

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Behçet’s disease (BD) is a complex chronic relapsing inflammatory disorder which is more common along the Mediterranean and Eastern Asia, than in the other areas (1). The mean age of onset of BD is in the early 30s, and the male-to-female ratio varies with ethnicity (2). BD is a neutrophilic perivasculitis with a wide range of cardiovascular abnormalities namely; aneurysms, pseudoaneurysms, vascular ruptures, intra-cardiac and venous thromboses. The low grade of inflammation in course of BD could lead to thromboses and vascular dysfunction (3). In addition, the involvement of thrombosis factors in occurrence of BD has been reported in some studies (45). BD is mainly characterized by recurrent oral and genital ulcers, uveitis, and skin lesions. The disease can involve joints, central nervous system, and the gastrointestinal tract (6).
The etiopathogenesis of BD is not clearly established. However, immune malfunction, characterized by activation in neutrophils and T cells and release of Th1-type pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α), has been considered as the major pathogenetic factor of the disease (789). The association of BD and promoter region of TNF-α gene was firstly reported in Japanese population (10). TNF-α protein, a multifunctional and pro-inflammatory cytokine with confirmed role in activation of macrophages and apoptosis, plays an important role in the regulation of immune system. Moreover, it appears to be in charge of the recurrent inflammatory reactions encountered in BD patients (11). The TNF-α gene lies on the short arm of chromosome 6 (6P21), encoded in the class III region of human leukocyte antigen (HLA) complex, adjacent to HLA-B (12). A number of single nucleotide polymorphisms (SNPs) in TNF-α promoter region have been identified, of which we chose to genotype TNF-α -857T/C and TNF-α -238G/A polymorphisms. It has been shown that the -857C and- 238A alleles cause an increase in TNF-α production (1314). The implication of these polymorphisms in susceptibility to several autoimmune diseases, such as rheumatoid arthritis, ankylosing spondylitis, and systemic lupus erythematosus, has been assessed (151617).
Iran is among the countries in which BD is rather common (18) and this study was designed to determine the frequency of TNF-α -857T/C and TNF-α -238G/A polymorphisms among Iranian Azeri Turkish BD patients.
MATERIALS AND METHODS
Subjects
A total of 161 Iranian Azeri Turkish subjects were included in this study, all the participants were single ethnic Iranian subjects. They were classified into two different groups; BD cases (n = 65), who were diagnosed according to the diagnostic criteria prepared by the international study group for BD (19), and healthy, unrelated, age and sex matched controls (n = 96), to analyze genetic variations in the TNF-α gene promoter region.
DNA Extraction and Genotyping
Genomic DNA was extracted from 2 mL of peripheral venous blood by a modified “salting out” technique (20), precipitated with ethanol and resuspended in sterile distilled water and DNA concentrations were determined with a UV spectrophotometer at 260 nm (Techne, Stone, United Kingdom).
The TNF promoter polymorphism (-238G>A & -857C>T) was evaluated by polymerase chain reaction (PCR) amplifications using sequence specific primers. Briefly, for polymorphism at -238G>A amplification with primer sense 5'-GAA ACC CCC CTC GGA ATC G/A-3', antisense 5'-GGC TGG GTG TGC CAA CAA C-3' and for polymorphism at -857C>T, antisense 5'-TCA CAT GGC CCT GTC TTC G-3' or 5'-CTC ACA TGG CCC TGT CTT C-3', sense 5'-AAG ATA AGG GCT CAG AGA G-3'. For PCR amplification, a total volume of 25 µL, containing 250 ng genomic DNA, 20 pmol of each primers, 300 µmol dNTPs mix (CinnaGen, Tehran, Iran), 1,500 µmol MgCl2, 2.5 µL 10 × PCR buffer (500 mM KCl and 200 mM Tris-HCl; pH 8.4), and 2 units Taq DNA polymerase (CinnaGen) were used.
PCR conditions were as following: denaturation at 94°C for 5 minutes, 35 cycles at 94°C for 35 seconds, 60°C for 20 seconds, and 72°C for 30 seconds, followed by one cycle of final extention at 72°C for 5 minutes. The PCR products were then electrophoresed on 2% agarose gel stained with ethidium bromide and visualized under ultraviolet light (87 bp for TNF -238G>A and 290 bp TNF -857C>T). Primer conx30 was added to each reaction as an internal control (400 bp). Distilled water was used as negative controls. In order to confirm the methodology, 30 samples that were screened by ARMS-PCR were subjected to automated sequence analysis.
