

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Functional abdominal pain (FAP) is one of the most common gastrointestinal complaints in children (1). FAP reduces the quality of everyday life, and leads to school absences and frequent visits to the doctor, which cause considerable distress to children and their families (23).
The prevalence of FAP is approximately 8%–10% in the pediatric population (45). Despite the high prevalence of FAP, its pathophysiology is currently unclear. Knowledge regarding FAP has improved over the past several decades, along with the identification of causative factors, diagnostic methods, and management of FAP in children (2). However, the management of FAP remains challenging for physicians.
Constipation is another common complaint in children, and may be one of the major causes of FAP (67). Because of the absence of a specific marker for diagnosis, the identification of constipation is mainly based on self-reported symptoms. The Rome III diagnostic criteria, published in 2006, are considered the gold standard for identifying functional constipation. Although various functional gastrointestinal disorders (FGID) have been defined separately using Rome III criteria, some of the associated pathophysiology and clinical symptoms are shared by FGID. It has also been suggested that constipation and other diseases classified as FGID are not separate disorders, but instead may represent various forms of a single disease (8). Previous studies reported that FGID has a common underlying interaction of psychosocial factors and altered gut physiology (910). For these reasons, it is often difficult to clinically diagnose a patient with constipation based on the Rome III criteria (81112).
In clinical practice, FAP patients or their caregivers may express concern about irregular prolonged duration of defecation. When asked about stool cohesion or form, or pain during defecation, a large proportion described symptoms suggestive of constipation or fecal retention. However, they often tend to disagree when asked directly whether they (or their child) have constipation. In a previous study, occult constipation (OC) was defined as a clinical condition with no complaint of constipation on initial medical history-taking and no symptoms indicating constipation, but at least one of the following signs: 1) hard consistency of stool (rock- or pellet-like) on rectal examination, and 2) evidence of large intestine distended by fecal material on plain abdominal radiography. Fecal retention was therefore proposed as a cause of recurrent abdominal pain in children (5).
Several authors have described pharmacologic treatments for FAP in children (1314). Although some have suggested laxatives (7131516), evidence of efficacy is limited. Furthermore, there are few studies assessing the prevalence of OC among patients with FAP (715).
Therefore, the first objective of this study was to investigate the prevalence of OC in those with FAP. The second objective was to determine which medications (i.e., laxatives or prokinetic drugs) are more useful in children with FAP and OC diagnosed by plain abdominal radiography and Leech scores.
MATERIALS AND METHODS
Study participants and randomization
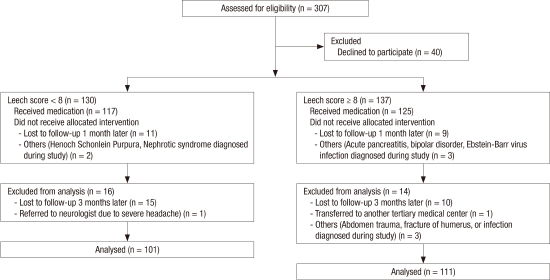
This study was performed prospectively between January 1, 2013 and December 31, 2013. We enrolled pediatric outpatients with abdominal pain who visited CHA Bundang Medical Center in Korea. Eligible participants included 307 children aged 4–15 years who met the Rome III criteria for FAP (8); 40 patients declined to participate and were excluded. Patients diagnosed with organic diseases after work-up were also excluded. Plain abdominal radiographs were obtained from all patients, and the amount of fecal retention was graded based on the Leech score.
For analysis, the enrolled patients were divided into 2 diagnostic groups according to Leech scores: 1) those with a Leech score < 8 were defined as group 1, and 2) those with a Leech score ≥ 8 were defined as group 2. OC was diagnosed in patients in group 2 whose clinical status satisfied the definition of OC as described in the Introduction (1517). Group 1 patients were only treated with prokinetic drugs. Group 2 patients received either prokinetic drugs or laxatives. Patients received lactulose (Duphalac®, 1–2 mL/kg/day; Choong Wae Pharma Corp., Seoul, Korea) or polyethylene glycol 3350/4000 (Forlax powder®, 1–1.5 mg/kg/day; Ahngook Pharmaceutical Co., Ltd., Seoul, Korea) for laxative treatment, and domperidone (Motilium-M tab®, 1–2 mg/kg/day; Janssen Korea Ltd., Seoul, Korea) for prokinetic drug treatment. Patients were randomly allocated to receive either medication by their hospital registration numbers after evaluation of their Leech score. Due to the nature of our study, the patients (or their parents) were not blinded to which medication they received.
We assessed the responses after follow-up at 2 weeks, 1 month, and 3 months by interviewing patients at the outpatient clinic. All children were interviewed by a gastroenterologist about complaints, signs, and symptoms of FAP, and the same physician evaluated the Leech score of enrolled patients and prescribed medications (Fig. 1).
Fig. 1
Flow diagram of patient classification.
FAP = functional abdominal pain, OC = occult constipation.

