

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Patent ductus arteriosus (PDA) is common in extremely premature infants, affecting 60%–70% of infants with less than 28 weeks of gestation (12). While the ductus arteriosus remains open, blood flows left-to-right from the aorta into the pulmonary arteries, causing pulmonary edema, respiratory failure, and compromised perfusion of the bowel, kidney, and brain. There are strong epidemiologic evidences supporting that PDA is associated with numerous morbidities of preterm infants, such as intraventricular hemorrhage (IVH), necrotizing enterocolitis (NEC), retinopathy of prematurity (ROP), and bronchopulmonary dysplasia (BPD) (3456). However, the extent to which these adverse outcomes are attributable to the hemodynamic consequences of ductal opening has not been established, and neither the best tools nor optimal thresholds to identify infants at greater risk for adverse outcomes have been delineated. Additionally, there is no consensus about the optimal timing of PDA treatment (78).
The definition of hemodynamically-significant PDA (hsPDA) varies between clinicians and centers, as well as between trials of PDA treatment (9). Many investigators have used echocardiography alone, or in combination with physical examination findings and cardiac biomarkers such as brain natriuretic peptide (BNP) to more objectively define an hsPDA (10). The traditional approach proposed by Kluckow and Evans (11) noted that a transductal diameter greater than 1.5 mm would be considered significant. Recently, McNamara and Sehgal (12) proposed the criteria and classification of hsPDA which use both clinical and echocardiographic findings. There are some reports about the association between the severity of hsPDA defined by echocardiography according to the McNamara and Sehgal’s classification and the neonatal outcomes (13). However, the clinical criteria used in the McNamara staging system is non-specific and there are no studies searching for the efficacy of PDA treatment on neonatal outcomes according to the presence or severity of clinical symptoms.
Until the year 2013, our unit performed ibuprofen treatment for a PDA with a transductal diameter ≥ 1.4 mm/kg adapting the proposal by Kluckow and Evans (11). From 2013, our unit has adopted new strategies for the treatment guideline of hsPDA that are more focused on the presence of clinical symptoms as well as on the echocardiographic and radiographic results. We still do not know whether such guidelines are adequate in improving the outcomes of preterm infants especially associated with hsPDA.
The aim of this study was to assess whether there are any differences in the mortality and the in-hospital outcomes of preterm infants with a gestational age (GA) < 28 weeks who received ibuprofen treatment according to the presence of clinical symptoms attributable to the hsPDA at the time of first ibuprofen treatment. We also assessed the association between the echocardiographic and radiographic findings and the clinical symptoms due to hsPDA. And we assessed whether there was any difference in the pharmacologic characteristics of the ibuprofen treatment according to the presence of clinical symptoms attributable to the hsPDA.
MATERIALS AND METHODS
Study design
A retrospective study was done with 98 preterm infants < 28 weeks of gestation who were born and admitted to the neonatal intensive care unit of the Seoul National University Children’s Hospital between April 2010 and March 2015 and received ibuprofen for the treatment of hsPDA. Clinical and demographic data were collected from the reviewed medical records of the enrolled patients. Three infants were excluded because of a major congenital anomaly or the absence of echocardiographic data or information about the PDA treatment. We also excluded the infants with pulmonary hemorrhage, IVH ≥ grade 3, or NEC ≥ stage 2b before ibuprofen treatment because these morbidities are relative contra-indications for ibuprofen treatment. Finally, a total of 91 preterm infants were included in the analysis (Fig. 1).
Fig. 1
Flow chart of the study population. A total of 91 infants with < 28 weeks of gestation born between April 2010 and March 2015 with hemodynamically-significant patent ductus arteriosus (hsPDA) receiving ibuprofen treatment were included in the analysis. Infants with hsPDA without clinical symptoms were 77 infants (84.6%) and infants with hsPDA with clinical symptoms were 14 infants (15.4%) at the time of first ibuprofen treatment.
PDA = patent ductus arteriosus.

