

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Subclinical hypothyroidism (SCH) is characterized by a slightly elevated thyroid stimulating hormone (TSH) serum level (usually < 10 mIU/L) when the serum concentrations of free and total triiodothyronine (T3) and thyroxine (T4) are within the reference range (12). SCH occurs in 4%–20% of the adult population, of which prevalence varies according to age, sex, body mass index (BMI), race, dietary iodine intake, and the cutoff concentrations of serum TSH (1). In the pediatric population, prevalence of SCH is estimated to be less than 4%, although epidemiologic studies are lacking (34).
The natural history of SCH varies depending on its etiology. Many thyroidal and non-thyroidal diseases can cause SCH. However, causes are not identified in conditions of isolated non-autoimmune hyperthyrotropinemia (iso-NAHT) or idiopathic SCH (15). Hashimoto’s thyroiditis (HT) is the most common thyroidal cause of SCH in both adults and children, followed by iso-NAHT (167).
SCH is usually reversible in pediatric patients (47891011), however, some pediatric patients with SCH eventually develop overt hypothyroidism. While predictors for progression to overt hypothyroidism have been replicated in adult studies (12), studies in children have been small (610).
This study aimed to investigate whether the presence of HT independently deteriorates thyroid function in children and adolescents without concomitant diseases. The natural history of SCH and predictors for initiating levothyroxine medication were also evaluated in the HT and the iso-NAHT patients, respectively.
MATERIALS AND METHODS
Subjects
The medical records of 288 patients (5−18 years of age) diagnosed with goiter and SCH between January 2005 and September 2014 at Seoul National University Children’s Hospital were retrospectively reviewed. SCH was diagnosed by at least two measurements of elevated TSH levels (defined as 4.2–10 mIU/L) with normal concentrations of free T4 and total T3. Patients who had underlying diseases (n = 122) such as chromosomal disorders, autoimmune diseases, malignancies, or other chronic disorders, and those who were treated with medications affecting thyroid function (n = 40) were excluded. An additional 17 patients who did not have a second visit were also excluded. In total, 109 patients with SCH were included.
Clinical and biochemical data
Height was measured with a standard stadiometer (Holtain Ltd., Crymych, United Kingdom) to the first decimal place, and body mass index (BMI) was calculated as weight divided by squared height (kg/m2). Age- and sex-specific z-scores for height, weight, and BMI were assigned based on the 2007 Korean National Growth Charts (12). Patients were classified according to BMI as lean (< 85th BMI percentile), overweight (85–95th BMI percentile) or obese (≥ 95th BMI percentile). History of thyroid diseases in first and second degree relatives was also investigated.
All subjects underwent physical examinations by 3 pediatric endocrinologists. Pubertal status was assessed by Tanner staging for breasts (females) and genitals (males). Goiter was graded according to the World Health Organization (WHO) criteria: 1) Grade 0 = not palpable and not visible, 2) Grade 1 = palpable but not visible (1a = not visible with neck extension, 1b = visible with neck extension), and 3) Grade 2 = palpable and visible (13). Once a goiter was identified clinically by a pediatric endocrinologist, neck ultrasound was performed at the discretion of the clinician evaluating the patient, especially in cases with a considerably enlarged (WHO grade 1b or 2) and/or firm thyroid gland in which palpation for nodules was difficult. Neck ultrasound was performed in 39 (33.0%) patients by a pediatric radiologist. Subjects with thyroid nodules or malignancies were not included in our study.
Regular follow-up evaluations of serum thyroid function and thyroid autoantibodies were performed every 3–6 months. Serum concentrations of free T4 and TSH were measured by immunoradiometric kits (RIAKEY; Shin Jin Medics, Seoul, Korea). The serum levels of T3, anti-thyroid peroxidase antibodies (TPOAbs) and anti-thyroglobulin antibodies (TGAbs) were determined by radioimmunoassay kits (Brahms DYNOTest; Diagnostica GmbH, Berlin, Germany). The normal ranges of serum free T4, TSH, and T3 were defined as 0.70–1.80 ng/dL (9.01–23.2 pmol/L), 0.4–4.1 mIU/L, and 87–184 ng/dL (1.34–2.83 nmol/L), respectively. Both titers of TPOAbs and TGAbs were considered to be positive for values higher than 60 U/mL.
