

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Nuclear medicine is a rapidly growing discipline that employs advanced technology. Medical practice gets significant benefit from molecular imaging procedures such as single-photon emission computed tomography (SPECT), positron emission tomography (PET), and from novel hybrid techniques such as single-photon emission computed tomography/computed tomography (SPECT/CT) and positron emission tomography/computed tomography (PET/CT), which provides unique functional and anatomical information relevant for patient management. Molecule-targeted therapy is also growing fast, with continuous development of approaches aimed to fight several forms of cancer.
The rapid growth of nuclear medicine practices inevitably leads to an increase in medical exposure to radiation. At the same time, public interest in such exposure has also increased, even more since Fukushima nuclear power plant disaster in 2011. However, irrational phobia to radiation sometimes leads to distortion of sound medical practices from the point of view of clinicians. Therefore, a rational management of medical exposure to radiation is needed more than ever in Korea.
In this article, current status, and the implementation of radiological justification for an optimization of nuclear medicine practices in Korea will be discussed through a brief review of the recommendations of the International Commission on Radiological Protection (ICRP).
CURRENT STATUS OF NUCLEAR MEDICINE PRACTICE IN KOREA
The Korean Society of Nuclear Medicine (KSNM) has been collecting data on nuclear medicine practice since 1962. Although these data have some limitations because the method of classification of practices varies by year, they are enough to understand temporal trends of nuclear medicine practice in Korea. Therefore, these statistical data were used in this review.
Gamma camera imaging
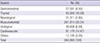
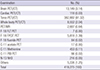
The use of gamma camera in nuclear medicine examination has constantly increased since 1962, showing a plateau in 2006, and reaching 560,993 examinations in 2013 (Fig. 1). In 2013, imaging examinations for musculoskeletal diseases accounted for approximately 50% of the total, and of this, Tc-99m MDP bone scan accounted for most of the cases. Thyroid and cardiovascular diseases accounted for 17% and 14% of cases, respectively (Table 1). In total, 227 conventional gamma cameras, and 33 SPECT/CT scanners (12.7%) have been installed until 2013. Among gamma camera imaging examinations, SPECT/CT examinations were performed in 7,717 cases (1.4%; Table 2).
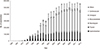
Table 1
Diagnostic nuclear medicine examinations using gamma camera in 2013 done in Korea
![]()
Table 2
Diagnostic nuclear medicine examinations using SPECT/CT in 2013 done in Korea
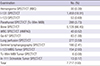
Ga-67, gallium 67; MIBI, methoxyisobutylisonitrile; MIBG, metaiodobenzylguanidine; WBC, white blood cell; SPECT/CT, single-photon emission computed tomography/computed tomography; HMPAO, hexamethylpropyleneamineoxime.
![]()
PET imaging
The first PET scanner was installed in Korea in 1994, and the first PET/CT scanner was installed in 2002. After June 1 2006, the National Health Insurance has covered PET examinations in Korea (Fig. 2). Analyzing by range of scan, torso PET(/CT), which covers from the eyebrow to the thigh, accounted for more than 90% of scans, while brain and whole body PET(/CT) followed, in 2013 (Table 3). Analyzing PET scanner type, the number of standalone PET scanners was only three, but the number of PET/CT scanners was 138 in 2013, because the fusion of PET with CT has had great clinical success. This phenomenon is far ahead comparing to SPECT/CT scanners, which have replaced only 14.7% of the conventional gamma cameras. In 2011, Asia's first integrated positron emission tomography/magnetic resonance imaging (PET/MR) scanner was installed in Korea, and four PET/MR units were installed until 2013. PET/MR scans accounted for approximately 0.64% of total PET examinations because it is too expensive.
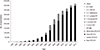
Table 3
Diagnostic nuclear medicine examinations using PET(/CT) in 2013 done in Korea
FLT, fluorothymidine; FPCIT, fluorinated N-3-fluoropropyl-2β-carbomethoxy-3β-(4-iodophenyl) nortropane; N-13 NH3, nitrogen-13 ammonia; PIB, Pittsburgh compound B.
