

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The development of clinical radiation oncology means enhancing knowledge of the total radiation doses, fractional doses, and biological effective doses that are the most suitable for removal of certain tumors based on long experience in cancer patient radiotherapy (RT) at clinics. Many clinical articles and a deepening of the knowledge of macroscopic and functional damage to normal organs around tumors occurring in the areas of clinical RT doses have also contributed to the development of this field. This accumulation of knowledge of clinical radiation oncology per se plays an important role in effectively treating cancer while minimizing side effects.
However, even if necessary doses for tumor control and effects on surrounding normal organs were sufficiently understood, the administration of accurate prescribed radiation doses to tumors can be said to have been impossible without support by the development of physics, computers, and machine engineering. For instance, if radiation is prescribed to be generated at a point 100 cm away from the tumor in the body, it first has to pass through approximately 85 cm of air, then the skin of the chest, the hard ribs, and the lung tissues containing large amounts of air. Then, it has to be precisely focused to irradiate metastatic tumors in the lymph nodes in front of the thoracic vertebrae behind the heart at a dose of 1.80 Gy. Due to technological advances, modern medicine can accurately implement this prescription.
The radiation dose prescribed by the physician can be delivered to an accurate point because the target in the body can be accurately aimed at using cutting-edge treatment equipment. The radiation dose can be precisely predicted through high performance computer calculations based on the patient’s computed tomography images. We can say that the development of computer and machine engineering is most acutely applied to the treatment of human diseases in the area of clinical cancer RT. In addition, the development of cutting-edge imaging technologies has overcome the limitations of cancer RT in the past, when the treatment relied on two-dimensional images. These new technologies enable physicians to see more clearly, delineate shapes or outlines that were unclearly identified in the past, provide three-dimensional shapes or location information of tumors, and can be fused to planned dose distributions for RT with magnetic resonance images at the same locations and coordinates.
Deepened understanding through biological studies on the effects of radiation on human bodies helps reduce radiation doses for tumor control through the development of radiation sensitizers that increase tumors’ responses to irradiation. Preclinical small animal based transitional studies and molecular biological studies of the effects of radiation on normal tissues around tumors or damage to the tissues assist in minimizing the side effects of RT to maximize patients’ quality of life.
In addition, the development of medical physical quality assurance (QA) techniques and programs is playing essential and pivotal roles in the identification, maintenance, and management of accurate and precise RT for cancer patients as well as for RT workers’ safety while delivering high-dose radiation for tumor treatment to many patients every day. Clinical RT for tumors can continue to develop based on these safety devices. This process of development is quickly becoming a base for achieving the ‘optimization’ of medical use of radiation. This issue concretely describes the changes in individual elements during the development of RT to minimize the effects of radiation on normal tissues.
DEVELOPMENT OF CLINICAL RADIATION ONCOLOGY AND ITS EFFECTS ON NORMAL TISSUES AROUND TUMORS
Although the full story of the development of radiation oncology should include the development of all of computer and machine engineering, cutting-edge imaging technology, studies of the effects of radiation on human bodies, and medical physical quality assurance programs in a broad sense, in this section, the development of clinical radiation oncology in the narrow sense, limited to the development of radiation oncology in the clinical field and the macroscopic and functional effects of that development on normal tissues will be addressed.
First, the clinical experience and knowledge in the field of clinical RT that have been gradually accumulated over time led to deepened and concretized knowledge about appropriate radiation dose prescriptions for tumor control, such as appropriate radiation doses for control of certain tumors and how the radiation effect can be reinforced to tumors. Recently, a method to maximize tumor control with extreme hypofractionation, called stereotactic ablative body radiotherapy (SABR), has been developed and is being widely used (12). Experience and knowledge about the radiation dose-volume relationship to macroscopic damage and functional disorders in many organs has also accumulated.
Furthermore, various prediction models for estimation of related probabilities have been devised. For instance, tumor control probabilities (TCP) and normal tissue complication probabilities (NTCP) are obtained through mathematical formulas composed of indicators related to tumor control and side effects on normal tissues, respectively (34). These probabilities become important clinical information that enables quantitative judgment on the benefits of (tumor control) and accompanying harms (side effects on surrounding tissues), thereby enabling the justification of the relevant radiation dose prescription when radiotherapies for cancer patients are planned at clinics.
For almost all normal organs that may exist around tumors, threshold doses are also presented in their own way such as TD50/5 (the radiation dose that causes 50% of the patients to have radiation-induced complications within 5 years) and TD5/5 (the radiation dose that causes 5% of the patients to have radiation-induced complications within 5 years). However, these models and threshold doses cannot be regarded as sufficiently reflecting recent diverse dose fractionation schemes and cutting edge treatment techniques, and should be continuously updated. The establishment of these pieces of information enables us to predict the occurrence of side effects more accurately when we plan radiotherapies, induces us to devise diverse alternative methods that may reduce such side effects, and plays the role of a guide to help us not to implement unreasonable treatments, with too-high probabilities of the occurrence of side effects compared to the probabilities of tumor control. It can be said that, compared to the past, more exquisite and safer treatments are implemented now based on these pieces of knowledge.