Thyroid autoimmunity was investigated by the measurement of serum concentrations of TPOAbs and TGAbs. In patients with HT, TGAbs and TPOAbs were each assessed separately and grouped as follows: 1) group 1 = normal level of either TGAbs or TPOAbs, 2) group 2 = increased less than 10 times above the upper normal limit, and 3) group 3 = increased more than 10 times above the normal limit. A diagnosis of iso-NAHT was based on the findings of isolated TSH elevation with normal free T4 and T3, no signs or symptoms of hypothyroidism, and the absence of thyroid autoantibodies (14).
Levothyroxine therapy was indicated in patients with SCH who had serum TSH concentrations > 10 mIU/L (7). The prevalence rates of children who reverted to a normal TSH level, continued to be SCH status, or eventually started levothyroxine therapy during the follow-up period were analyzed.
Statistical analysis
All continuous variables were described as mean ± standard deviation. Analysis for normality was firstly performed and nonparametric variables were log-transformed for further analysis. To compare two groups, Student’s t-test was used for continuous variables and χ2 test or Fisher’s exact test was performed for categorical variables. The χ2 test for trend analysis was used to compare the proportion of age groups at initial diagnosis (5.0–9.9, 10.0–13.9, and 14.0–17.9 years) and thyroid status at last follow-up (euthyroidism, SCH, and overt hypothyroidism) according to the presence of thyroid autoimmunity (between HT and iso-NAHT groups). Probability of requiring levothyroxine medication plots were constructed using the Kaplan-Meier method, and the two groups were compared by the log-rank test. The Cox proportional hazard model was used to compare HT and iso-NAHT groups after adjusting for confounding variables and to analyze the predictors of requiring levothyroxine medication of each group. The hazard ratios (HRs), 95% confidence interval (CI), and P values were reported. P values less than 0.05 were considered statistically significant. All statistical analyses were performed using the SPSS statistical software (version 21.0; SPSS Institute, Chicago, IL, USA).
RESULTS
Baseline characteristics at diagnosis
Clinical and biochemical characteristics of 109 patients (91 females) are shown in Table 1. The mean age was 9.2 ± 2.6 years (range 5.1–18.0) and 48 patients were prepubertal (44.0%). Thirty patients (27.5%) were overweight or obese and 32 (29.4%) had a family history of thyroid disease. Grade 2 goiter was found in 29 patients (26.6%). None complained of any clinical symptoms of hypothyroidism.
Table 1
Comparison of clinical and biochemical characteristics at initial diagnosis between HT and iso-NAHT patient groups
Continuous variables are described as mean ± standard deviations.
HT = Hashimoto’s thyroiditis, iso-NAHT = isolated non-autoimmune hyperthyrotropinemia, BMI = body mass index, FH = family history, T4 = thyroxine, T3 = triiodothyronine, TSH = thyroid stimulating hormone, TGAbs = thyroglobulin antibodies, TPOAbs = thyroid peroxidase antibodies.
*Log-transformed for Student’s t-test; †
P values < 0.05; ‡TGAbs and TPOAbs were separately grouped into normal levels of one of either antibodies, elevated less than 10 times above the upper normal limit or elevated to more than 10 times above the upper normal limit.
While 37 patients were eventually diagnosed with HT (33.9%, HT group), 72 remained idiopathic during the follow-up period (66.1%, iso-NAHT group, Table 1). The proportion of patients in the HT group increased significantly according to age, from 26.3% for 5.0–9.9 year-olds, to 50.0% for 10.0–13.9 year-olds, and 57.1% for 14.0–17.9 year-olds at diagnosis (P = 0.013 by χ2 test for trend analysis, Fig. 1). Patients of the HT group were significantly older than those of the iso-NAHT group at diagnosis (mean 10.1 vs. 8.8 years, P = 0.011), although the proportion of prepubertal children did not differ between the two groups. The proportion of sex, overweight or obesity, family history of thyroid disease, and goiter size was similar between the HT and iso-NAHT groups. Serum concentrations of TSH, free T4, and total T3 were not different between the two groups (Table 1).