![]()
Therapies with radiopharmaceuticals
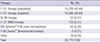
Nuclear medicine treatment continued to increase, after a plateau in 2009, reaching 30,759 cases treated in 2013 (Fig. 3; Table 4). I-131 therapy for thyroid cancer accounted for over 99% of the cases. Sr-89 treatment for palliation of metastatic bone pain, I-131 metaiodobenzylguanidine (MIBG) therapy for neuroendocrine tumors, SIR-Spheres® Y-90 resin microspheres for liver malignancies, and Y-90 Zevalin® (ibritumomab tiuxetan) for lymphoma accounted for the rest of cases treated; however, it has not been proven that treatment with these radiopharmaceuticals improve survival rate, and either are for too rare diseases, or too expensive.
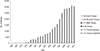
Table 4
Radiopharmaceutical therapies performed in 2013 in Korea
![]()
IMPLEMENTATION OF RADIOLOGICAL JUSTIFICATION FOR NUCLEAR MEDICINE PRACTICE
Recommendations of the ICRP for justification for medical exposure to radiation
According to the ICRP, the main aim of medical exposure to radiation is to do more good than harm to the patient, and the principle of justification applies to three levels within the use of radiation in medicine (Table 5) (1).
Table 5
The ICRP recommendations on radiological justification and optimization in medicine

*In practice, the values are selected on the basis of a percentile point on the observed distribution of doses to patients or to a reference patient.
![]()
● At a first level, the use of radiation in medicine is accepted as doing more good than harm to the patient. This level of justification can now be taken for granted, and will not be discussed further in this review.
● At a second level, a specified procedure with a specific objective is defined and justified. The aim of the second level of justification is to judge whether the radiological procedure will improve diagnosis or treatment, or will provide necessary information about the exposed individuals.
● At a third level, the application of the procedure to a patient should be justified. Therefore, each medical exposure to radiation should be justified in advance, taking into account the specific objectives of the exposure, and the characteristics of the individual involved.
The justification for a radiological procedure is a matter of national and international professional bodies in conjunction with national health and radiological protection authorities, and the corresponding international organizations. Decisions about risk and effectiveness of existing and new procedures should be reviewed from time to time, as more information becomes available. It is often possible to speed up the justification process by defining referral criteria and patient categories, in advance.
Implementation of radiological justification for nuclear medicine practice by international professional bodies
A practical method to implement radiological justification is to follow proper referral guidelines according to the recommendations of the ICRP. Therefore, radiological justification for nuclear medicine practice has been implemented mainly by referral guidelines (Table 6).
Table 6
Referral guidelines for implementation of radiological justification in nuclear medicine

| Professional bodies | Guidelines |
|---|---|
| International professional bodies | SNMMI; evidence-based referral guidelines |
| Oncology Practice Guidelines Summary from multiple organizations for major cancer Types (2,3,4,5,6) | |
| Cardiac Practice Guidelines Summary (7) | |
| ACR; evidence-based rating referral guidelines to assist in making the most appropriate imaging for a specific clinical condition | |
| ACR's Appropriateness Criteria® (8) | |
| ATA; evidence-based rating referral guideline through collaboration with related academic societies | |
| Revised American Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer (2009) (9) | |
| Korean professional bodies | KSNM; evidence-based rating referral guidelines |
| Clinical application of 18F-FDG PET in various cancer (10) | |
| Clinical application of 18F-FDG PET in Neurology (27) | |
| KTA; evidence-based rating referral guidelines through collaboration with related academic societies | |
| Revised Management Guidelines for Patients with Thyroid Nodules and Thyroid Cancer (11) |
SNMMI, Society of Nuclear Medicine and Molecular Imaging; ACR, American College of Radiology; ATA, American Thyroid Association; KSNM, Korean Society of Nuclear Medicine; KTA, Korean Thyroid Association.