As for methods of setting target volumes for tumors of cancer patients, in the past, such methods were relatively simple as the locations of shields were drawn on skeletal structures on simple two-dimensional X-ray planes; current methods are quite complicated and exquisite. They require higher expertise as 3D CT images are taken from almost all patients and target volumes are drawn on CT cross sections in every slice (5). As knowledge and experience have accumulated in clinical radiation oncology on the conditions of tumor recurrence after RT, such as recurrences in the central regions of primary cancers, recurrences in the surrounding regions of primary cancers, 1st echelon lymph node recurrences, and 2nd echelon lymph node recurrences, the volume range of treatment judged to have been excessive in the past is gradually decreasing. Since anticancer chemotherapy has also been developing recently, target volumes are generally decreasing in cases where diverse multimodality treatments combining anticancer chemotherapy and radiation are implemented, so that only macroscopic tumors are treated or only macroscopic tumors and adjacent lymph nodes are treated, and this means that less radiation is delivered to surrounding normal tissues.
Image guidance systems to identify the anatomical structures of treatment sites at every time of RT were nonexistent in the past. However, recent RT systems have been installed with computerized tomography 3D volume imaging devices so that the three dimensional structure of the tumor and surrounding normal tissues can be identified at each time of treatment as well as changes in tumor sizes in the case of some macroscopic tumors. There are cases where tumor sizes decrease rapidly even during periods of fractionated RT. For such tumors, the concept termed “adaptive radiotherapy” can be introduced to continuously reduce target volumes when tumor sizes have decreased, thereby gradually reducing radiation exposure to surrounding normal tissues (67). For instance, in one case a large small cell lung cancer decreased by more than 30% after only the first two weeks out of the total treatment period of six weeks. This change was immediately noticed and the target volume was revised to correspond to adaptive radiotherapy. In another case, the head fixing mask of a head and neck cancer patient become loose because the outline of the skin of the patient changed due to rapid loss of neck edema and body weight. The head fixing mask was immediately corrected for accurate treatment under the principles of adaptive radiotherapy for administration of more accurate doses.
This adaptive RT has only become possible due to the introduction of systems that allow for changing complicated treatment designs many times during a treatment process due to increases in the time efficiency of RT plans, something that was not even dreamed of in the past. Adaptive RT can be said to be different from cone down treatment, which treats only those macroscopic tumors that remain after completing radiation irradiation for microscopic tumor control, because of the timing of and reasons for readjustment of targets. In fact, we can conclude that clinical radiation oncology is a study of setting radiation doses and target volumes for prescriptions. In this case, changing appropriate radiation doses and target volumes are intended to reduce radiotherapy’s side effects. Recently, adaptive RT has been developed into a form of actively adjusting treatment ranges for tumors that change in size even during RT periods.
OPTIMIZATION OF THE EFFECTS OF RADIATION ON NORMAL TISSUES FOLLOWING THE DEVELOPMENT OF MEDICAL PHYSICS, COMPUTERS, AND MACHINE ENGINEERING
Entering the 1990s, the development of medical physics, computers, and machine engineering has been extensive, and this development has been naturally incorporated into the field of RT to play an important role in minimizing side effects and protecting normal tissues in treatment ranges. In this section, the core part of such development will be explained concretely.
Dimension change: 2-Dimensional → 3-Dimensional → 4-Dimensional radiotherapy
Two-dimensional therapy is a method of estimating the locations of tumors from the front or lateral side of patients based on bony structures through kilo voltage (kV) X-ray based plain radiographic images. This method is used to apply radiation therapy only anterior-posteriorly or laterally. Clinical RT could not get out of the frame of this two-dimensional approach to therapy for a long time. In the middle of the 1990s, three dimensional (3D) spatial information on patients’ bodies and internal organs obtained through computed tomography (CT) became available as computerized data. This enabled the implementation of 3D RT using computers to plan simulated treatments.
Through the 3D spatial information from CT and Hounsfield Unit information obtained from individual tissues, actual radiation doses absorbed in the body could be known. This was supported by computing ability to calculate the doses, and therefore 3D conformal RT was finally introduced into clinics (8). 3D conformal RT rapidly diffused immediately after commercialization. 3D conformal RT accurately targets tumors in various organs of human bodies. The locations of tumors can be seen at diverse angles and from diverse directions as well as sufficiently dispersing doses on surrounding normal organs to avoid placing any important normal organs in danger, thereby enabling much safer RT (Fig. 1).
Fig. 1
Principles and conceptual diagrams of 2D radiotherapy, 3D conformal radiotherapy, and intensity modulated radiotherapy. (A) 2D radiotherapy: Radiation is administered only anterior-posteriorly or laterally, precisely based on bone structures so that, when treating concave tumors (T), the distribution of prescribed dose (Dark Yellow) becomes rectangular and high dose radiation is focused on the center of the tumor and adjacent normal tissues (N). (B) 3D conformal radiotherapy: The patient’s body is simulated in the computer and radiation can be delivered at diverse angles so that radiation doses to normal tissues outside the tumor can be reduced but radiation dose to normal tissues in the center of tumors cannot be reduced. (C) Intensity modulated radiotherapy: In the case of intensity modulated radiotherapy, unlike 3D conformal radiotherapy in which single direction irradiation can be delivered with only one beam, radiation beams are divided into numerous beamlets to minutely adjust the intensity of radiation. The beams are delivered in 360 degree rotations or at diverse angles so that even normal tissues in the center of tumors can be irradiated with lower doses of radiation than the prescribed dose.

