

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The urologic disease that causes particular but common health problems in a man’s life course not only affects quality of life but also contributes shortening of survival. The urologic disease accounts for a substantial part of medical problem and incurs socio-economic burden (1). Among urologic diseases, urinary tract infection is the most diagnosis commonly made and causes more than 8 million patient visits to hospitals every year in the United States (2). About 15% of all congenital anomalies involve the genitourinary system (3). Urinary cancer in male population was estimated to cause for more than 34% of new cases of all types of tumors and about 14% of death due to cancer (4). About 5%–10% of the population in industrialized countries were known to having symptom of urolithiasis in their life time (5). The prevalence rate of urinary stone disease has reportedly increased in the United States and European countries, as people in developed countries have been exposed to risk factors such as aging and metabolic syndrome (678). Also, injuries of the urinary system or genitalia take 5% of all combat-related trauma and about 34% of all genitourinary injuries are mostly caused by sport related trauma (910).
A number of reports had sought to look at the urologic disease of Korean population. Bae et al. (11) estimated that the annual incidence of urolithiasis of Korea was 457 per 100,000 based a sampled population from the national health insurance review data. Song et al. (12) reviewed the conscription examination data to see the prevalence rate of urologic disease in young men. It showed that 0.46% of a total of 615,382 examinees were having urologic problems at the moment of the examination. Urinary tract infection was the most prevalent diagnosis (0.15%) followed by testicular absence (0.11%) and single kidney (0.04%).
Military service is mandatory for every man in Korea, mostly in their twenties, and it requires them to be screened for medical fitness for the service. Since the fitness of a soldier is expected to be better than general people in order to serve their duty and maintain preparedness for combat (13141516), it might be expected to have lower likelihood of using medical services. On the other hand, most soldiers are likely to be exposed to intense physical activities during exercise, on service, and various types of combat injury by gunshot, land mine and other external forces. Those may affect urologic health of military soldiers, so that it can present unique epidemiology of the population. Although several reports of military population in other countries showed varying epidemiology of genitourinary diseases (1718), urologic health of the Korean military has not been examined. This study sought to see characteristics of urologic diseases in Korean military population with the electronic medical records database of military hospitals.
MATERIALS AND METHODS
Study population & data collection
Eligible patients were searched through the Defense Medical Statistics Information System (DMSIS) with criteria of male active duty members who had visited the Urology Department of the military hospital between 1 January 2008 and 31 December 2013. DMSIS is a system, which is operated by the Armed Forces Medical Command (AFMC), to provide epidemiological information to increase its capability of situational awareness against natural and deliberate disease outbreaks (19). This system offers archiving, querying, and generating functions for the epidemiological data from a database of electronic medical records of nineteen military hospitals across Korea. As military hospitals provide outpatient, inpatient, and emergency services to all active duty soldiers and only outpatient services to recent retirees and civilian workers, n-Defense Electronic Medical Information System (n-DEMIS) has been used to manage medical records in the hospitals. De-identified n-DEMIS information is transferred to the DMSIS server every day. DMSIS contains demographic information such as sex, age, rank, and clinical information based on the International Classification of Diseases 10th edition (ICD-10), medical departments visited, type of services used (outpatient and inpatient), length of stay, and pharmaceutical information. Inclusion criteria were set to extract the urologic disease incidence of active-duty male soldiers only: first visit, patients who have appropriate age and sex information, and urologic diseases diagnosed by the urologist. Female active members, reserve forces, civilian workers, family of active duty members were excluded, accordingly. The final data contains information of 72,248 subjects. Two references of the diagnosis code have been used during the study period: the fifth version of Korean Standard Classification of Diseases (KCD), which is also a translated version of ICD-10, had been applied from 2008 up to 2010 and the sixth version has been using from 2011. The fifth and sixth version of KCD codes were grouped into clinical categories according to opinion of an urologist (SYC) who referred Campbell-Walsh Urology 10th edition (Supplementary Table 1). Numbers of first visits in each diagnosis in outpatients and inpatients were considered as incidence cases in a respective year. Age was categorized into ≤ 20, 21 to 30, 31 to 40, 41 to 50, and ≥ 51 years old. Rank was divided into private, private first class, corporal, sergeant, non-commissioned officer, and commissioned officer according to Korean military class. Korean armed forces consisted of 3 services: the Army, the Navy (Marines included), and the Air Force.
Statistical analysis
In order to calculate annual incidence rates, we cited the total population of each military service in a corresponding year as a denominator from the national defense white paper that has been published biennially by the Ministry of National Defense since 1967. The annual incidence rates of urologic diseases were calculated with applying Poisson distribution to estimate confidence interval (CI) of 95% depending on the total incidence number of each disease (20). All statistical analyses were performed using the SAS software (SAS 9.3; SAS Institute, Cary, NC, USA).
RESULTS
There was a total of 72,248 first visits of active duty male soldiers in increasing trend annually. Most patients belonged to ages of 18 and 30 years, conscripted ranks and Army (Table 1). Urolithiasis, prostatitis, epididymoorchitis, urethritis, and varicocele were frequently diagnosed during six years (Table 2). The outpatient data showed that prostatitis and urethritis ranked in the highest, while varicocele, epididymoorchitis, and urolithiasis occupied two fifth of total hospitalized patients among ten major diseases. Outpatient departments had provided its service to 70% of all patients (Tables 3 and 4). Among prostatitis, acute prostatitis took about 1.7% and the others were chronic prostatitis. In urolithiasis, renal stone took about 22.8% and stone of urinary tract except kidney occupied the rest. In dysuresia, frequency of micturition was the most prevalent diagnosis code that took about 38.8% (data not shown in the tables). The occupied proportions of inpatient service use varied from 2.14% of hematuria to 47.19% of varicocele in 2013 (Table 5). Varicocele, which showed the highest proportion of using inpatient service, presented 17.2 days of hospital stay (95% CI, 16.51–17.90). Dysuresia was found to cause the longest stay (25.11 days; 95% CI, 23.24–26.98) and the shortest stay was observed in urethritis patients (8.71 days; 95% CI, 6.88–10.54).
Table 1
Basic characteristics of the study population

![]()
Table 2
Annual incidence cases of urologic disease, 2008–2013
![]()
Table 3
Annual incidence cases of urologic disease in outpatient department, 2008–2013
![]()
Table 4
Annual incidence cases of urologic disease in inpatient department, 2008–2013
![]()
Table 5
Hospitalization rate and length of stay of urologic diseases
BPH = benign prostatic hyperplasia, HR = hospitalization rate, LS = length of stay, CI = confidence interval, NA = not Available due to lack of data for confidence interval
![]()
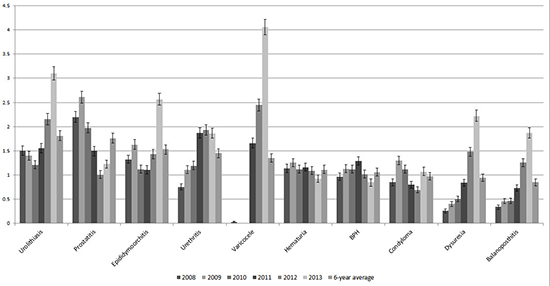
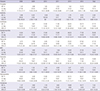
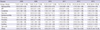
Annual incidence rates in the armed forces and its subordinates are presented in Table 6. Incidence rates of urologic disease varied from 12.3 to 34.2 cases per 1,000 person-years. The incidence rate of urolithiasis in 2013 doubled from that of 2008: 1.5 per 1,000 population in 2008 and 3.14 per 1,000 population in 2013. In addition to a gradual increase of urolithiasis, sharp increases of epididymoorchitis, varicocele, dysuresia, and balanoposthitis were observed during the period. However, the rate of prostatitis had been decreased from 2.2 per 1,000 population in 2008 to 1.25 per 1,000 population in 2013. When we separated data into three services, the Army showed relatively higher incidence rates during the period than the Navy and the Air Force. Sudden increases of incidence rates of varicocele in three services are remarkable: 2.45 per 1,000 population in 2012 and 4.12 per 1,000 population in 2013. While the incidence rates of urolithiasis in the Navy remained constant, that of the Army and the Air Force noticeably increased in 2013. The urologic disease in conscripted soldiers showed very different disease distribution from the entire military population: Epididymoorchitis was the highest disease followed by urolithiasis, dysuresia, and balanoposthitis in 2013 (Table 7). Benign prostatic hyperplasia was not identifiable among conscripted soldiers contrary to that in entire military population.
Table 6
Annual incidence rates of urologic disease from 2008 to 2013 by service (per 1,000 population, [%])

![]()
Table 7
Annual incidence rates of urologic disease in conscripted personnel from 2008 to 2013 (per 1,000 population, [%])
![]()
DISCUSSION
We sought to see incidence rates of urologic diseases in Korean military population by reviewing 6-years electronic medical records from nineteen military hospitals. Few studies have shown for a number of urologic diseases (1112). As we reviewed a full range of diagnosis made in the urology department in military hospitals, we were able to describe incidence rates and volume of services provided to military personnel.
Given that urolithiasis has been known as the most common urologic disease in civilian population, it was consistent in our analysis: urolithiasis was the most prevalent disease across the study period. Although our study showed a lower incidence rate of urolithiasis than that of Bae et al.’s study (11), 1.8 and 4.5 per 1,000 population, respectively, it should be noted that the incidence rate of this study was calculated from active duty soldiers who visited military hospitals with obvious symptoms from urolithiasis. Urolithiasis patients with mild symptoms might have been managed in primary medical facilities rather than in military hospitals. In addition, stone occurrence was known to be lower before age 20 but peaks in incidence in age 30 to 50 (21). Since higher body mass index increases chance of having urolithiasis (22), better physical fitness of military personnel might contribute on lowering incidence rate of urologic stone disease.
This study showed that chronic prostatitis occupied 9.3% total urologic cases and ranked the second most common disease. Depression, voiding problem, and other urinary symptoms, which chronic prostatitis can cause, are not life-threatening symptoms, but those can impair quality of life during the military service (23). This suggests that psychological symptoms caused by urologic diseases should be managed properly to prevent possible adjustment problem in military setting.
Urologic infection consists of epididymoorchitis, urethritis, condyloma, and balanoposthitis. Infection accounted the largest portion of urologic diseases in the population. The epidemiology of epididymoorchitis has not been known well, particularly in young males. Collins et al. (24) reported that 0.29% of 60,000 visits were diagnosed as epididymoorchitis. In 2002, epididymoorchitis took only 0.69% of outpatient visits in the United States (25). However, our data showed that epididymoorchitis took 6.1% of outpatient visits and 12.8% of inpatients. A study, which reviewed hospital visit data of the Armed Forces Capital Hospital in the 1970s, showed that 14.7% of urological inpatients had been diagnosed epididymoorchitis (26). This highlights that further study is needed to find any contributing factor on higher incidence of the disease in Korean military population. According to research in other countries, young age and sexual activity contribute on increasing incidence of epididymitis (2527). Polish incidence rate of urethritis was 2.19 per 100,000 person-year and that of condyloma was 1.1 per 100,000 person-year (28). In a Japanese boy cohort, urethritis was observed in 15% of uncircumcised boys (29). The incidences of epididymoorchitis, urethritis, and condyloma were higher than other studies, but the incidence of balanoposthitis was lower than other study. The higher incidences of epididymoorchitis, urethritis, and condyloma may be contributed by their high sexual activity. The low incidence of balanoposthitis might be related to very popular circumcision practice in Korea (30). The frequency of balanoposthitis could be increased in uncircumcised men (31). Although circumcision has been rarely practiced in most European countries, Latin America, and Japan (32), circumcision has been practiced to mostly school age children in Korea and a study revealed that a circumcision-friendly social atmosphere and a collective belief on hygiene of male genital organ drive such high rate of the practice (33).
Given that a soldier is entitled to get free medical service during the service, many military physicians do not need to consider cutbacks of medical charges or out-of-pocket payment from patients. This may explain why the hospitalization rate and the length of stay of military hospitals are notably frequent and longer than those of civilian hospitals. In this study, it was shown that mean length of stay (16.2–22.6 days) in military hospitals was longer than that of length of stay (9 days) in civilian hospitals (34). The frequency of service provision to urologic patients is affected not only by disease occurrence but also by change of health policy, transportation, and even unit training schedule. An outburst of total urologic patients in 2013 can be explained by implementation of regular health check-ups for all corporals across services to be screened for prevention of avoidable loss. As this health screening policy emphasized that all enlisted soldiers should visit hospital at least once during their 2-years services, the likelihood of being diagnosed asymptomatic urologic diseases or with mild symptoms might be increased.
We should note a number of limitations of this study. First, this study might underestimate true incidence of urologic disease in Korean military population since we analyzed only medical records from military hospitals. Mild urologic diseases such as urethritis or balanoposthitis could be managed in primary medical treatment facilities than in military hospitals. This may contribute to underestimation of true incidence and lead to describing patients who have relatively severe urologic symptoms and need advanced care only. In addition to exclusion of primary level facilities, it was not available to investigate soldiers who visited civilian hospitals since the health insurance claim data has not been shared between the National Health Insurance Service (NHIS) and AFMC. Conscripted soldiers have been covered by the national health insurance to ensure the right to get quality medical services from civilian hospitals since 2004 (35). If a commander of a military unit approves, a soldier may get medical service from a civilian hospital unless in emergency case. If in emergency, medical evacuation is initiated to ensure timely and definite care within the military health system. However, a patient can be referred to a civilian hospital if it needs far advanced care over than capacity of the military hospital. Despite of various benefits to conscripted soldiers through the health insurance, the claim data has been collected only for administration purpose while being shared with AFMC very limitedly. Once the claim data is shared with AFMC, military medical researchers will be able to produce the incidence rate accurately. Second, some parts of data of urologic diagnoses were missing since the category has been changed while updating the fifth KCD to the sixth by 2011. For example, very few incidence cases of varicocele had been reported during 2008 to 2010, contrary to high incidence cases during 2011–2013. A consistent disease categorization is needed to get more robust data not only in urologic diseases but also in other area. Third, identification of any clinical risk factor for urologic disease in military setting was not possible since DMSIS provides limited range of data only for epidemiological and managerial purpose. If de-identified clinical data such as laboratory and ultrasonographic results is available through the system, risk factors in young male population would be identifiable. This will give a chance to see how exposures in the military service, physical activity, climate of their base, sexual activity, and other factors, are linking with urologic health.
Although Korean military occupies largely in young male population and the urologic health is known to be highly related to quality of life in men, it has been rarely addressed. More serious attention should be considered for promoting urologic health of the population based on scientific evidence. If the current trend of health service use for treatment of urologic disease continues, it will occupy a significant volume of health service use in near future. To ensure better urologic health of active duty male soldiers, further study should be followed to optimize the health service delivery and to identify any linkage of urologic diseases and potential occupational exposures during the service.
 XML Download
XML Download