Numbers in parenthesis are reference numbers.
![]()
The Society of Nuclear Medicine and Molecular Imaging (SNMMI) has been using evidence-based referral guidelines such as the National Cancer Center Network (NCCN) guidelines for the implementation of nuclear medicine practice (234567). These guidelines are intended for referring physicians, as well as nuclear medicine physicians and radiologists. These practice guidelines are revised and updated periodically, and new guidelines are written. The NCCN guidelines have an advantage reflecting referring physician's view point because these guidelines were not made by the SNMMI itself but made by cancer centers that means referring physicians.
The American College of Radiology (ACR) has been publishing evidence-based rating referral guidelines (8). These guidelines have an advantage to assist in making the most appropriate imaging for a specific clinical condition among clinically available imaging modalities with grading.
Regarding therapy, the American Thyroid Association (ATA) has been publishing evidence-based rating referral guidelines of I-131 therapy for thyroid cancer through collaboration with related academic societies (9). Members of the taskforce included experts in thyroid nodule and thyroid cancer management with representation from the fields of endocrinology, surgery, and nuclear medicine.
Implementation of justification for nuclear medicine practice in Korea
Legal regulation on the use of radiation in medicine is stated at the administrative rule under the Nuclear Safety Act in Korea. Previously these acts mainly deal with relevant technical standards. After revision in 2013, the definition and responsibility of medical radiation exposure are stated.
According to Article 50—i.e., Protection and Management of Medical Radiation Exposure—of the “rules relating to technical standards, such as radiation safety management,” which were revised on December 19, 2013, medical exposure to radiation covers the following: 1) Exposure of individuals for medical purposes; 2) Exposure of embryos/fetuses or infants during medical exposure to radiation of patients who are pregnant or breastfeeding; 3) Exposure of individuals such as family and close friends who are helping in the support and comfort of patients; 4) Exposures incurred by volunteers as part of a program of biomedical research.
Regarding justification, Article 50 (i.e., Protection and Management of Medical Radiation Exposure) states the following: 2) Those who use radioactive isotopes in humans should do so that the benefits are greater than the harm caused by radiation exposure. While Article 51 (i.e., User's Responsibility) states that: 1) Those who use radioactive isotopes in humans should do so that a doctor who has sufficient expertise in medical radiation protection uses medical radiation; 2) Unless they have checked the radiation protection plan and referred to the doctor’s prescription and informed consent from the patient or legal guardian regarding medical exposure to radiation, those who use radioactive isotopes in humans should avoid the use of radiation; 4) According to claim 1), the user should review the justification for and optimization of medical exposure to radiation periodically, based on the Notice of the Nuclear Safety and Security Commission of the Republic of Korea (NSSC), and should maintain records of medical exposure.
Above mentioned relevant regulation and the ICRP recommendations, radiological justification for nuclear medicine practice has been implemented mainly by referral guidelines in Korea. In the case of fluorine-18 fluorodeoxyglucose (F-18 FDG) PET/CT examination, which is the most frequent diagnostic nuclear medicine practice in Korea, the KSNM has published periodically evidence based rating referral guidelines of its own for F-18 FDG PET/CT examination for each disease in its journal (10). These referral guidelines have been created using evidence-based approaches such as rating prospective randomized control studies. Regarding therapeutic nuclear medicine practice, I-131 therapy for thyroid cancer is the most employed, accounting almost 99% of all therapeutic practices in Korea. The KSNM has published guidelines of I-131 therapy for thyroid cancer through collaboration with related academic societies (1112). These guidelines were mainly based on the ATA guidelines, so there are minor differences considering Korean situation.
Although there is no clear remark of the effect of health insurance policy on the ICRP recommendations, whether the National Health Insurance Service covers specific practices on a certain clinical indication can result in great impact on medical exposure to radiation in Korea. For example, the Health Insurance Review & Assessment Service (HIRA), which is under the Ministry of Health and Welfare, changed the health insurance policy for F-18 FDG PET/CT examinations in December 1, 2014. Thereafter, the number of examinations using F-18 FDG PET/CT examination is expected to decrease to 60%-80% levels suddenly.