Statistical analysis
Statistical analysis was carried out with the SPSS version 16.0 (SPSS Inc., Chicago, IL, USA). Categorical variables were evaluated by standard χ2 or Fisher exact tests, Allele and genotype frequencies were calculated and compared with non-parametric tests followed by Fisher’s exact analysis using STATA version 8 (StataCorp LP, College Station, TX, USA). A P value of < 0.05 was considered significant.
RESULTS
The studied population included 65 BD patients and 96 ethnically matched controls. Patient group included 41 (63%) men and 24 (37%) women (mean ± standard deviation [SD] age, 34.25 ± 9.33). The control group included 54 (56.2%) men and 42 (43.8%) women without BD or other inflammatory diseases.
A total of 65 BD patients and 96 control subjects were both analyzed for two SNPs in the promoter region of TNF-α (at position -238 & -857). The distribution of genotypes for deviation from Hardy-Weinberg equilibrium was tested by Fisher’s exact test (P > 0.05). The allele and genotype distributions of TNF-α -857T/C polymorphism was significantly different between BD Patients and healthy controls. A significant difference was observed between patients with BD and controls, with respect to the allele frequency of TNF-α -857T (P = 0.005; odds ratio [OR] = 0.382; 95% confidence interval [CI] = 0.162–0.886).
Homozygosity for TNF-α -857T/T was observed in the 2 (2.1%) of Healthy controls, but was not observed in any BD Patients. Heterozygosity for TNF-α -857C/T in healthy controls was more than BD Patients (43.8% vs. 21.5%; P = 0.001). The distribution of TNF-α -857 allele and genotype frequencies in BD patients and controls are shown in Table 1. The TNF-α -238G/A polymorphisms were not different between BD patients and healthy controls in this ethnic. The frequencies of TNF-α -238 G/G and G/A genotypes were 6.2% and 93.8% in BD patients, 6.3% and 93.7% in healthy controls and the allele frequencies of TNF-α -238G were 0.53 in BD patients and 0.54 in healthy controls (P = 0.500; OR = 0.96; 95% CI = 0.53–1.73). In previous study, we have already shown a significant association of BD with TNF-α -1031C allele (P = 0.001; OR = 3.08; 95% CI = 1.73–5.47) in the same patients that we further studied in this research (21).
Table 1
TNF-α genotypes and allele frequencies at position -857 in patients with BD and in healthy controls

The frequencies of TNF-α -857C-238G, TNF-α -857C-238A, TNF-α -857T-238G, TNF-α -857T-238A haplotypes were 0.51, 0.471, 0.019, and 0 in BD patients; and 0.491, 0.44, 0.052, 0.017 in healthy controls, respectively (Table 2). Among four haplotypes, TNF-α -857C-238G was the most common haplotype in Iranian Azeri Turkish population. Although distribution of these haplotypes showed no significant association with our patients and control group, haplotype of TNF-α -857C (from this study) and TNF-α -1031C (from the previous study) showed statistically a significant association (P = 0.001) with BD in our cohort (Table 3).
Table 2
Haplotypes of TNF-α promoter region (-238 & -857) in Iranian Azeri Turkish patients with BD and healthy controls
| Haplotypes | Patients, % | Controls, % | P value | OR (95% CI) |
|---|---|---|---|---|
| GC | 51.0 | 49.1 | 0.444 | 1.083 (0.599–1.960) |
| AC | 47.1 | 44.0 | 0.388 | 1.129 (0.622–2.048) |
| GT | 1.9 | 5.2 | 0.056 | 0.353 (0.044–2.148) |
| AT | 0.0 | 1.7 | - | - |
Table 3
Haplotypes of TNF-α promoter region (-857 & -1031) in Iranian Azeri Turkish patients with BD and healthy controls
| Haplotypes | No. of patients | No. of controls | P value | OR (95% CI) |
|---|---|---|---|---|
| CT | 57 | 110 | 0.362 | 0.7843 (0.464–1.324) |
| CC | 33 | 23 | 0.001 | 3.3635 (1.825–6.196) |
| TT | 4 | 33 | 0.001 | 0.1791 (0.061–0.523) |
| TC | 0 | 0 | - | - |
We also analyzed the allele and genotype frequencies according to the clinical features in patients with described clinical characters and those without the clinical characters.