If there is any suspect of cardiomegaly or pulmonary edema on chest radiograph, or respiratory difficulty, hypotension, decreased urine output or metabolic acidosis suggesting hsPDA, we checked the echocardiography for the confirmation of hsPDA. Before the ibuprofen treatment, all infants underwent an echocardiography to check for the presence of congenital heart defects and to evaluate the PDA status by a pediatric cardiologist. All infants received intravenous or oral ibuprofen at an initial dose of 10 mg/kg, followed by two doses of 5 mg/kg each after 24 and 48 hours. An oral route was preferred when feeding was started and there was no feeding intolerance. The patient was assessed clinically and echocardiographically at 24–48 hours after the third dose, and if the hsPDA persisted without any contraindications of ibuprofen treatment, a second and, if necessary, a third course of ibuprofen treatment was administered. If there were still significant respiratory difficulty, hypotension, or oliguria without closure of hsPDA by ibuprofen treatment, secondary PDA ligation was done.
We categorized the entire study population into two groups according to the presence of clinical symptoms attributable to the PDA at the time of first ibuprofen treatment. Then, we compared the baseline demographic characteristics prior to ibuprofen treatment including the GA at birth, birthweight, year of birth, gender, cesarean section, multiple pregnancy, complete course of antenatal steroid use, small for gestational age (SGA), clinical risk index for babies (CRIB)-II score (14), Apgar score at 5 minutes, presence of delivery room (DR) resuscitation, histologic chorioamnionitis, pregnancy induced hypertension (PIH), sepsis and inhaled nitric oxide use prior to treatment between the two groups. We examined the differences in echocardiographic findings just before the ibuprofen treatment including the transductal diameter per kilogram, left atrial/aortic root (LA/Ao) ratio and left ventricular end-diastolic dimension (LVDD) ratio, and the radiographic findings including cardiomegaly and pulmonary edema on the chest radiograph. The differences in the pharmacologic treatment characteristics including the first day of ibuprofen treatment, route of medication and numbers of ibuprofen treatment courses were also assessed. Lastly, the mortality and in-hospital outcomes after ibuprofen treatment were compared between the two groups.
Definitions
hsPDA was defined as a PDA with a transductal diameter ≥ 1.4 mm/kg with significant left to right shunt confirmed by echocardiography considering the previous studies by Kluckow and Evans (11) and McNamara and Sehgal (12). Presence of clinical symptoms due to hsPDA was defined as at least one of the 3 following clinical symptoms besides echocardiographic confirmation compatible with the hsPDA:oliguria ≤ 1mL/kg/hr in the preceding 8 hours before ibuprofen treatment, hypotension caused by PDA requiring inotropics more than 10 µg/kg/min or respiratory difficulty requiring invasive mechanical ventilator care. Respiratory difficulty was defined as having at least two of the following findings in infants with conventional ventilator care; FiO2 > 0.5, respiratory rate > 40/min, and peak inspiratory pressure > 20 cmH2Oto maintain oxygen saturation between 88% and 95%, and a PaCO2 < 65 mmHg. In infants with high frequency ventilator care, a mean airway pressure >13 mmHg and a FiO2 > 0.5 were required to define respiratory difficulty as the previous report (15).
First day of echocardiography was defined as the difference between the date of the first echocardiography examination and the date of birth. Zero day in the data meant the echocardiogram was done less than 24 hours after birth. First day of ibuprofen administration was determined from the difference between the date of first ibuprofen use and the date of birth. Cardiomegaly on the chest radiograph was defined as a cardiothoracic ratio of more than 0.6. The definition of SGA was according to the definition published by Olsen et al. (16). PIH was defined as any maternal diagnosis of eclampsia or preeclampsia. DR resuscitation was defined as cardiac compression or administration of medication in the DR. Invasive ventilator care ≤ 2 days after birth was defined as any ventilator support via endotracheal tube ≤ 2 days after birth. Hypotension before treatment was defined as hypotension with any inotropic or hydrocortisone use before ibuprofen treatment. Sepsis was defined as the presence of a causative organism documented from the blood culture. PDA closure rate was defined as the rate of PDA closure confirmed by echocardiography after ibuprofen treatment or secondary ligation. Secondary ligation was defined when infants received PDA ligation after failure to close the PDA with ibuprofen treatment. The postnatal day of PDA closure was defined as the first postnatal day of PDA closure confirmed by echocardiography in patients treated with only ibuprofen administration or the postnatal day of PDA ligation in infants receiving secondary ligation. We defined the duration of invasive ventilator care as the duration of ventilator support via endotracheal tube, and we also defined the duration of respiratory support as the whole duration of any ventilator or oxygen support during hospitalization.
Statistical analysis
All the continuous variables are expressed as the median (range), and the categorical variables are expressed as numbers and proportions. For univariate analysis, continuous variables were compared using the Mann-Whitney U test, and categorical variables were compared using the χ2 or fisher’s exact test. Univariate analyses were done for the mortality, secondary PDA ligation, and in-hospital outcomes associated with prematurity including NEC ≥ stage 2b, spontaneous intestinal perforation (SIP), duration of respiratory support, duration of invasive ventilator care, hospital stay (days), moderate to severe BPD and severe BPD only. To assess the independent association between the presence of clinical symptoms due to hsPDA at the time of the first ibuprofen treatment and the primary outcomes (mortality ≥ 3 postnatal days, secondary PDA ligation and composite outcome including mortality ≥ 3 postnatal days, NEC ≥ stage 2b of modified Bell’s criteria [17], severe BPD at 36 weeks of gestation (18), and IVH ≥ grade 3 of Papile’s classification [19]) and secondary outcomes (NEC ≥ stage 2 or death, BPD or death, severe BPD or death, and IVH ≥ grade 3 or death), binary logistic regression analysis was done adjusting for the CRIB-II score, birthweight, the year of birth, and the invasive ventilator care ≤ 2 postnatal days. The statistical analysis was done with IBM SPSS Statistics version 20 (IBM Corp., Amarok, NY, USA) and R version 3.1.2. (http://www.r-project.org). P values less than 0.05 were considered statistically significant.
RESULTS
A total of 91 infants were included in our analysis. Seventy-seven infants (84.6%) received ibuprofen treatment for hsPDA without clinical symptoms at the time of first ibuprofen treatment and 14 infants (15.4%) were treated with clinical symptoms attributable to the hsPDA.
Baseline and demographic characteristics
Infants treated with ibuprofen in the presence of clinical symptoms due to hsPDA (clinical symptoms group) were younger and lighter at birth with higher CRIB-II scores compared to the infants without clinical symptoms due to hsPDA at the time of first ibuprofen treatment (no clinical symptoms group). Those infants who were born after 2013 tended to be more in the clinical symptoms group. More infants received invasive ventilator care within 2 postnatal days in the clinical symptoms group (Table 1).
Table 1
Demographic and baseline characteristics of the study population
Echocardiographic and radiographic characteristics
There was no statistically significant difference in the first day echocardiography between two groups (1 [0–7] day in no clinical symptoms group vs. 1 [0–3] day in the clinical symptoms group; P value = 0.803). Among the echocardiographic parameters at the time of first ibuprofen treatment, only the transductal diameter/kg was larger in the clinical symptoms group compared to the no clinical symptoms group. There was no difference in cardiomegaly or pulmonary edema on the chest radiograph between the two groups (Table 2). In the clinical symptoms group, 5 infants (35.7%) had both cardiomegaly and pulmonary edema on the chest radiograph; however, 7 infants (50.0%), had neither cardiomegaly nor pulmonary edema even though there were clinical symptoms due to hsPDA.
Table 2
Echocardiographic and radiographic characteristics of the study population
Pharmacologic characteristics of ibuprofen treatment
There was no significant difference in the median postnatal day of the first course of ibuprofen therapy in both groups. More infants received multiple courses of ibuprofen in the clinical symptoms group compared with the no clinical symptoms group (Table 3).
Table 3
Pharmacological characteristics of ibuprofen treatment in the study population
Mortality and in-hospital outcomes
PDA closure was confirmed in 86 (94.5%) infants in our study population. There were no statistically significant differences in the PDA closure rate and the postnatal day of PDA closure between the two groups (13 [3–89] days in the no clinical symptoms group vs. 18 [3–41] days in the clinical symptoms group; P = 0.837). Thirty-four infants (37.4%) received secondary PDA ligation after failure of PDA closure by ibuprofen use. The frequency of secondary PDA ligation was higher in the clinical symptoms group compared with the no clinical symptoms group in the univariate analysis (Table 4).
Table 4
In-hospital outcomes according to the presence of clinical symptoms due to PDA at the time of ibuprofen treatment
PDA = patent ductus arteriosus, hsPDA = hemodynamically-significant PDA, NEC = necrotizing enterocolitis, SIP = spontaneous intestinal perforation, IVH = intraventricular hemorrhage, PVL = periventricular leukomalacia, BPD = bronchopulmonary dysplasia, ROP = retinopathy of prematurity, VEGF = vascular endothelial growth factor.
Three infants died after PDA closure confirmed by echocardiography. One infant died by multi-organ failure due to NEC 3b, and the other 2 infants died because of sepsis from methicillin-resistant Staphylococcus aureus and imipenem-resistant Acinetobacter baumannii in each case, respectively. In the univariate analysis, there were no significant differences in the mortality; however, the total duration of hospitalization, invasive ventilator care, and total respiratory support were all longer, and BPD was more frequent in the clinical symptoms group compared with the no clinical symptoms group (Table 4).
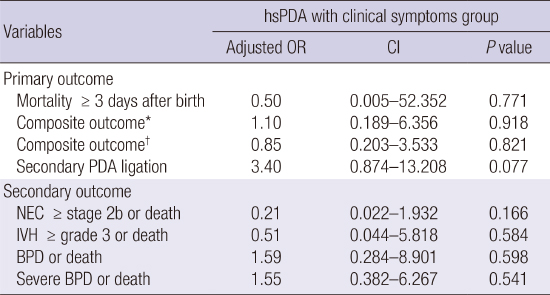
After multivariate analysis adjusting for the CRIB-II score, birthweight, the year of birth, and the invasive ventilator care ≤ 2 postnatal days, there were no significant differences in mortality, secondary PDA ligation and in-hospital outcomes between the clinical symptoms group and the no clinical symptoms group (Table 5).
Table 5
Multivariate analysis of mortality and in-hospital outcomes according to the presence of clinical symptoms at the time of ibuprofen treatment (reference: hsPDA without clinical symptoms group)

Adjusted for the CRIB-II score, the year of birth, birthweight, invasive ventilator care ≤ 2 days after birth.
hsPDA = hemodynamically-significant patent ductus arteriosus, OR = odds ratio, CI = confidence interval, PDA = patent ductus arteriosus, NEC = necrotizing enterocolitis, IVH = intraventricular hemorrhage, BPD = bronchopulmonary dysplasia.
*Mortality ≥ 3 days after birth, NEC, IVH, BPD; †Mortality ≥ 3 days after birth, NEC, IVH, severe BPD.
DISCUSSION
In our study, infants who received first ibuprofen treatment when there were clinical symptoms attributable to hsPDA were younger with higher CRIB-II scores than infants with first ibuprofen treatment done with no clinical symptoms due to hsPDA. More infants received multiple courses of ibuprofen treatment who received first ibuprofen treatment when there were clinical symptoms attributable to hsPDA; however, there were no significant differences in the mortality and in-hospital outcomes between the two groups.
All the patent ductus are not pathologic. In some cases, the patent ductus may be an “innocent physiologic bystander” with little hemodynamic consequences; however, in other cases, it may contribute to significant pathologic changes for which early detection and intervention are warranted to prevent neonatal morbidities (420). We usually define hsPDA as PDA with a left-to-right shunt from the aorta into the pulmonary arteries which causes pulmonary vascular and left ventricular volume overload. However, there is no consensus on the definition of hsPDA (921). The lack of a standardized approach in determining the hemodynamic significance is a major barrier in searching for an association between persistent ductus arteriosus and the major morbidities of preterm infants or in assessing the benefit of PDA treatment (8). Before the PDA staging system was proposed by McNamara and Seghal (12), a transductal diameter more than 1.5 mm was proposed as a significant factor implying end-organ hypoperfusion reported by Kluckow and Evans (11). McNamara and Sehgal (1222) proposed the staging of PDA for determining the severity of hsPDA, which was based on the clinical and echocardiographic criteria. Echocardiographic staging includes E1 (no evidence of ductal flow), E2 (small non-significant ductus arteriosus), E3 (moderate hsPDA), and E4 (large hsPDA). Clinical staging includes C1 (asymptomatic), C2 (mild), C3 (moderate), and C4 (severe) based on illness severity and the magnitude of the cardiovascular, respiratory, and gastrointestinal problems.
Our unit adapted the definitions for hsPDA according to the suggestions of Kluckow and Evans (11) and Mcnamara and Sehgal (1222) if PDA with a transductal diameter ≥ 1.4 mm/kg with a significant left to right shunt was confirmed by the echocardiography. Because our study was a retrospective study, we could not get the whole echocardiographic parameters such as ductal flow pattern, early passive to late atrial contractile phase of transmitral filling ratio, and isovolumic relaxation time. Thus, we could not define the hsPDA entirely dependent on the Mcnamara staging based on echocardiographic criteria. For the definition of clinical symptoms due to hsPDA, our definition of clinical symptoms was close to C3 or C4 of clinical staging by McNamara and Seghal (1222). When we tried to classify our study population according to the McNamara’s clinical staging, it was difficult to judge which group is suitable for each baby because some parameter fitted one stage, however, other parameters fitted another. Especially about C2 and C3 group, most infants were in the gray zone between C2 and C3 group, so we decided to adapt another guideline to define clinical symptoms due to PDA according to the Sosenko et al. (15). We did not include infants with mild respiratory symptoms in the clinical symptoms group because mild respiratory symptoms can be due to other causes such as respiratory distress syndrome, sepsis or “evolving” BPD.
There have been many reports suggesting a correlation between the increase of the plasma BNP level and the echocardiographic parameter suggesting hsPDA or symptomatic PDA (1023). Choi et al. (24) suggested that the BNP levels correlated well with the magnitude of the ductal shunt, and the BNP levels were higher in the symptomatic PDA group when compared with the asymptomatic PDA group. Other researchers suggested that the early BNP level was significantly correlated with the magnitude of the ductal shunt and can help to predict hsPDA (2526). Because we could get the BNP level in only 14 infants among the study population (data are not shown), we could not examine such a correlation between the BNP level and other echocardiographic or radiographic parameters or the association between the severity of the clinical symptoms and the BNP level. Further studies are needed focusing on the association between the BNP level and hsPDA.
In our study, only the transductal diameter was a significant echocardiographic parameter which can predict the presence of clinical symptoms due to hsPDA. However, when we assessed the correlation between the findings of the radiography and the clinical symptoms, there was no significant association in our study. Because the size of the thymus of a neonate is relatively big and chest radiography is usually done as an anteroposterior view, we could not obtain exact information about cardiomegaly, and echocardiographic measurement can be a better method to judge cardiomegaly. There are several studies on significant echocardiographic parameters as an early marker of hsPDA because echocardiographic signs usually have been shown to precede clinical symptoms by 1.8 days (27). Some researchers have suggested that a transductal diameter exceeding 1.5 mm combined with diastolic flow reversal in the descending aorta may be the best echocardiographic criterion (28). Others have stated that a substantial ductal shunt is associated with the following: an increased ratio of left atrial to aortic root dimensions ≥ 1.5:1, a ductal diameter ≥ 1.5 mm, a measured LVDD ratio by the normal LVDD ratio of more than 115% (29), left ventricular volume and pressure overloading, and reversal of diastolic flow in the descending aorta or in the cerebral or renal arteries (1230). About left ventricular volume and pressure overloading, an increased LVDD ratio (measured LVDD divided by the normal LVDD as an index) > 115% was a useful index of PDA treatment (29). However, in isolation, many of these markers have low sensitivity and specificity for ductal significance when compared to the transductal diameter (11). Therefore, a study on the combination of clinical and echocardiographic markers is needed for better decision making about PDA treatment.
There still is no consensus on which PDAs we have to treat, when to treat, and how to treat. There is a high chance of spontaneous closure of preterm PDA, especially in infants with higher GA (2128). Moreover, there is some evidence that preterm infants with mild symptoms from PDA do not necessarily benefit from early pharmacologic treatment compared with conservative treatment (1531). Additionally, there are potential risks associated with pharmacologic treatment, such as impaired renal function, intestinal perforation, NEC and increase of bleeding tendency. Many studies on surgical ligation have reported adverse outcomes such as increased BPD in association with surgical ligation (32). The timing of PDA ligation is also important for determining the neonatal outcomes (33). Thus, targeted treatment is important to reduce such adverse effects, and knowing early markers of hsPDA that indicate the need for treatment will be beneficial.
In our study population, the infants in the clinical symptoms group were younger and the CRIB-II score was higher; and after adjusting for such differences in the baseline characteristics, there were no significant differences in the mortality and in-hospital outcomes between the two groups. Although more infants received repeated courses of ibuprofen treatment in the clinical symptoms group, there were no significant differences in the PDA closure rate and in the duration of PDA opening. Previous studies have suggested that ductal ligation causes an abrupt change in the hemodynamics of preterm infants, thereby leading to adverse neonatal outcomes (34). Recently, Lemmers et al. (35) performed near infrared spectroscopy-monitored cerebral oxygen saturation (rSco2) and brain MRI at term equivalent age and assessed the regional brain volume and maturation of the posterior limb of the internal capsule in an indomethacin group, PDA ligation group, and matched control groups without PDA. PDA led to lower cerebral oxygenation, and the PDA ligation group had the lowest rSco2 values, the highest postnatal age before effective treatment, and the lowest volumes of most brain regions, especially the cerebellum. We can infer that the longer period of suboptimal cerebral oxygenation in the PDA ligation group, not the surgical procedure itself, could be a reason for the negative effect of PDA on brain growth. We can also guess that current practice to postpone medical or surgical ductal closure may cause negative effects on brain growth. In our study, the frequency of secondary PDA ligation was somewhat higher in the clinical symptoms group with marginal statistical significance after multivariate analysis; however, it did not affect the mortality and the frequency of BPD. And there was no difference in the postnatal day of PDA closure between two groups. Our data favor the selected treatment of clinically symptomatic PDA without adverse clinical outcomes.
In our study, there were no significant differences in mortality or neonatal outcomes between prophylactic or pre-symptomatic treatment and symptomatic treatment. Although the meta-analysis suggests that prophylactic indomethacin treatment can reduce the frequency of IVH and reduce later PDA treatment and PDA ligation, there was no significant difference in mortality or long-term neurodevelopmental outcomes (36). Yeo et al. (37) reported that prophylactic ibuprofen treatment in preterm infants could not reduce PDA ligation and the incidence of IVH. Concerning pre-symptomatic treatment, there are some reports which compared the mortality and neonatal outcomes between early and conventional treatment groups. Van Overmeire et al. (38) reported that early treatment at postnatal day 3 was associated with more renal side effects without any advantage in respiratory or major outcomes. Candel-Pau et al. (39) performed routine echocardiography within 48 hours after birth in infants < 29 weeks of gestation, and if the PDA diameter/weight ≥ 1.4 mm/kg and/or the LA/Ao ratio ≥ 1.4, indomethacin treatment was done. However, when they compared the frequency of secondary ligation, mortality and major preterm morbidities between such an early treatment group and the conventional treatment group, there were no significant differences like our study results.
Our study has some limitations. First, this is a retrospective study with a small number of patients in a single center. Thus, the factors with marginal statistical significance like secondary PDA ligation should be reassessed with a large cohort. Actually, ibuprofen was recently accepted as a treatment modality of preterm PDA and we included all the infants with ibuprofen treatment after intravenous type of ibuprofen became available in Korea. So, although the power level of our study did not reach 0.80, the results of our study are meaningful as a suggestion on the needs of future prospective, multi-center study. Second, we only included the preterm infants with ibuprofen treatment and the treatment policy changed from 2013. Moreover, we could not assess the outcome of infants with conservative management for preterm PDA which is an increasing treatment policy for preterm PDA after the year 2013. Although we tried to adjust such bias by year factor in multiple regression analysis in this study, further studies are needed focusing on the association between conservative treatment of preterm PDA and neonatal outcomes. Third, the definition of clinical symptoms from hsPDA was somewhat different from the clinical staging of preterm PDA by McNamara and Sehgal (1222). If we could classify the group according to their clinical staging, we could assess the relationship between the severity of the clinical symptoms and the neonatal outcomes in preterm infants, so further studies are needed.
In our study, about 15% of the infants with ibuprofen treatment received treatment in situations for which the clinical symptoms were attributable to the hsPDA. Younger infants tended to receive first ibuprofen treatment when there were clinical symptoms due to hsPDA. Although more infants received multiple courses of ibuprofen treatment in the clinical symptoms group, there were no differences in the mortality and in-hospital outcomes between the infants with clinical symptoms due to hsPDA and the infants without clinical symptoms. We can hold off on PDA treatment until the clinical symptoms becomes prominent. However, because our study was a retrospective, single center study with small number of study objects, a prospective, multicenter, large cohort study is needed in the near future.
 XML Download
XML Download