IMPLEMENTATION OF RADIOLOGICAL OPTIMIZATION FOR NUCLEAR MEDICINE PRACTICE
Recommendations of the ICRP for optimization of protection to medical exposure to radiation
According to the ICRP, in the case of exposure from diagnostic medical procedures, the diagnostic reference level (DRLs) is recommended for the optimization of protection, but it is not implemented by individual patient dose constraints. It is a mechanism to manage patient doses in order to be commensurate with the medical purpose.
DRLs apply to exposure of patients to radiation from procedures performed for medical imaging purposes. They do not apply to radiation therapy. In the practice, values are selected based on a percentile point on the observed distribution of doses to patients, or to a reference patient. Values should be selected by professional medical bodies in conjunction with national health and radiological protection authorities. And these values reviewed at intervals that represent a compromise between necessary stability and long-term changes. The selected values could be specific for a country or region.
DRLs are used in medical imaging to indicate whether, in routine conditions, levels of patient-dose, or administered activity (i.e., amount of radioactive material) for a specific imaging procedure are unusually high or low for that procedure. If so, a local radiological review should be initiated to determine whether protection has been adequately optimized, or whether a corrective action is required (13). The DRL should be interpreted as a readily measurable patient-dose-related quantity for the specific procedure.
Implementation of radiological optimization for nuclear medicine practice by international professional bodies
To determine DRLs in nuclear medicine, the National Council on Radiation Protection and Measurements of the USA (NCRP) surveyed a part of the Unite States and ACR-AAPM adopted this DRL and recommend using it for optimization. In practical view full national survey is very difficult, they adopted this partial national data (Table 7) (14).
Table 7
Guidelines for radiopharmaceuticals dose optimization in nuclear medicine

| Professional bodies | Guidelines |
|---|---|
| International professional bodies | ACR-AAPM; guideline presents diagnostic reference levels |
| ACR-AAPM Practice Parameter for Reference Levels and Achievable Administered Activity for Nuclear Medicine and Molecular Imaging (14) | |
| cf) Reference Levels is based on NCRP partial national survey data. | |
| SNMMI; Procedure Standards containing dose recommendations, equipment QC, personnel qualification (15) | |
| SNMMI-EANM; harmonized pediatric dose guideline | |
| Pediatric radiopharmaceutical administration: harmonization of the 2007 EANM pediatric dosage card (version 1.5.2008) and the 2010 North American consensus guidelines (17) | |
| IAC Nuclear/PET; standard for PET accreditation | |
| The IAC Standards and Guidelines for Nuclear/PET Accreditation (18) | |
| Korean professional bodies | Regarding DRLs; survey is under progress |
| KSNM starts surveying Individual hospital protocols for calculation of administered doses through the KSNM website. | |
| KSNM is developing a survey method for CT Dose Index (CTDI) and Dose Length Products (DLP) | |
| KSNM; procedure guidelines including dose recommendations | |
| Nuclear Medicine Procedure Manual (20) | |
| 18F-FDG PET Procedure Standard (21) | |
| KSNM; technical standard for radiopharmaceuticals related personnel and facilities | |
| KSNM technical standard for procedures using radiopharmaceuticals (28) | |
| Regarding accreditation; relevant foundation is under progress | |
| KARA and other agencies have been performing certification services | |
| A foundation tentatively named the "Institute for Quality Management of Nuclear Medicine," is being established |
ACR, American College of Radiology; AAPM, American Association of Physicists in Medicine; NCRP, National Council on Radiation Protection and Measurements; SNMMI, Society of Nuclear Medicine and Molecular Imaging; EANM, European Association of Nuclear Medicine; KSNM, Korean Society of Nuclear Medicine; KTA, Korean Thyroid Association.
Numbers in parenthesis are reference numbers.