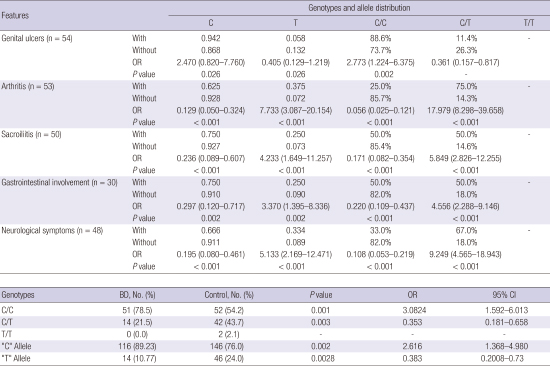
The TNF-α -238G/A polymorphism did not show any association with clinical findings (data not shown). The associations between the frequencies of TNF-α -857C/T genotypes and clinical findings of BD are shown in Table 4. TNF-α -857C/T polymorphisms in BD patients with Posterior uveitis, anterior uveitis, skin lesions, pseudo folliculitis and sided were not significantly different from BD patients without the manifestations (data not shown). However, the TNF-α -857T-allele frequency was significantly higher in patients with arthritis, sacroiliitis, gastrointestinal involvement and neurological symptoms compared with those of patients without the manifestations. Conversely, the TNF-α -857T-allele frequency was significantly lower in BD patients with Genital ulcers than BD patients without this clinical character (Table 4).
Table 4
Genotype and allele distribution of BD TNF-α -857C/T polymorphism between IBD patients and clinical characteristics
DISCUSSION
BD is an inflammatory multi-systemic disorder with unknown etiology and it seems that both genetic and environmental factors trigger the development and severity of this disease. Although, the association of HLA-B51 with BD (22), peculiar geographical distribution of this disease along the old silk route and familial aggregation of BD patients (23) strongly support the contribution of genetic factors to the pathogenesis of BD, disease-susceptible genes yet remain to be determined. In view of the TNF genes’ biological properties and roles of these cytokines in inflammatory disorders, it has been postulated that polymorphic TNF genes could play an important role in the BD (24). The increased levels of circulating TNF-α and enhanced TNF-α mRNA expression in BD has been reported (11). Alterations of the TNF expression related to the polymorphic alleles of TNF genes may implicate a pathogenetic role in the increased activity of this cytokine in BD. To study the influence of TNF-α gene in susceptibility to BD we have already shown a significant association of BD with TNF-α -1031C allele (21). To have a comprehensive study, the distribution of TNF-α promoter -238G>A and -857C>T polymorphisms were investigated in both BD patients and sex-age-ethnic matched healthy controls. These results demonstrated that the frequency of TNF-α -857C allele was significantly higher in Behçet’s patients than in healthy controls and it was strongly associated with BD (P = 0.001; OR = 2.616; 95% CI = 1.129–6.160), whereas the frequency of TNF-α -238A allele was similar in the two compared groups and was not associated with susceptibility to BD in this ethnic group. This is the first report of assessment of TNF-α -857C/T allele promoter polymorphism and its significant associations with BD in patients from Iranian Azeri Turk ethnic group. The results of this study are consistent with results reported in Turkish (2526) and Korean (27) populations. In the aforementioned populations no association was found between TNF-α -238G>A polymorphism and susceptibility to BD. Conversely, the TNF-α association with BD in Caucasian population Ahmad et al. (28), showed the higher frequency of TNF-α -238A allele in BD patients in comparing to that of healthy controls. In a meta-analysis, Touma et al. (29) reported that TNF-α -1031C (OR = 1.35; 95% CI = 1.09–1.68), -238A (OR = 1.51; 95% CI = 1.12–2.04) and -857T (OR = 0.76; 95% CI = 0.58–0.98) had a significant association with BD. The ethnic variation might be responsible for these discordant results in the frequency of -857 and -238 gene polymorphisms between the present study and the other studies (2829).
Haplotype analysis of TNF-α promoter polymorphisms (at positions -857, -1031) in our cohort showed a strong association with BD disease (P = 0.001; OR = 3.36; 95% CI = 1.825–6.196) (Table 3), whereas this association was not seen in haplotype analysis of the other polymorphisms in TNF-α promoter region (at positions -238, -857, -308) (Table 2). These findings are in consistent with a previous report (28) but it differs with some other studies (2730). On the base of our findings the TNF-α -857T-1031T haplotype is associated with resistance to BD (P = 0.001; OR = 0.17; 95% CI = 0.061–0.523) (Table 3).
In order to study the association of BD clinical parameters’ with different genotypes (or alleles), our results showed the significant association of arthritis and sacroilitis with TNF-α -857T allele. Conversely, patients with a positive genital ulcer have a lower frequency of TNF-α -857T allele (Table 4). These findings suggest that TNF-α -857C/T gene polymorphism could have an effect on the development of clinical features of BD in this ethnic group.
In conclusion, the TNF-α -857C, -1031C alleles and their haplotype are significantly associated with BD. These alleles may contribute to the enhanced inflammatory reactivity observed in patients with BD. By considering the effect of geographical variations on occurrence of this disease, the association of TNF-α gene cluster polymorphisms with BD in other ethnic groups needs to be further studied.
 XML Download
XML Download