Four-dimensional (4D) RT was introduced in 2010 and has been ever-spreading. 4D RT means taking the motion due to breathing into account in RT plans, such as treatment for tumors (e.g., lung cancer) moving due to breathing. RT systems are always divided into two stages, RT planning and radiation delivery. 4D RT planning obtains CT images that reflect breathing movements, that is, video CT (4D-CT) to plan RT with accurate and sufficient information about the movements due to breathing. In the actual stage of radiation irradiation, diverse techniques are used such as basic 4D RT, in which the patient is instructed to breathe comfortably or shallowly, and the entire movement trajectories of tumors obtained through 4D-CT are regarded as tumors and aimed at. Another technique is the Active Breathing Control method in which the patient holds his/her breathe for 10-20 seconds during which the radiation beams are applied, to restrict and control the range of movement of lung tumors in the lung. 4D-Gating RT monitors respiration motion magnitudes using equipment such as ANZAI Belt TM or Real-time Position Management TM (RPM) to determine a threshold of movements and radiation is administered only when tumors are located in the center of the amplitude, excluding sections in which the amplitude is too large. 4D-Tracking RT applies radiation by following the movements of tumors, using special equipment such as Cyber-Knife (9). These methods, in which movements are sufficiently understood and the movements are restricted or followed, either in the stage of therapy planning or in the stage of irradiation, can be regarded as advanced therapies that can minimize damage to normal tissues around tumors (Fig. 2).
Fig. 2
4D-Radiotherapy concept diagram. (A) Radiotherapy during natural free breathing. In this case, the normal lung tissues in the whole range of the moving Y-axis are irradiated. (B) Gated radiotherapy (window period RT). Radiation beams are alternatingly turned on and off according to the patient’s respiration cycle so that radiation is not administered during the top and bottom parts of the respiration cycle, thereby excluding some normal tissues from irradiation. (C) Gated radiotherapy with active breath control. Although the respiration cycle is followed, radiation is delivered while the patient is holding his/her breath so that relatively small volumes of normal lung tissues are irradiated. (D) Tracking radiotherapy. This is the most ideal therapy, in which the patient breathes comfortably, and an image-guided or respiration sensor-based tracking system follows the patient’s tumors to only deliver radiation to the tumors. In this method, the least volume of surrounding normal lung tissues is irradiated. However, in this case, quite strict quality assurance programs are required because the error tolerance in this irradiation system is very small.

Intensity modulated radiotherapy and multi-leaf collimator
Intensity-modulated RT can truly be said to be a revolutionary scientific development. If RT made a great leap from 2D therapy when 3D conformal RT was introduced, the clinical introduction and commercialization of intensity modulated RT can be said to be a leap comparable to or larger than that. The core concept of intensity modulated RT is minutely modulating the intensities of radiation on the tumor and adjacent surrounding normal tissues every time radiation is administered (10). When the therapy is planned, different tumor regions, that is, high dose prescription regions and low dose prescription regions can be set, and restricted doses can be set for surrounding normal tissues. Thereafter, if the RT planning computer is ordered to generate a RT plan, an optimum dose distribution will be derived through diverse and complicated beam combinations delivered by the multi-leaf collimator (MLC). For tumor targets, if the center of tumors are judged hypoxic and resistant to radiation or are quite densely populated with tumor cells, a higher radiation dose can be prescribed. Parts adjacent to macroscopic tumors or regions judged as harboring microscopically invading tumors can be irradiated with a lower dose of radiation compared to gross tumors. Doses to surrounding normal tissues can also be limited to those that would not cause any side effects. In particular, radiation doses can be restricted very strongly for very sensitive organs. This means that dose distributions in the body can be finely modulated.
The invention of intensity modulated RT can be said to be primarily attributable to the advancement of computer science and the development of the computer-controlled MLC that emits numerous slices of radiation to enable fine modulation. The MLC was first developed as a set of many collimators in the form of small strands that were installed on the head of the radiation generator to relieve radiologic technicians’ efforts to manually insert cerrobend lead block shields for individual directions of irradiation for the patient to fit the form of necessary shielding. The speed of MLC was not very high at the beginning. However, as the thickness of each collimator of a MLC installed on the linear accelerator was gradually reduced from 1.5 cm to 1 cm, to 0.5 cm, and to 0.3 cm now, the movement speed increased so that many fine and diverse slices of radiation can be delivered and treatment of a patient can be completed in only 10-20 minutes.
The AgilityTM 160-leaf MLC recently introduced to the market has 0.5 cm thick collimators that can swiftly move diverse forms of radiation beams at speeds of approximately 6.5 cm per second in a field size of 40 cm × 40 cm to form excellent dose distributions, and the TrueBeam STXTM is equipped with 0.25 cm thick collimators to enable highly precise treatment. The tomotherapy equipment has a Y-axis field limited to 5 cm at the maximum but is installed with a binary MLC that rotates helically for treatment. The movements of the MLC are air-hydraulically modulated at very high speeds to enable very fine modulation of radiation intensities.