![]()
DRL is an optimization tool in national level but the DRL itself does not recommend administered dose of each hospital for a certain practice. Therefore, before determining of DRLs, dose recommendations are needed. The SNMMI recommends each radiopharmaceuticals administered dose through ‘SNMMI’s Procedure Standards’ of each practice (15). To enhance accessibility on recommended dose, the SNNMI provides radiation dose tool which provides adults guidelines for protocol selection and injected activity, broad estimates for effective dose and absorbed dose to the critical organs through dose optimization website (16). Regarding pediatric nuclear medicine, special attentions have been paid because children are more sensitive to radiation, several guidelines have been proposed by international professional bodies. But there are some differences in pediatric dose among international guidelines. To resolve this difference, in 2014, harmonized guideline was made by EANM and SNMMI (17).
Since the goal of dose optimization is to keep radiation exposure as low as reasonably possible without deteriorating diagnostic performance, quality controls for both equipment and standardized procedures are required for nuclear medicine imaging. For this respect, the SNMMI has been recommending ‘SNMMI’s Procedure Standards’ series (15). These procedure standards help to identify those elements of the procedure that are most important in obtaining a high-quality examination, while simultaneously controlling costs. Some standards were formally adopted by the SNMMI in collaboration with other professional organizations. These standards include quality controls for both equipment and standardized procedures and recent standards include qualification of personnel (physician, technologist, medical physicist, radiopharmacist, radiochemist, radiation safety officer) also.
Continuing quality assurance is an integral part of the present-day practice of medicine. The Intersocietal Accreditation Commission (IAC), Nuclear/PET offers accreditation as an increasingly renowned method for Nuclear Medicine, Nuclear Cardiology and PET facilities to evaluate and demonstrate the level of patient care they provide. Serving as the basis for the accreditation program, the Standards are the extensive document defining the minimal requirements for Nuclear/PET facilities to provide quality patient care. Facilities are encouraged to use the Standards as both a guideline and the foundation to create and achieve realistic quality care goals (18).
Optimization is not a matter of administered dose, but is a matter of image quality also. So, theoretically the concept of DRL has some limitation. And DRLs have been used for over two decades to detect and bring down wide variation in radiation doses. Very limited success has been achieved through DRL. Therefore, recently a new term ‘acceptable quality dose’ (AQD) that is aimed at optimization within the DRL, is facility initiated and takes into account all three important parameters—image quality, dose and patient’s body build is proposed (19).
Implementation of diagnostic reference levels for nuclear medicine practice in Korea
Legal regulation on radiological optimization is stated at the administrative rules under the Nuclear Safety Act in Korea. Article 50—i.e., Protection and Management of Medical Radiation Exposure—of the “rules relating to technical standards, such as radiation safety management,” which were revised on December 19, 2013, states that: 2) Those who use radioactive isotopes in humans should do so that the benefits are greater than the harm caused by radiation exposure; 3) The user, according to claim 2), should keep radiation exposure to a low range where it is reasonably possible taking into account economic and social factors. Article 51—i.e., User's Responsibility—states that: 1) Those who use radioactive isotopes in humans should do so that a doctor who has sufficient expertise in medical radiation protection uses medical radiation; 4) According to claim 1), the user should review the justification for and optimization of medical radiation exposure periodically, depending on the Notice of the NSSC and should maintain records of medical exposure.
Above mentioned relevant regulation and the ICRP recommendations, radiological optimization for nuclear medicine practice has been implemented in Korea. Although there is no DLR data such as the NCRP’s, individual hospital protocols for calculation of administered doses are submitted annually through the KSNM website. Since radiation exposure, not only from radiopharmaceuticals, but also from CT should be taken into account in multi-modality imaging procedures such as PET/CT and SPECT/CT, the KSNM is developing a survey method for CT Dose Index (CTDI) and Dose Length Products (DLP), which is a readily measurable patient-dose-related quantity.