Natural course of SCH: comparison between the HT and iso-NAHT groups
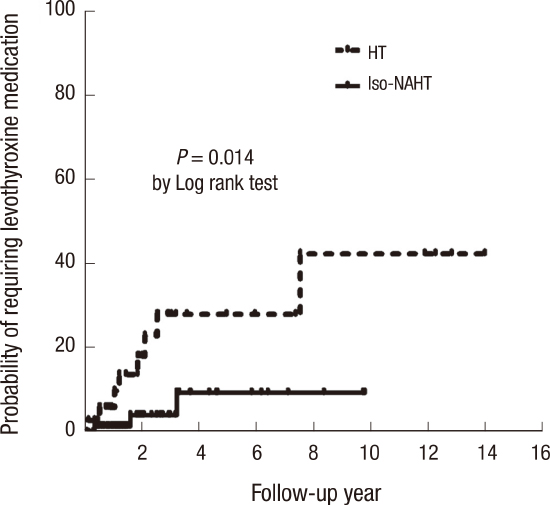
The natural courses of SCH in the HT and iso-NAHT groups are compared in Table 2. During the median follow-up of 2.0 years (range 0.1–15.2), 32 (29.4%) remained in the SCH state and 66 (60.6%) showed normalization of TSH concentrations, whereas 11 patients (10.1%, 8 HT and 3 iso-NAHT; 4 prepubertal and 7 pubertal) eventually started levothyroxine. Levothyroxine was started at a median age of 10.0 (6.7–24.8) years in the 8 HT patients, and at 5.7, 8.3 and 12.7 years (2 prepubertal and 1 pubertal) in the 3 iso-NAHT patients (Supplementary Fig. 1).
Table 2
Comparison of clinical and biochemical characteristics at the time of initiating levothyroxine or last follow-up between patients with HT and those with iso-NAHT
Continuous variables are described as means ± standard deviations.
HT = Hashimoto’s thyroiditis, iso-NAHT = isolated non-autoimmune hyperthyrotropinemia, T4 = thyroxine, T3 = triiodothyronine, TSH = thyroid stimulating hormone, TGAbs = thyroglobulin antibodies, TPOAbs = thyroid peroxidase antibodies.
*Log-transformed for Student’s t-test; †
P- values < 0.05; ‡TGAbs and TPOAbs were separately grouped into normal levels of one of either antibodies, elevated less than 10 times above the upper normal limit or elevated to more than 10 times above the upper normal limit.
Compared to the iso-NAHT group, the HT group showed a higher proportion of patients who eventually required treatment with levothyroxine (21.6% vs. 4.2%). The proportion of patients who remained in the SCH state (32.4% vs. 27.8%) was also higher, and there were a lower proportion of patients who underwent normalization of TSH concentrations at last follow-up (45.9% vs. 68.1%) (P = 0.008 by χ2 test for trend analysis, Fig. 2A) in the HT group. The probability of requiring levothyroxine mediation was significantly higher in the HT group than in the iso-NAHT group (P = 0.014 by the log-rank test, Fig. 2B). Baseline TSH levels greater than 7.0 mIU/L was a risk factor related to later levothyroxine medication with marginal significance (P = 0.057). The presence of HT at diagnosis of SCH was an independent predictor for later levothyroxine medication (HRs = 4.6 vs. iso-NAHT, P = 0.025) after adjusting for age, sex, baseline TSH levels, initial goiter size, and family history of thyroid disease.

Predictors for thyroid dysfunction in each patient with HT and iso-NAHT
In an analysis of the HT group, grade 2 goiters (P = 0.047) and high titers (more than 10 times above the upper normal limit) of TGAbs (P = 0.006) were risk factors for later levothyroxine medication. Age, sex, baseline TSH levels, and TPOAb titers were not significant risk factors for later medication. The Cox proportional hazard model showed that high titers of TGAbs was an independent predictor for later medication (HRs = 28.2 vs. normal TGAbs, P = 0.013, Table 3). In an analysis of the iso-NAHT group, male sex (P = 0.028), and baseline TSH levels greater than 7.0 mIU/L (P = 0.003) were significant risk factors for later levothyroxine treatment. However, independent prognostic factors were not identified in the iso-NAHT group in the Cox proportional hazard model (data not shown).
Table 3
Predictors for levothyroxine therapy in patients with HT
HT = Hashimoto’s thyroiditis, HR = hazard ratio, CI = confidence interval, TSH = thyroid stimulating hormone, FH = family history, TGAbs = thyroglobulin antibodies, TPOAbs = thyroid peroxidase antibodies.
*High TGAbs and TPOAbs were defined as serum levels of antibodies elevated more than 10 times above the upper normal limit.
DISCUSSION
During a median follow-up of 2 years in pediatric SCH patients without concomitant chronic disorders, the majority (89.9%) of patients, whose TSH levels were less than 10 mIU/L, reverted to normal TSH levels or maintained SCH status. Only 10.1% of pediatric SCH patients eventually initiated levothyroxine with a significant difference between the HT and iso-NAHT groups (21.6% vs. 4.2%). Presence of HT itself was an independent risk factor for later levothyroxine medication.
In most pediatric SCH patients with TSH levels less than 10 mIU/L, TSH concentrations remained stable or normalized during follow-up. Studies of the natural courses of SCH in children and adolescents have revealed favorable evolution and lower risk of levothyroxine treatment (9111516). Idiopathic SCH is more likely to resolve spontaneously. According to a prospective evaluation of pediatric iso-NAHT, 88% of patients showed normalization or maintained stable TSH levels (8). On the other hand, approximately 50% of SCH patients with HT were eventually given levothyroxine treatment during median 5 years of follow-up, regardless of concomitant chronic disorders (Turner’s syndrome, celiac disease and type 1 diabetes mellitus) (17). Thus, thyroid autoimmunity is an important determinant in the development of overt hypothyroidism.
The results of our study support the recent prospective report showing higher risk of levothyroxine treatment in 32 patients with HT (53.1%) than 90 patients with iso-NAHT (11.1%) (10). While thyroid autoimmunity is a well-known predictor of thyroid dysfunction in the adult population (18), only small studies have been conducted in the pediatric population. Another retrospective study comparing 87 HT children with 59 iso-NAHT children did not show significant differences in the tendency towards thyroid dysfunction between the groups (22% vs. 14%) (6). Although our study is limited to its retrospective design and variable follow-up period, it is strengthened by the inclusion of homogeneous pediatric SCH patients without concomitant chronic diseases and statistical adjustment of different follow-up years using the Kaplan-Meier survival analysis and the Cox proportional hazard model.
The importance of thyroid autoantibodies at diagnosis of SCH has been emphasized in the pediatric population as well as the adult population. HT patients with high TGAb titers should especially be carefully evaluated for progression to overt hypothyroidism, a finding consistent with previous studies (617). Independent predictors for thyroid dysfunction were not identified in our patients with iso-NAHT. This may have been due to the small sample size, extremely low risk for levothyroxine medication, and lack of extensive investigations for other possible factors associated with iso-NAHT (TSH receptor gene mutation or iodine intake etc.). Heterozygous mutation of TSH receptor mutations related to a loss of function of the TSH receptor plays a role in TSH resistance, leading to iso-NAHT and SCH (5). Further studies are needed to find predictors for thyroid dysfunction in pediatric patients with iso-NAHT.
SCH of younger children was more likely to be idiopathic, while the proportion of HT patients increased with age at diagnosis (Fig. 1), as shown in other studies (67). Unexpectedly, 2 of 3 children with iso-NAHT and 2 of 8 patients with HT were prepubertal at the time of initiating levothyroxine medication (Supplementary Fig. 1). Although thyroid volume can increase during puberty (1920), and thyroid hormone requirements may increase during the pubertal growth spurt (2122), thyroid dysfunction can develop irrespective of pubertal onset. Furthermore, a previous prospective study with iso-NAHT patients reported that normalization of TSH concentrations was less evident in prepubertal patients than pubertal patients (8).
In conclusion, pediatric SCH patients with TSH levels less than 10 mIU/L mostly showed a benign and self-remitting course. Approximately 10% of pediatric SCH patients without concomitant chronic diseases eventually started levothyroxine medication regardless of pubertal onset. A higher risk for hypothyroidism in patients with HT (especially those with high titers of TGAbs) compared to those with iso-NAHT was evident in the pediatric population.
 XML Download
XML Download