In the case of 3D conformal RT, doses to tumors and surrounding normal tissues can be known as resultant values when radiation angles and the intensities of individual beams have been determined. In the case of intensity modulated RT, desired doses or dose limits are set and the computer determines the radiation methods by itself (Fig. 1). Since doses desired in the body can be more freely modulated, more optimal dose distributions can be obtained than with 2D or 3D conformal RT in terms of normal tissue protection for most types of cancers. For instance, whereas 2D or 3D conformal RT cannot reduce doses to the hippocampus that are known to be associated with cognitive dysfunction during whole-brain irradiation for metastatic brain tumors, intensity modulated RT can reduce doses to the hippocampus located in the center of the brain to less than a half of surrounding doses so that fewer side effects from brain treatment can be expected (1112).
Radiosurgical management
Recently, radiosurgery has been attracting the most attention in the field of RT. Radiosurgery is a treatment method that delivers high dose radiation of around 10 Gy for each fraction, and therefore the radiation needs to applied very precisely and accurately. The radiation is delivered in many diverse directions to be concentrated on the tumor so that absorbed radiation doses for surrounding normal tissues are drastically reduced (Fig. 3). As RT has become very precise, tumors very close to normal tissues can now be treated more safely. This technique has become possible through the development of computers, machine engineering, and cutting-edge imaging techniques. This therapy has been actively implemented recently in parallel organs (such as the lung and liver) and has been reported to have been capable of obtaining amazing local control rates of 97% for 20 Gy × 3 fractions = 60 Gy in early-stage lung cancer (1).
Fig. 3
Stereotactic ablative body radiotherapy (SABR) for a single metastatic lung tumor. The right figure shows the beam configuration of SBRT in which radiation is distributed in many diverse directions and the left figure shows the distributions of high-dose radiation confined to the tumor on axial, sagittal, and coronal images.

This therapy has been actively used for early-stage lung cancer, solitary or oligo-metastatic pulmonary cancer, and liver cancer. This therapy is also used for fast pain relief and local control in patients with vertebral metastasis in cases where spinal cord, a serial organ, can be safely excluded. The Gamma-Knife had been the most frequently used device for stereotactic radiosurgery of benign and metastatic brain tumors before equipment dedicated to radiosurgery was commercialized. More recently, linear accelerator equipment has been advanced and refined, and this equipment is threatening existing radiosurgery through smooth incorporation of image-induced techniques. This therapy is usually used only for 3-5 cm or smaller tumors, and requires very careful considerations about surrounding normal tissues and strict quality control.
The dawning of the particle beam therapy age
When discussing the development of radiation oncology, particle beam radiotherapy, that has been attracting great public attention, cannot be omitted. Unlike for photon beams, in the case of particle radiation, due to the nature of radiation beams called Bragg’s peaks, lower doses are absorbed at the surface of the body and most of the energy is released at a certain depth in the body. Therefore, if the depth at which most of the radiation is absorbed can be adjusted, radiation can be concentrated on tumors and radiation doses to normal tissues the radiation passes through before arriving at the tumor can be greatly reduced (13) (Fig. 4). Although particle beam radiotherapy attracted attention to the extent that it has been called a dream cancer treatment method, it is not yet widely used because the installation cost is too high.
Fig. 4
Particle beams and Bragg’s Peaks. Usually, in the case of X-rays (photons), the doses are built up on the surface of the skin and absorbed doses are the highest at approximately 1-3 cm directly below the skin and attenuated thereafter to become gradually lower. On the other hand, particle radiotherapy using particles such as proton or carbon is characterized by Bragg’s Peaks, in which low absorbed doses are administered until a certain depth from the skin and radiation energy is concentrated at a certain depth. In this case, if the depth is adjusted well, radiation can be efficiently delivered to tumors with lower doses than normal tissues. Protons are advantageous in that radiation energy is almost completely dissipated after the Bragg’s Peak and carbon ions are advantageous in that radiation doses are lower than for protons from the skin until the radiation arrives at tumors. It is claimed that since carbon radiation has approximately three times larger biological effects, carbon ions can enhance treatment efficacy in terms of tumor control.

There are other reasons why this treatment method has not yet been widely diffused, not just the high installation cost. Currently, although photon beam-based radiotherapies are applied with excellent image induced and tracking techniques in all processes, ranging from RT planning to irradiation, and multi-fine radiation intensity modulation through MLCs and rotating gantry-based diverse angle irradiation systems are smoothly implemented, proton therapy has not yet been able to surpass the precision of photon beam intensity modulated RT because it irradiates only one direction from fixed systems and only in two to three directions at the maximum when it uses rotating gantries.
However, recently, in the case of proton particle radiotherapy, fine intensity modulated particle radiotherapy has been accomplished with the introduction of scanning beams, and the precision has been enhanced gradually as the number of directions of radiation has been increased to at least five or six. Therefore, although it needs time for technical development, proton particle radiotherapy is expected to eventually develop into a technology that surpasses photon beam therapy. Carbon ion therapy is also expected to become a superior therapy because it has a relative biological effectiveness approximately three times higher than photons or protons. Their Bragg’s peaks have properties that enable them to deliver lower doses to the skin and higher doses to tumors. However, since carbon ions are heavier than protons, this therapy requires larger accelerators and much higher construction costs than does proton therapy. The technical specifications for rotary gantries and scanning beam therapy need to be developed further before commercialization and diffusion of this therapy.
DECREASES OF THE EFFECTS OF RADIATION ON NORMAL TISSUES FOLLOWING THE DEVELOPMENT OF RADIOLOGY AND CUTTING-EDGE IMAGING TECHNOLOGIES
The development of radiology and the incorporation of cutting-edge imaging technologies brought amazing changes to RT. If CT had not been developed, 3D conformal RT and intensity-modulated RT could not have been developed. CT obtains patients’ 3D anatomical structural information, and Hounsfield Unit (HU) values of CT can be used to accurately predict radiation doses in the body in planning prior to RT. Furthermore, image fusion techniques that accurately overlaps CT images, that are the basic ones used in RT planning, with MRI and PET images when treatments such as 3D conformal RT and intensity modulated RT are actually implemented, was developed so that target volumes can be more accurately drawn. Various cancer types, such as brain, prostate, and liver are not well-visualized in CT images but are clearly visible in MRI images. Drawing target volumes on combined images leads to accurate irradiation of tumors and also the exclusion of unnecessary normal tissues from the range of RT (14).
In addition, 4D-CT techniques that can define the trajectories of tumors following actual breathing, such as in the case of a lung cancer that moves according to breathing, by obtaining video images instead of still frames have been commercialized and actively used at clinics. Accurately grasping tumors’ movements according to breathing helps reduce unnecessary exposure of normal tissues to radiation. The grasping of tumor movements through the fusion of diverse images and 4D-CT is necessary in the stage of RT planning, but in addition, many image-guided RT techniques have also been developed so that cutting-edge imaging techniques can be applied to the actual processes of irradiation to help improve the accuracy and precision of treatment.
An in-room X-ray based monitoring system (ExacTrac®) can be installed in the RT room to identify tumor movements during each treatment session within the range identifiable on X-ray images. RT equipment can be installed with kV CT or mV CT so that CT images can be taken in the RT room, when the patient is in the treatment posture, immediately before actual treatment to recheck the CT when the therapy was planned, and the locations of the target and surrounding normal tissues defined in the images before treatment. This minimizes the setup error that may occur during each session of RT and enables adaptive RT. In the cases of tumors moving according to breathing, as mentioned earlier, Active Breathing Control, 4D-gating, and tracking treatment are implemented with the help of cutting-edge imaging techniques. Recently, MRI has been installed on RT equipment to allow RT to be performed while viewing organs in human bodies in real time. This innovation, the ViewRayTM system, was recently developed and just has been commercialized. This equipment is expected to bring about higher accuracy to the RT of tumors that cannot be easily seen through existing CT but can be viewed more clearly through MRI.
Meanwhile, in addition to external radiotherapy, innovations in brachytherapy, commonly used to treat prostate cancer, have made it possible to insert radioactive isotopes more accurately and more precisely by incorporating transrectal ultrasound images. Recently, attempts to fuse MRI images with ultrasound images or CT for initial treatment or post-implant dosimetry planning have been made (1516). In the case of brachytherapy for uterine cervical cancer or other high dose rate brachytherapy, 3D brachytherapy plans using CT or MRI images have been widely applied, and finer and safer treatments are being implemented accordingly (17).
MODULATION OF RADIOTHERAPY-RELATED IMPACTS ON NORMAL TISSUES BASED ON DEEPENED RADIOBIOLOGICAL UNDERSTANDING OF THE EFFECTS OF RADIATION ON HUMAN BODIES
When discussing the effects of radiation on normal tissues in human bodies during RT for cancer, there is a fact that must be always be kept in mind. Although all three major cancer treatment methods (RT, surgical treatment, and anticancer chemotherapy) have been proven to be effective for tumor treatment, they always involve side effects on normal tissues. Modern medicine’s treatments have a limitation in that they cannot remove cancer tissues growing in normal tissues without any effect on the normal tissues. What is important is to what degree the side effects can be reduced while still removing the cancers.
Surgery, anticancer chemotherapy, and RT have different purposes and primarily cooperate with each other under the principle of multidisciplinary treatment in order to cure a patient’s cancer, but in some cases they compete with each. Surgery is more invasive than RT, can in many cases have much more serious adverse effects than the side effects induced by RT, and in many cases is inferior to RT in terms of the quality of life. For instance, in the case of prostate cancer, RT has much lower rates of side effects such as urinary incontinence and sexual dysfunction in comparison to surgery. In the case of laryngeal cancer, RT can preserve the voice, but radical surgery cannot. Surgery is a treatment that should remove the entire organ in which a certain cancer exists or the tumor and a considerable part of surrounding normal tissues, leading to the complete loss of the shape or function of the organ in many cases.
Meanwhile, although anticancer chemotherapy is implemented when a cancer has metastasized or is highly likely to metastasize, or when that type of primary cancer responds very well to anticancer chemotherapy, the anticancer drugs that go into the body through intravascular injection or oral administration cause many systemic side effects such as hair loss, stomatitis, digestive organ mucous membrane inflammations, vomiting, and declines in the functions of the bone marrow. RT is advantageous in that it is less invasive compared to surgery, is more local compared to anticancer chemotherapy, involves the least discomfort or pain during treatment periods, and in general enhances the quality of life the most. The most important thing in cancer treatment is that gains from the treatment are much larger than losses due to the treatment.
The effects of radiation on human bodies are largely divided into deterministic effects and stochastic effects (18). Deterministic effects refer to effects in cases where there are threshold doses of radiation for damage caused by radiation and the level of damage increases as the dose increases. The normal organ damage values such as TD5/5 and TD50/5 mentioned above are reference values of radiation doses for deterministic effects. Deterministic effects show distinctive conditions by organ, and cataract of eye lenses, vertebral nerve damage, small bowel stricture, salivary gland damage, and pulmonary fibrosis are some deterministic effects having threshold doses. In other words, this means that such aftereffects will not occur if the threshold doses are not exceeded.
The introduction of radiation into medicine or human industries has a history exceeding one century, and radiation has been used in many diverse areas. Radiation biology, the study of the effects of radiation on organisms, has been ongoing for a long period of time, correlating with the history of radiation used for examination of human diseases and cancer treatment. However, traditional radiation biology is not sufficiently informed with the molecular biological knowledge that has been developing rapidly recently. In particular, basic molecular biological studies on the effects of radiation on human bodies are extremely insufficient in the area of modern RT dose-fractionation schemes that have recently become diverse and complex, and have come to have different trends of dose prescriptions. One of important reasons for this is that small animal disease models closely reflecting the effects of radiation on human bodies have been lacking in terms of modern clinical RT doses and techniques.
To mimic local RT for humans in small animals, micro-beam irradiation in mm units and image-guiding devices to define the treatment are necessary, but there have been difficulties in the application of these technologies to small animals. As the importance of RT has increased and attention to RT has become higher than ever before, efficient small animal-based transitional studies on the effects of RT on normal tissues have begun only recently. These studies will play a major role in understanding RT related side effects on normal tissues more deeply and help in developing appropriate treatment methods (1920). If the side effects of RT are biologically overcome, relatively more radiation can be delivered to tumors, and this will eventually enhance therapeutic ratios. Although only a few drugs (e.g., amifostine) have been developed to prevent and relieve the side effects of RT’s, more efficient therapeutic agents should be developed through further studies.
Stochastic effects are the effects of radiation on human bodies with no threshold dose or very low threshold doses, and are defined to have after-effects of which the seriousness is not proportional to doses but the incidence is proportional to doses. These are effects on human bodies that are mainly observed in very low dose areas that are far away from clinical RT dose areas. These effects are often due to the effects of radiation on genes and carcinogenesis. Although radiation is recognized as a carcinogen, the evidence for radiation to directly cause cancers is weak, and radiation is classified as a weak carcinogen.
The grounds for arguments that radiation causes cancers rely on cohort studies of survivors of the nuclear bombing on Hiroshima in Japan, in which exposure to radiation and the frequency of cancer onset are related to each other in a proportional relationship between radiation dose and cancer incidence rate. However, if the risk of secondary cancers in cancer patients receiving high dose RT at clinics is calculated based on the formula of the dose-response relationship obtained from the above reports, much higher cancer rates are estimated compared to secondary cancers actually found at RT clinics. This means that the risk for cancers caused by radiation is excessively exaggerated.
It is very difficult to directly prove that a cancer has occurred after RT because of the RT in a cancer patient, because cancers are caused by stepwise variations of genes and composite interactions between genes, and changes in microenvironments for tumors should accompany the interactions. A single factor such as radiation exposure cannot be regarded as the only factor causing the onset of a cancer. The occurrence of additional secondary cancers in cancer patients may not be attributable to RT but may be attributable to the patients’ genetic predisposition, immunodeficiency, common carcinogenic influence, or other environmental factors or interactions between these factors and RT (21).
In fact, although there are many papers claiming an association between RT and cancer onsets, there are also reports arguing that there is no association or very little association between the two, indicating that this matter requires careful attention. Recently, Koshy et al. reported one of the largest studies to examine the role of RT for Stage I and II Hodgkin disease, including SEER data based on long-term follow-ups of 12,247 Hodgkin patients. Their conclusion was that the rate of secondary malignancy did not increase at all among patients who received RT in addition to anticancer chemotherapy compared to patients who had not received RT (22). Welte et al. (23) reported that according to follow-up data from 15,449 patients who received RT from 1981 to 2003, the incidence rates of secondary cancers not related to primary cancers were just 0.5% and 2.2% in the 5th year and the 15th year, respectively. Doi et al. (24) reported that the probability of occurrence of secondary cancers later in children who received RT per 1 Gy of radiation dose was much lower compared to children who survived atomic damage. Zelefsky et al. (25), who surveyed the occurrence of secondary cancers after RT in 2,658 prostate cancer patients, reported that after compensating for the patients’ ages and smoking history, the secondary cancer incidence rate of RT patients was not different from that of patients who had surgery.
Given that cancer incidence gradually increased recently, to the extent than the probability for a general person to contract cancer once during his/her life has been reported to be up to 25%, the interpretation of cancer development due to radiation should be made carefully and objectively. The dispute related to the relationship between RT and cancer development will continue hereafter. However, separately from this dispute, one thing that must be noted and kept in mind when the legitimacy of RT for cancer patients is discussed, is that the possibility of occurrence of cancers after RT is very low, and even if a cancer does occur, it will occur 10-20 years later. Therefore, the use of radiographic images to diagnose and evaluate diseases and RT for treatment of cancers that threaten life now should be addressed separately from the social atmosphere that encourages healthy persons to avoid exposure to radiation. In the case of patients with a disease, medical radiographic examinations or cancer radiotherapies provide much larger gains than damage due to exposure to radiation, unlike in generally healthy persons. Therefore, the correct perception should be applied when considering actively undergoing appropriate radiographic examinations or radiation treatments when necessary, according to the situation.
DEVELOPMENT OF MEDICAL PHYSICAL QA TECHNIQUES AND PROGRAMS
RT for cancer patients is a complicated process that involves many stages. Quality assurance (QA) aims to check the entire process carefully, preventing or minimizing errors that may occur, and effectively improving treatments. When a patient has decided to receive RT, the RT begins with taking images of the site to be treated, such as CT images, by having the patient assume the posture to be used during actual treatment or by making devices to fix certain postures. Thereafter, targets are set on the images obtained, and normal organs are drawn on the images. Then the therapy is planned according to the doctor’s prescriptions to obtain optimum RT dose distributions. During this process, what kind of RT planning equipment and RT equipment will be used become important determinants. When the RT planning process has been completed, all of these computerized pieces of information are transmitted to the RT room. In the RT room, the same posture as the posture taken when the therapy was planned is reproduced, the treatment center point is identified, and radiation is administered.
Immediately before the RT and during the RT, there are processes to check whether the RT is implemented properly. Because RT involves many processes from the moment at which RT is determined to be the appropriate treatment, accurate and efficient quality control programs are necessary for all of the individual processes. In particular, thanks to the development of RT techniques, normal tissues are exposed to relatively less radiation so that gradually higher-dose radiation can be delivered to tumors, to the extent that a one-time dose prescribed for tumors exceeds 20 Gy in some cases. Increases in one-time doses per se mean increases in risks and this also becomes a reason for the necessity of finer and more accurate QA. If not supported by strict controls, RT cannot be implemented safely and accurately no matter how much it is technologically developed. Accurate prediction and measurement of radiation doses administered to human bodies without errors is a foundation of all radiotherapies. Accurate prediction of radiation doses in minute areas is the basis of safer implementation of high-precision RT. Furthermore, the accuracy of the position of RT and the accuracy of dose prediction in organs moving due to breathing are extremely important information in actual treatment, and doctors can implement RT more confidently based on the information.
RT QA is basically divided into periodic QA and patient-specific QA. Periodic QA consists of machine QA, dose QA, and image QA for treatment equipment. This includes QA for the therapy planning system that establishes RT plans, treatment information systems, treatment equipment, and measuring instruments. There is also QA for the process through which individual devices are combined to actually deliver radiation. For such complicated QA, many recognized institutions such as the American Association of Physicists in Medicine (AAPM), the ASRO (American Society of Radiation Oncology), the International Commission of Radiation Units & Measurements (ICRU), the International Atomic Energy Agency (IAEA), the American College of Radiology (ACR), and the European Society of Therapeutic Radiation Oncology (ESTRO) provide efficient and safe quality control protocols (26272829).
Periodic QA can be generally divided into daily, monthly, and yearly QA. Daily QA mainly consists of tests of elements that seriously affect patients’ setups and individual beam ports’ aiming, equipment doses, and basic safety devices. This QA is intended to prevent serious errors from occurring in patients due to wrong treatment procedures. Monthly QA measures detailed areas that may become problems through gradual accumulations of errors over approximately one month, based on the premise that daily QA of equipment is implemented properly and controls for factors that cause systematic errors in many patients, although not revealed easily such as beam uniformity. Yearly QA conducts measurements comparable to receiving inspections conducted when equipment is introduced, and careful inspections of equipment to check conformity with the therapy planning system. According to the results, there may be a need to implement maintenance of modeling in the QA or therapy planning system. Ideally, all measurements should be conducted at the level of yearly QA, but this will cause problems in time and labor power due to precise measurement. Accordingly, combinations of the most ideal frequencies for the maintenance of treatment equipment and measuring methods that fit the frequencies are recommended in the form of QA at different frequencies to enable finding the balance between costs and efficiency.
Recently, surpassing the basic QA in RT processes, individual QA has been implemented for the safety of treatments of individual patients. This QA can be divided into pre-treatment QA that is implemented as end-to-end tests of treatment processes before patient specific treatment, and in-vivo measurements to evaluate accuracy in the process of actual treatment. This QA is intended to secure the safety of treatments of individual patients, recognizing the limitations of the hardware and software that predict doses actually delivered to patients, and considering human factors that may occur. Patient-specific QA means the process to check whether the actual radiation delivered is the same as the treatment plan for each patient, through therapy planning and radiation processes that are the same as those for the actual patient but implemented on a human body model phantom before treating the patient. In the newest cutting-edge treatment methods in which the operation of mechanical devices for radiation irradiation is complicated and exquisite, target volumes and normal tissues are close to each other, changes in doses are large in boundaries, or one-time delivery doses are larger than normal fractional doses. To implement these processes in all patients, large amounts of manpower and time are necessary and investments in this manpower, equipment, and time leads to patients’ safety and accurate RT. In the case of high-precision treatments such as intensity modulated RT and stereotactic body radiation surgery, patient-specific QA needs to be implemented in all patients.
In 2010, the New York Times reported intensity modulated RT and other RT related accidents. The full text of the article comprehensively addressed human mistakes, machine failure, and software problems that lead to so-called catastrophic failure. Mentioning the risk of RT that is not properly controlled, this article reported that 621 cases of treatment errors occurred in the State of New York between 2001 and 2008. As a result, changes in the paradigm of advanced cutting-edge RT QA were needed (2830). Accordingly, surpassing the existing quality control of related hardware and software, recent QA programs require the construction of QA systems based on actual risks in treatment through analysis of failure modes in the entire process. Major methods include Failure Mode Effectiveness Analysis (FMEA). FMEA analyzes the processes of RT, defining possible “Risks” by stage, and analyzing the probability for the risks to lead to failure modes (Occurrences), the severity of the failure modes, and the ease of detecting the risks through quantitative methods to configure radiation treatment safety systems (3132).
By now in 2015, RT has undergone great development mechanically and systematically as compared to the past, leading to improvement in the accuracy of RT and decreases in the frequency of mechanical or human mistakes or errors. In other words, while RT equipment or systems in the past had relatively more problems compared to those of now, the newest RT equipment has been changed to be excellent in stability and accurate in the delivery of prescribed radiation doses. In general, RT is implemented now with much lower error rates than in the past. However, although the stability of the equipment has become excellent as such, and system errors are decreasing, ironically, RT QA is becoming more complicated, more time-consuming, and more difficult. This is because, although the overall stability improved thanks to the introduction of computer systems, highly severe errors appear in forms that cannot be easily detected in complicated detailed processes.
Meanwhile, RT QA processes have become complicated and sophisticated, to the extent that the resultant demand for manpower and equipment cannot be met. To overcome this problem, Systematic RTQA programs have been coming to the fore recently. These programs are intended to adjust the efficiency and safety of RT to achieve balance through treatment process analysis methods such as FMEA, using resources available in each process of treatment. These programs are intended to control failure modes occurring in complicated processes most effectively, even with the restrictions on funds and resources, through systematic and appropriate approaches designed by expert groups. RT and quality control will undergo processes to be continuously developed so that accurate radiation doses prescribed can be delivered to tumors and less radiation can be delivered to surrounding normal tissues.
Recently, various clinical studies have been actively conducted as domestic multicenter studies or through participation in international clinical studies. In these cases, if RT is included in the clinical study protocols, the RT should be managed by each institution that conducts the study using domestically/internationally unified protocols and quality control programs. In international clinical studies, in the USA, RT quality control is conducted by an institution named Imaging and Radiation Oncology Core (IROC, formerly the Radiation Physics Center [RPC]). General verification procedures are implemented up to 3D-CRT and in the case of IMRT, Site Specific QA under a concept similar to Patient Specific QA is added (33). In Europe, RT quality control is managed by an institution named Equal Estro (34), and in Korea, the Korea Food and Drugs Administration is in charge of RT quality control.
CONCLUSION
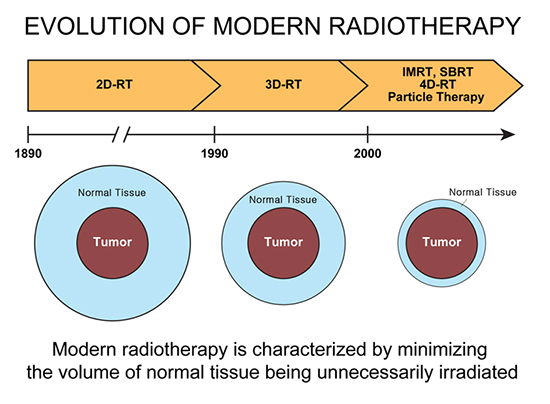
RT has been playing important roles in cancer treatment for more than one century. From the latter half of the 1990s onward, it has been re-writing the history of cancer treatment as new cutting-edge treatment methods were poured out with the help of the development of medical physics, computers, and machine engineering (Fig. 5). The development of RT has allowed for irradiating tumors with higher doses while continuously reducing the radiation doses delivered to surrounding normal tissues. The newest cutting edge radiotherapies are treating tumors with amazingly high efficiency that could not be even be dreamt of in the past, while minimizing radiation impact on surrounding normal tissues.
Fig. 5
Evolving clinical cancer radiotherapy over a century. Radiation has played important roles in cancer treatment over a long time, more than 100 years. Following the development of computers and machine engineering, an age of 3D treatment has come about only in the middle of the 1990s, when 3D conformal radiotherapy began to be diffused widely, and at the beginning of the New Millennium age, cutting edge treatment methods such as IMRT, SBRT, and particle therapy were commercialized and have widely diffused, so that the second act of the history of radiation cancer treatment could commence.

As RT has become more important, along with the advent of diverse cutting-edge treatment methods, small animal model based radiation biological studies have been developed recently, and active studies to overcome the side effects accompanying RT through molecular biological mechanisms are in progress. As RT has become more complicated and finer, precise QA is necessary in all procedures from the beginning to the end of RT for accurate aiming and the administration of accurate radiation doses. Although errors were maximally reduced through periodic QA of equipment or systems in the past, recently, an age has come in which RT is implemented while verifying doses according to therapy plans for individual patients. As RT relies on technical development, cutting-edge technologies will be continuously developed and the field of radiation cancer treatment will continuously develop accordingly. In addition, as biological understanding of the effects of RT on surrounding normal tissues has become deeper, it is hoped that cancer treatment with no RT-related side effects will be developed some day. In an age when 2/3s of cancer patients survive longer than five years, and in an age when patients’ quality of life in life after treatment is emphasized, it is expected that RT, which is a noninvasive treatment, can continuously improve the quality of life in terms of preservation of organs and functions after treatment.
 XML Download
XML Download