Regarding recommended administered activity, the KSNM also recommends through procedural manual of each practice based on SNM technical standards (20). But regarding pediatric nuclear medicine, diverse international dose recommendations have been used in Korea. In 2014, new harmonized guideline between SNMMI and EANM was introduced, so dose difference in pediatric nuclear medicine will be expected to decrease.
To achieve good imaging quality, procedural guidelines for each nuclear medicine practice are available at the KSNM website, although part of them are under revision (21). In the revised procedural guidelines, recommendations on drinking plenty of fluids and frequent bladder emptying will be included in order to reduce radiation exposure without compromising diagnostic performance. In addition, reasonably increasing the administered activity to reduce examination time that can be used in elderly patients with pain, will also be included.
The KSNM and the Korean PET association promoted a voluntary quality control program for PET studies, and conducted a pilot project. Since the implementation of a Standard Certification System in November 2011, the Korean Association for Radiation Application and other agencies have been performing certification services for the Ministry of Health and Welfare. The KSNM, in conjunction with the Korean Society for Nuclear Medicine Technology (KSNMT), has a committee that provides standards for quality control of nuclear medicine imaging. In addition, a foundation tentatively named the “Institute for Quality Management of Nuclear Medicine,” which is similar to the “Korean Institute for Accreditation of Medical Image,” is being established under the Ministry of Health and Welfare.
IMPLEMENTATION OF PROTECTION FOR CAREGIVERS AND COMFORTERS OF PATIENTS TREATED WITH RADIONUCLIDES
The recommendations of ICRP for protection of caregivers and comforters of patients treated with radionuclides
Precautions for the public are rarely required after the performance of diagnostic nuclear medicine procedures. However, some therapeutic nuclear medicine procedures (e.g., those involving I–131), can result in a significant exposure for other people, particularly those involved in the care and support of patients (1). Therefore, the public caring for such patients in hospitals or at home require consideration.
The ICRP Publication 94 provides recommendations for the discharge of patients after therapy involving radionuclides. These recommendations state that for radiological protection purposes (i.e., be subject to a public dose limit of 1 mSv/year), young children, infants as well as visitors not engaged in direct care or comforting should be treated as members of the public (22). For individuals directly involved in comforting and caring, other than young children and infants, a dose constraint of 5 mSv per episode (i.e., the duration of a given discharge after therapy) is reasonable. The constraint needs to be used flexibly. For example, higher doses may be appropriate for parents of very sick children. The thyroid gland of persons under the age of 15 years is more radiosensitive than that of adults; thus, particular care should be taken to avoid contamination of infants, children, and pregnant women from patients treated with radioiodine. The decision to hospitalize or discharge a patient after radionuclide therapy should be made on an individual basis taking into account several factors such as residual activity in the patient, patient’s wishes, family consideration (particularly the presence of children), environmental factors, and existing guidance and regulations. The unintentional exposure of the public in waiting rooms or in public transportation is usually not high from nuclear medicine patients, except radioiodine (2223).
Implementation of protection for caregivers and comforters of patients treated with radionuclides by international professional bodies
For the Implementation of protection for caregivers and comforters IAEA recommends using patient instruction card (24). They recommend radiation safety officer or medical doctor fill out the restriction periods on close contact and provide to the released patients. This card has an advantage of simplicity to enhance compliance of patients (Table 8).
Table 8
Guidelines for implementation of protection for caregivers and comforters of patients treated with radionuclide

| Organization | Guidelines |
|---|---|
| ICRP | The 2007 Recommendation; dose constraint for caregivers and comforters |
| 5 mSv per episode | |
| 1 mSv for young children, infants, and visitors | |
| International professional bodies | IAEA; Patient instruction card containing restriction periods determined by each hospital |
| https://rpop.iaea.org/RPOP/RPoP/Content/Documents/Whitepapers/patient-information.pdf (24) | |
| ATA; guideline presents restricted periods according to the administered activities | |
| Korean professional bodies | Radiation Safety Guideline for I-131 Thyroid cancer therapy (25) |
| MRSRC; radiation safety instruction for I-131 Thyroid cancer therapy presents restricted periods according to the administered activities | |
| Radiation Safety Instruction for I-131 Thyroid cancer therapy (26) |
ICRP, International Commission on Radiological Protection; IAEA, International Atomic Energy Agency; ATA, American Thyroid Association; MRSRC, Medical Radiation Safety Research Center
Numbers in parenthesis are reference numbers.
![]()
Radiation safety is an essential component in the treatment of patients with thyroid diseases by I-131. The ATA published one of the most useful guidelines (25). The ATA created a task force to develop recommendations that would inform medical professionals about attainment of radiation safety for patients, family members, and the public. Examples of the development of tables to ascertain the number of hours or days (24-hour cycles) of radiation precaution appropriate for individual patients treated with I-131 for thyroid cancer have been provided. Reminders in the form of a checklist are presented to assist in assessing patients while taking into account individual circumstances that would bear on radiation safety. Information is presented to supplement the treating physician’s advice to patients and caregivers on precautions to be adopted within and outside the home.
Implementation for protection of caregivers and comforters of patients treated with radionuclides in Korea
Legal regulation on radiological protection for caregivers and comforters is stated at the notice under the Nuclear Safety Act in Korea. Article 12—i.e., Isolation and discharge criteria for patients—, of the NSSC Notice on “technical standards on radiation safety management in the medical field” effected on April 1, 2015, states that: Those who use radioactive isotopes in humans for treatment purposes should provide patients with instructions on how to keep radiation levels as low as reasonably possible in other individuals. In these instructions, the following information should be included: ① Minimize contact time with the patient depending on the dose of the administered radioisotope; ② Restrict patients treated with radioisotopes to crowded places; ③ Minimize pollution caused by patient's feces, etc; ④ Precautions for breastfeeding or planning pregnancy; ⑤ Caution when using airport security X-ray detection devices; ⑥ Information on the impact of ionizing radiation on human health; ⑦ Name and telephone number of an available contact person when there are additional questions.
Based on above mentioned relevant regulation and the ICRP recommendations, protection for caregivers and comforters of patients treated with radionuclide has been implemented in Korea. The most important change in above mentioned revision refers to “Restricting crowding of patients treated with radioisotopes to certain places.” This change relates to a recent phenomenon in which patients with thyroid cancer crowded in care hospitals after I-131 treatment, in Korea. If patients go to their homes, it is not a problem from the point of view of radiation safety management. However, if patients crowd in care hospitals, it can lead to problems such as repeated exposure of personnel, or exceeding environmental limits.
Based on above mentioned revision, the Medical Radiation Safety Research Center made a standard instruction and distributed each hospital (26). This instruction includes restriction periods for public transportation, sleeping, return to work on and limitation of using accommodation including care hospital. Before this, each hospital used their own modified international instruction, so there were some differences in restriction periods. After this standard instruction, deviation of restriction periods in Korea will decrease.
SUGGESTIONS FOR THE FUTURE
Radiological justification for nuclear medicine practice in Korea has been implemented by referral guidelines of the KSNM, as discussed in the previous section. In addition, in order to implement radiological optimization, a survey has been performed on the protocols that determine the dose to be administered for each radiopharmaceutical. However, for optimization purposes, further efforts are required.
Software for the monitoring of patient dose of radiation
In 2012, the Korea Food and Drug Administration (KFDA) developed a CT radiation dose monitoring software (i.e., KDose), which is available as freeware. KDose was developed as a prototype that can automatically import CT radiation dose information from hospital medical records. However, this software is for CT radiation monitoring only; thus, for the nuclear medicine field, additional functions are needed. For example, in the case of F-18 FDG PET/CT, information on the dose of injected radiopharmaceutical is recorded at the acquisition workstation. New patient-radiation-dose monitoring software should be able to receive this information at the same time.
National registry and management system of patient-radiation-dose
A national registry and management system of patient-radiation-dose is also required to determine the need for on-site radiological review, which is recommended by the ICRP. