), the CpG-island methylator phenotype (CIMP), and the serrated pathway (4). Mutations in BRAF and KRAS are mutually exclusive, and activating BRAF mutations occur almost exclusively in microsatellite-unstable and CIMP-high CRCs (5).
In contrast to other oncogenes such as KRAS, the incidence of BRAF mutation is fairly low among CRCs. This incidence ranges from 5% to 15% according to previous studies. However, the BRAF V600E mutation has been highlighted as a new predictive biomarker of anti-EGFR monoclonal antibody efficacy in CRCs (678). In addition, this mutation is considered a new candidate for targeted therapy. A few researchers have attempted to use the BRAF V600E mutation as a new therapeutic target in advanced and metastatic CRCs (910).
However, the prognostic implication of the BRAF V600E mutation remains controversial. Several studies have shown that the BRAF V600E mutation is associated with poor survival in advanced CRCs, and particularly in microsatellite stable (MSS) CRCs (11). Other studies have failed to prove a relationship between BRAF status and prognosis (1213). Furthermore, characterization of the clinicopathological features of BRAF-mutated CRCs remains unclear. Therefore, we aimed to investigate the association between the BRAF V600E mutation status and clinicopathological features of CRC and to validate the clinical significance of this mutation with regard to survival prognosis.
MATERIALS AND METHODS
Study population and clinicopathological review
Three hundred sixty-five CRC cases registered between 2011 and 2014 were collected from the Konkuk University Medical Center pathologic archives. Fourteen patients who had undergone neoadjuvant chemotherapy and 2 patients who had undergone surgery for recurrent tumors were excluded from the study. Finally, a total of 349 primary CRC cases were evaluated. Two hundred eighteen patients underwent conventional adjuvant chemotherapy comprising FOLFOX (folinic acid/5-fluorouracil/oxaliplatin), FOLFORI, or XELOX (capecitabine/oxaliplatin). Among them, 2 patients were treated with cetuximab, an anti-EGFR monoclonal antibody.
Evaluation of pathologic features
Various demographic features were obtained from the Konkuk University Medical Center electric medical records, including each patient’s age, sex, tumor size, tumor location, treatment methodology, and follow-up history. We also reviewed slides containing hematoxylin and eosin-stained tumor sections. One pathologist (JMH) evaluated the pathological features of the 349 CRCs, including the pathologic (p) T/N stages, tumor differentiation, lymphovascular invasion, perineural invasion, tumor border, tumor budding, Crohn-like lymphoid reaction, peritumoral lymphoid reaction, and proportions of mucinous, signet ring cell, medullary, serrated, and cribriform-comedo components (Fig. 1).
Fig. 1
Histopathological features of CRCs. (A) CRC with positive tumor budding (arrow, ≥ 5 buds). (B) CRC with a marked peritumoral lymphoid reaction and tumor cell destruction by infiltrating lymphocytes. (C) CRC with an active Crohn-like lymphoid reaction (≥ 1-mm-sized lymphoid aggregate). (D) Mucinous component. (E) Signet ring cell component. (F) Medullary component. (G) Serrated component. (H) Cribriform-comedo component. Stain, hematoxylin-eosin; original magnification: 1.25× (C), 40× (B, F, H), 100× (A, D, G), 400× (E, inset of B, inset of G).
CRC = colorectal cancer.
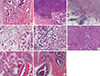
Tumor differentiation was graded according to the 2010 World Health Organization (WHO) classification. The proportion of each component in a tumor was assessed using the following 3 categories based on a previous study by Kim et al. (14): absent, < 50%, and ≥ 50%. The histologic features of each component were determined based on the 2010 WHO classification. Medullary features were defined as a syncytial growth pattern of large tumor cells with a high nuclear/cytoplasmic ratio and prominent nucleoli. Serrated features were defined as glandular serration with abundant eosinophilic cytoplasm, intra- and extracellular mucin, and a lack of tumor necrosis. Cribriform-comedo features were defined as cribriform glandular architecture with central comedo-like necrosis.
Tumor budding was evaluated according to a previous study by Ueno et al. (15). This characteristic was defined as a single tumor cell or cluster of < 5 tumor cells at the invasive front. A tumor with ≥ 5 buds visible in a 200× magnification field was classified as a budding-positive tumor. Peritumoral lymphoid reactions were assessed according to Klintrup’s scoring system (16), as follows: G0, no increase of lymphoid cells at the invasive margin; G1, mild increase of lymphoid cells without tumor cell destruction caused by lymphoid infiltration; G2, band-like infiltration of lymphoid cells at the invasive margin with focal tumor cell destruction by lymphocytes; or G3, cup-like intense lymphoid infiltration at the invasive margin with frequent tumor cell destruction by lymphocytes. An active Crohn-like lymphoid reaction was defined as the presence of a ≥ 1-mm peritumoral lymphoid aggregate, based on the criteria presented by Ueno et al. (15).
Immunochemistry and interpretation of EGFR and p53
An automatic Ventana ES immunohistochemistry staining device (Ventana Medical Systems, Tucson, AZ, USA) was used for all immunohistochemistry (IHC) procedures. Four-micrometer tissue sections were cut, dried, deparaffinized, and rehydrated according to standard procedures. Primary antibodies specific for EGFR (clone E30, dilution 1:100; Dako, Glostrup, Denmark) and p53 (clone D07, dilution 1:500; Thermo Fisher Scientific, Fremont, CA, USA) were used for this study. Internal controls were used in all IHC evaluations to ensure the quality of staining.
EGFR staining was graded using a 4-tiered system (0, 1+, 2+, 3 +) according to the membranous staining intensity and frequency in the cancer cells, as follows: 0, negative/no membranous staining; 1+, faint/partial membrane staining; 2+, weak/complete membrane staining in > 10% of total invasive cancer cells; and 3+, intense/complete membrane staining in > 10% of total invasive cancer cells.
p53 positivity was defined according to the distribution patterns of stained nuclei. Only cases involving widespread positivity among tumor cell nuclei in either the entire tissue section or segments of the tumor sample were considered positive. Tumors with a scattered distribution of positive nuclei were considered negative even if > 10% of the tumor cells exhibited nuclear staining (17).
MSI and BRAF V600E mutation tests
DNA extraction was performed in our study as previously described (18). The MSI status was analyzed via polymerase chain reaction (PCR) amplification with fluorescent dye-labeled primers comprising mononucleotide (BAT25 and BAT26) and dinucleotide markers (D2S123, D5S346, and D17S250) specific for microsatellite sites. MSI was defined as a single-band shift in either of 2 alleles or the appearance of a variably sized band in the cancer sample. Cases were stratified as a high incidence of MSI (MSI-H) when instability was identified in > 30% of markers and as a low incidence of MSI (MSI-L) when instability was identified in < 30% of markers. A MSS status was defined as a lack of definite evidence of MSI.
The BRAF V600E mutation was identified using pyrosequencing as previously described (19). The following PCR and sequencing primers were used: 5'-biotin-TTCATAATGCTTGCTCTGATAGG-3' (PCR, F), 5'-GGCCAAAAATTTAATCAGTGGAA-3' (PCR, R), and 5'-CCACTCCATCGAGATT-3' (Sequencing R). The PCR conditions comprised 50 repeats of a 30-minute incubation at 55°C. Pyrosequencing TM was executed using a single-nucleotide polymorphism (SNP) reagent kit (Biotage, Uppsala, Sweden).
Statistical analysis
The χ2 test was used to analyze differences in various clinicopathological factors between the BRAF V600E mutant and wild-type CRC groups. Student’s t-test was used to compare the mean age and mean tumor size between these two groups. The Kaplan-Meier method was used to produce overall survival curves. The log-rank test was used to analyze differences in survival probability. A Cox regression model was applied to univariate and multivariate analyses regarding survival and used to generate hazard ratios (HRs) and confidence intervals (CIs). All statistical parameters were considered significant at a P value < 0.05.
RESULTS
Demographic features of the patients studied
A total of 349 patients with primary CRC were evaluated in this study. Table 1 presents the various clinicopathological features of the baseline study population. More than half of the tumors were located in the distal colon (proximal, 30.4% vs. distal, 69.6%). More than 90% of cases exhibited moderate differentiation (94.0%). Most cases involved locally advanced tumors. pT3 or pT4 cancers accounted for 77.3% of the total study cases, and lymph node metastasis was also identified in 43.8% of cases (n = 153). Sixty-three (18.1%) of the 349 cancers had already generated distant metastases at the time of diagnosis. Peritoneal carcinomatosis was identified in 30 cases. Of the 349 patients with CRC, 214 had received standard adjuvant chemotherapy after surgery.
Table 1
Clinicopathological features of 349 primary CRCs and relationships with MSI status

CRC = colorectal cancer, MSI = microsatellite instability, MSI-H = microsatellite instable-high, MSS = microsatellite stable, MSI-L = microsatellite instable-low, SD = standard deviation, WD = well differentiated, MD = moderately differentiated, PD = poorly differentiated, LVI = lymphovascular invasion, LA = lymphoid aggregate, EGFR = epidermal growth factor receptor.
*Indicated characteristics were evaluable in 346 cases. Three of 349 CRC cases were excluded from the evaluation because of a lack of appropriate amounts of tumor sample resulting from previous endoscopic polypectomy or submucosal dissection.
Associations between MSI status and clinicopathological characteristics
Among the 349 patients, 35 (10.0%) had MSI-H CRC. Accordingly, we assessed differences in clinicopathological characteristics between MSI-H and MSS/MSI-L CRCs (Table 1). Patients with MSI-H CRC were statistically younger than those with MSS/MSI-L CRC (P = 0.031). Most (25/35, 71.4%) MSI-H CRCs were located in the proximal colon. The MSI-H subgroup included fewer pT4-stage tumors and cases of lymph node metastasis than did the MSS/MSI-L subgroup. Furthermore, CRCs with a MSI-H status were less likely to be associated with distant metastasis (P = 0.002). Histologically, poorly differentiated tumors were more frequently observed among MSI-H CRCs (P = 0.011). However, MSI-H CRC was associated with a lower rate of perineural invasion (P = 0.049). MSI-H CRC was found to more frequently associate with Crohn-like lymphoid reactions and high-grade peritumoral lymphoid reactions (P = 0.010 and P = 0.011, respectively). MSI-H CRCs had a significantly larger mucinous component than did MSS/MSI-L CRCs (P < 0.001). In addition, MSI-H CRCs were more likely to exhibit serrated features, although this difference was not statistically significant (P = 0.064).
Incidence of BRAF V600E mutation and its association with clinicopathological characteristics
BRAF V600E mutation was detected in 20 of 349 (5.7%) cases. We evaluated the relationship between BRAF V600E mutation and clinicopathological characteristics in the investigated tumors (Table 2). CRCs harboring the BRAF V600E mutation were mostly located in the proximal colon (70.0%; P < 0.001). These tumors also more frequently presented with mucinous, signet ring cell, and serrated components than did wild-type CRCs (P < 0.001, P = 0.002, and P = 0.008, respectively). In addition, BRAF V600E-mutated CRCs more frequently exhibited peritumoral lymphoid reactions than did BRAF wild-type CRCs (P < 0.001). These findings were similar to the features of MSI-H CRCs. Several factors associated with a worse prognosis were also found to correlate with the BRAF V600E mutant phenotype. Tumors harboring the BRAF V600E mutation more frequently exhibited poorly differentiated histology, infiltrative borders, and tumor budding, compared to tumors harboring wild-type BRAF (P = 0.007, P = 0.019, and P = 0.015, respectively). Lymphovascular invasion was also more frequent among tumors with the BRAF V600E mutation. Specifically, 12 (65.0%) of 20 BRAF-mutated cases exhibited lymphovascular invasion (P < 0.001). Peritoneal carcinomatosis was also significantly more frequently identified in BRAF-mutated cancers (P = 0.021).
Table 2
Associations between BRAF and variable clinicopathological characteristics

SD = standard deviation, LVI = lymphovascular invasion, WD = well differentiated, MD = moderately differentiated, PD = poorly differentiated, MSI = microsatellite instability, MSI-H = microsatellite instable-high, MSS = microsatellite stable, MSI-L = microsatellite instable-low, EGFR = epidermal growth factor receptor.
*Indicated characteristics were evaluable in 346 cases. Three of 349 CRCs cases were excluded from the evaluation because of an inappropriate amount of tumor for evaluation resulting from previous endoscopic polypectomy or submucosal dissection.
Cancers harboring the BRAF V600E mutation tended to have a larger tumor size and more advanced pathologic T stage, although these differences were not statistically significance (P = 0.051 and P = 0.094, respectively). However, EGFR and p53 immunoreactivity were observed significantly more frequently in BRAF V600E mutant CRCs than in wild-type CRCs (P < 0.001 and P = 0.015, respectively). Mean age, sex, pN stage, and perineural invasion were not found to differ significantly according to BRAF status. In addition, no correlation was observed between the BRAF status and MSI (P = 0.128), although the latter is well known to be associated with BRAF mutation in CRC.
We also evaluated the clinicopathological characteristics of CRCs with respect to BRAF V600E mutation status in the MSS/MSI-L subgroup (Supplementary Table 1). In this subgroup, CRCs harboring the BRAF mutation more frequently exhibited peritoneal carcinomatosis, a proximal location, advanced pT stage, larger tumor size, infiltrative border, tumor budding, and mucinous, signet ring cell, and serrated components when compared with BRAF wild-type CRCs. The former also more frequently exhibited marked peritumoral lymphoid reactions.
Univariate and multivariate survival analyses of various clinicopathological characteristics of CRCs
We evaluated the prognostic value of various clinicopathological parameters, including the BRAF V600E mutation and MSI statuses (Table 3). To ensure a precise statistical analysis, we excluded 22 cases with follow-up durations of < 6 months. Accordingly, 327 cases were subjected to overall survival analysis. The median follow-up duration was 23.1 months (range, 2.1–43.0 months). Fourteen (4.3%) cancer-related deaths were recorded.
Table 3
Univariate and multivariate analyses of overall survival
HR = hazard ratio, CI = confidence interval, LVI = lymphovascular invasion, PD = poorly differentiated, MD = moderately differentiated, WD = well differentiated, MSI = microsatellite instability, MSI-H = microsatellite instable-high, MSS = microsatellite stable, MSI-L = microsatellite instable-low, EGFR = epidermal growth factor receptor.
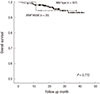
In the univariate analysis, advanced pT and pN stages were associated with poorer overall survival (P = 0.040 and P < 0.001, respectively; Table 3). Distant metastases at diagnosis and/or peritoneal carcinomatosis were also associated with reduced overall survival (P < 0.001 for both). Regarding tumor features, histologic differentiation, lymphovascular invasion, and perineural invasion correlated significantly with overall survival (P = 0.028, P = 0.001, and P = 0.018, respectively), as did the presence of a signet ring cell component (P = 0.042). Patients whose CRCs exhibited marked peritumoral lymphoid reaction (G3) demonstrated poorer overall survival (P = 0.060). However, BRAF mutation and MSI status were not found to be associated with overall survival in the current study (P = 0.773 and P = 0.397, respectively; Fig. 2).
Fig. 2
Comparison of overall survival between patients with BRAF V600E-mutated CRC and those with wild-type CRC among 327 cases of primary CRC.
CRC = colorectal cancer.
A multivariate analysis was conducted to include peritumoral lymphoid reaction and all other factors that exhibited significant associations with overall survival in the univariate analysis. However, only pT stage (HR = 4.212; 95% CI, 1.290–13.752; P = 0.017) remained as an independent prognostic factor of overall survival (Table 3).
We further assessed the prognostic value of BRAF mutation status in stage-stratified subgroups using a Kaplan-Meier survival analysis and log-rank test. However, we found no difference in overall survival between patients with BRAF V600E-mutated CRC and wild-type CRC in each subgroup (stage II/III CRC, P = 0.631; stage IV CRC, P = 0.934). We also evaluated overall survival in several different subgroups through a Kaplan-Meier analysis. However, we found no difference in overall survival between patients with BRAF V600E-mutated CRC and wild-type CRC in each subgroup (CRCs with adjuvant chemotherapy, P = 0.670; MSS/MSI-L CRC, P = 0.759; proximal-located CRC, P = 0.308).
DISCUSSION
In the current study, we evaluated the BRAF V600E mutation statuses of CRCs using pyrosequencing techniques. According to a previous review by Kim et al. (20), the prevalence of BRAF-mutated CRC is lower in Eastern Asian countries than in Western countries. BRAF mutations have been reported to account for 3.7%–20.6% of all CRCs in Western countries, but only 0.7%–11.4% of CRCs in Eastern Asian countries (e.g., China, Japan, and Korea). Similarly, the incidence of BRAF V600E mutation was quite low in the current study, as only 20 (5.7%) cases harbored this mutation. In addition, the incidence of MSI-H CRC was also quite low (10.0%) in this study, as in other studies of Korean patients (21). Various genetic and/or environmental factors appear to influence these ethnic differences; however, the cause of the ethnic molecular heterogeneity observed in CRCs is not yet fully understood.
To characterize BRAF V600E-mutated CRCs, we analyzed associations between the BRAF V600E mutation and other clinicopathological factors. We found that this mutation associated significantly with a proximal tumor location (P < 0.001), poor differentiation (P = 0.007), presence of a mucinous component (P = 0.003), and peritoneal carcinomatosis (P = 0.021). Many previous studies regarding the clinicopathological features of BRAF-mutated CRCs reported results consistent with those of our study. A recent meta-analysis of 25 major studies also revealed that BRAF mutation was significantly associated with poor differentiation, mucinous histology, and a proximal location (22). Generally, BRAF-mutated CRC has been associated with a MSI-H status (252627). Although our study revealed that BRAF mutation was more frequently observed in the MSI-H subgroup (4/35; 11.4%) relative to the MSS/MSI-L subgroup (16/314; 5.1%), this difference was not statistically significant (P = 0.128).
In our study, the BRAF V600E mutation was found to be associated with other histopathological features of CRCs. Specifically, an infiltrative tumor border, lack of lymphovascular invasion, marked peritumoral lymphoid reaction, negative tumor budding status, and presence of a serrated or signet ring cell component were more frequently identified in BRAF V600E-mutated CRCs than in wild-type CRCs. Some of these features have also been identified in MSI-H CRCs (23). Therefore, we assessed the association between BRAF V600E mutation and clinicopathological findings in MSS/MSI-L CRCs. With the exception of tumor differentiation, all features that differed significantly between BRAF-mutated and wild-type CRCs retained this significant difference independently of the MSI status. In addition, pT stage (P = 0.045) and tumor size (P = 0.025) were found to be associated with BRAF mutation.
Tumor-associated inflammatory reactions are commonly observed in various types of cancers and are usually associated with prognostic behaviors. In CRCs, the immune microenvironment has been highlighted as a new marker of prognostic prediction. Tumor-infiltrating lymphocytes (TILs), especially CD8+ T cells, with anti-tumor effects and positive effects on survival have been discovered in several studies of CRC (24). In addition, some studies revealed that MSI might be associated with increased tumor-associated lymphocyte infiltration (2526). Therefore, we evaluated peritumoral lymphoid reaction according to Klintrup’s criteria in the current study. We found that a marked peritumoral lymphoid reaction was associated not only with the MSI-H status, but also with the BRAF V600E mutation independently of the MSI status. However, an active Crohn-like reaction was not found to be associated with the BRAF status. In addition, a peritumoral lymphoid reaction did not have a prognostic effect in the current study.
Whereas the peritumoral lymphocytic reaction is a well-known characteristic of MSI-H CRC, the direct relationship between BRAF mutation and tumor-associated lymphocytic inflammation remained unclear. In contrast to our findings, a previous study by Zlobec et al. (4) revealed that BRAF mutation was associated with the absence of a peritumoral lymphocytic reaction. These authors suggested that this absence might partly explain the poor prognosis of patients with BRAF-mutated CRCs. Yoon et al. (27) further demonstrated a lack of association between CD8+ T cell and FoxP3+ regulatory T cell infiltration and BRAF mutation. Although we cannot explain the association of a marked peritumoral lymphoid reaction with BRAF mutation among MSS/MSI-L CRCs in our study or the clinical implication of this finding, the correlation between BRAF and tumor-associated lymphocytic reactions is clearly controversial, and related studies are limited. Accordingly, additional large population studies are needed.
In the overall survival analyses, only an advanced TNM stage, peritoneal carcinomatosis, lymphovascular invasion, and poor differentiation, all of which are well-known prognostic factors, were associated with poor overall survival. In contrast, although BRAF V600E mutation was associated with peritoneal seeding, lymphovascular invasion, and poor differentiation, it did not associate directly with survival even in the univariate analysis. Notably, this mutation was not related to overall survival even in the MSS/MSI-L subgroup. Furthermore, the MSI status, which is usually considered a prognostic factor for CRC, was not predictive of overall survival in our study.
However, several limitations of our study prevent us from concluding that the BRAF V600E mutation is not associated with prognosis in CRCs. First, the follow-up duration was too short to allow a survival analysis involving significant statistical outputs. In medical statistics, an average follow-up period of at least 5 years should be implemented. In contrast, the mean follow-up period in the current study was only 16 months, and the maximum follow-up duration was < 3 years for all cases. Second, the number of cancer-related deaths during the follow-up period was too small to achieve the minimum statistical power. Only 14 patients died from CRC. Therefore, an additional follow-up is needed to validate the prognostic significance of the BRAF mutation.
In conclusion, the incidence of the BRAF V600E mutation was relatively low in this study, in agreement with previous studies conducted in Eastern Asian countries. BRAF-mutated CRCs exhibited some clinicopathological features which were also frequently observed in MSI-H CRCs, such as a proximal location; mucinous, signet ring cell, and serrated components; and marked peritumoral lymphoid reactions. However, in this study even BRAF mutated CRCs without MSI-H status also show these findings. Thus they are distinct characteristics of BRAF mutated CRCs independently of the MSI status.
 XML Download
XML Download