None of the patients included in this study fulfilled the Rome III criteria for functional dyspepsia, irritable bowel syndrome, or abdominal migraine (8). Those who received antibiotics, probiotics, or any other drugs that might affect gastrointestinal motility throughout the study period were excluded. Patients who were unable to revisit the clinic during the 3 follow-up periods were also excluded.
Measurement of outcomes
Improvement of symptoms was defined when abdominal pain decreased by more than half in frequency or severity. The Faces Pain Scale-Revised (FPS-R) was also used to measure pain intensity. The FPS-R consists of 6 facial expressions for the degree of pain, ranging from no pain (scored 0) to severe pain (scored 5). Children were asked to choose the facial expression that best described the pain they felt at the time of the interview. We defined therapeutic response as a score reduction of ≥ 2 points (18).
Statistical analysis
Statistical analysis was performed using SPSS, version 21.0 (IBM Corp., Armonk, NY, USA). A χ2 test was performed for between-group comparisons. Linear logistic regression analysis was performed to investigate whether symptom relief could be predicted by sex, age, medication, or Leech scores. A P value < 0.05 was considered statistically significant.
Results
Patient baseline characteristics
The mean age of the patients enrolled (n = 212) was 7.9 ± 2.9 years. No differences in sex were observed. Approximately 47.6% (n = 101/212) and 52.4% (n = 111/212) of patients were classified as groups 1 or 2, respectively. The prevalence of OC in patients with FAP was 52.4% (n = 111/212) in our study.
Of the 212 patients who were treated, a therapeutic response was observed in 121 (57.1%) at 2 weeks, 129 (60.8%) at 1 month, and 116 (55.5%) at 3 months.
Comparison of the therapeutic response between groups
The response rates in group 1, treated with only prokinetic drugs, were 52.5% (53/101) after 2 weeks, 54.5% (55/101) after 1 month, and 45.5% (46/101) after 3 months (Table 1). The therapeutic response rates after 2 weeks, 1 month, and 3 months in group 2, treated with either prokinetic drugs or laxatives, were 61.3% (68/111), 66.7% (74/111), and 63.1% (70/111), respectively (P = 0.472, P = 0.674, and P = 0.740). There were no statistically significant differences between group 1 and 2.
Response rate to prokinetic drugs by the Leech score
During the study period, 159 patients with FAP (group 1, n = 101; group 2, n = 58) were assigned to treatment with prokinetic drugs and completed the 3-month follow-up. The response rates for patients in groups 1 and 2 treated with prokinetic drugs were 52.5% vs. 46.6% after 2 weeks (P = 0.290), 53.5% vs. 50.0% after 1 month (P = 0.399), and 45.5% vs. 48.3% after 3 months (P = 0.433), but were statistically insignificant.
Response rate by medications (prokinetic drugs vs. laxatives) in group 2
Of the 111 group 2 patients, 58 and 53 were allocated to receive either prokinetic drugs or laxatives, respectively. There was no difference in the demographic data, including Leech scores, between those who were treated with prokinetic drugs and laxatives in group 2 (Table 2).
Table 2
Demographic and baseline characteristics of group 2
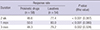
After 2 weeks, symptomatic resolution was achieved in 46.6% (27/58) and 77.4% (41/53) of patients treated with prokinetic drugs or laxatives, respectively (P < 0.001). The therapeutic response rates in those treated with prokinetic drugs and laxatives were 50.0% and 83.0% after 1 month (P < 0.001) and 48.3% and 79.2% after 3 months (P < 0.001), respectively (Table 3).
Table 3
Response rate by medication (prokinetic drugs vs. laxative) in group 2
| Duration | Response rate | P value (Rho value) | |
|---|---|---|---|
| Prokinetic drugs (n = 58) | Laxatives (n = 54) | ||
| 2 wk | 46.6 | 77.4 | < 0.001 (0.387) |
| 1 mon | 50.0 | 83.0 | < 0.001 (0.380) |
| 3 mon | 48.3 | 79.2 | 0.002 (0.328) |
Adverse effects including diarrhea or stool soiling were not reported by any of the children who had laxatives prescribed, and no neurological symptoms were reported in those prescribed prokinetic drugs.
Response rate in group 2 by Leech score
Among 30 patients with a Leech score of 8, 23.5% (4/17) and 53.8% (7/13) treated with prokinetic drugs or laxatives, respectively, reported an improvement in symptoms after 2 weeks. An improvement in symptoms after 1 month and 3 months was achieved in 47.1% and 52.9% of patients treated with prokinetic drugs, and in 69.2% and 53.8% of patients treated with laxatives, respectively. Among 37 patients with a Leech score of 9, 20, and 17 patients were treated with prokinetic drugs or laxatives, respectively. An improvement in symptoms was observed in 45.0% (9/20), 40.0% (8/20), and 50.0% (10/20) of patients treated with prokinetic drugs, and 82.4% (14/17), 82.4% (14/17), and 76.5% (13/17) of patients treated with laxatives at 2 weeks, 1 month, and 3 months, respectively.
In all treatment periods (i.e., 2 weeks, 1 month, and 3 months), patients who were treated with laxatives had a better therapeutic response than those treated with prokinetic drugs; however, the sample size of patients with Leech scores of 11, 12, 13, and 14 was relatively small. With increasing Leech scores, the differences in treatment responses between those treated with laxatives or prokinetic drugs became larger.
In group 2 patients who received laxatives, the therapeutic response was significantly improved (odds ratio [OR], 2.615; 95% confidence interval [CI], 1.135–6.026; P = 0.024). However, in patients who received prokinetic drugs, improvement in Leech score was not statistically significant (OR, 0.778; 95% CI, 0.516–1.172; P = 0.230) (Table 4).

DISCUSSION
Plain abdominal radiography is a cost-effective, noninvasive, and reliable tool used to quantify stool impaction (17). Previous studies concluded that plain abdominal radiography is useful for characterizing fecal impaction and assessing therapeutic response (1920). There are 3 different scoring systems that quantify fecal retention on plain abdominal radiography; of these, the Leech score was reported to be the most clinically useful for estimating fecal load on plain abdominal radiographs in children (21). Therefore, the Leech scoring system was used to analyze plain abdominal radiographs and categorize the patients in this study.
The association between OC and FAP has been reported in various studies (5715). Approximately 52.4% of all patients with FAP and a Leech score ≥ 8 were presumed to have OC in this study. Not all patients with FAP have OC, but the number of patients with FAP and OC was higher than we expected. Our results correspond to previous studies in which the proportion of patients with FAP and OC was reported to be 42.6%–46.0% (515).
A comprehensive diagnostic strategy coupled with a stepwise therapeutic approach proved effective in reducing FAP (22). One study reported 27% and 70% of patients showed spontaneous relief or improvement with therapy, respectively, after 6 months of follow-up. However, 30% of children still had persistent symptoms of FAP after a follow-up of 5 years (323). There are various approaches for managing FAP, including reassurance, maintaining a symptom diary, and psychological therapy. However, primary management is limited in many cases (24). Pharmacotherapy is frequently used for FAP. Prokinetic drugs are reported to decrease abdominal symptoms and are considered safe in children (252627). Acid-suppressing drugs, such as histamine-receptor antagonists, proton-pump inhibitors, antispasmodic drugs, analgesics, and probiotics, are commonly used. In a previous study, among patients who fulfilled the Rome criteria for functional gastrointestinal pain syndromes, those who appeared to be pain-free with laxatives were defined to have OC, and the prevalence of OC in children with FAP who were successfully treated with laxatives was 46% (15).
There was no significant difference in the FPS-R scores between groups in those treated with prokinetic drugs during the study period. Among patients with a Leech score ≥ 8 and FAP, laxatives were more effective than prokinetic drugs in relieving symptoms. In FGID, hypersensitivity to rectal or sigmoid balloon distention can be observed in 50%–70% of patients (28). Fecal retention in the colon with subsequent bowel distension may explain why treatment with laxatives was effective in patients with FAP. Our findings are supported by previous studies in which laxatives were found to be more effective in children with FAP, high Leech scores, and severe fecal retention (829). The therapeutic response of the patients included in our study slightly decreased at the follow-up after 3 months compared to that after 1 month. This might result from the fact that parental reactions and compliance by the participants were relatively higher at the beginning of medical treatment.
The strength of our study lies in the approach used to reveal the relationship between childhood FAP and OC. Many patients with FAP did not fulfill the Rome III criteria for constipation, but had a high Leech score based on plain abdominal radiographic findings. Therefore, estimating the amount of fecal retention may be considered an important step in selecting treatment for patients with FAP. We also attempted to compare the effectiveness of laxatives vs. prokinetic drugs in patients with FAP with OC; laxatives were more effective in reducing symptoms compared to prokinetic drugs in children with OC, suggesting that fecal disimpaction using laxatives was effective for relieving abdominal pain in patients with a Leech score ≥ 8.
There are some limitations. This study was conducted in a single tertiary-care hospital setting; therefore, it is difficult to generalize our results to the entire pediatric population. Furthermore, long-term follow-up was not achieved, and the response rate was limited by the 3-month follow-up. Second, placebo effects cannot be excluded due to the absence of controls. Therefore, a larger, double-blind investigation is warranted. Moreover, we used the FPS-R, which is a clinically valuable instrument, in order to measure therapeutic responses. However, there is a possibility that the responses reported by patients or caregivers using the FPS-R were misestimated.
In conclusion, we found that the prevalence of OC among patients with FAP was 52.4%, which is higher than expected. More than half of the patients diagnosed with FAP had OC, suggesting a close relationship. Laxatives were found to be more effective than prokinetic drugs for relieving symptoms of FAP in children with a Leech score ≥ 8.
 XML Download
XML Download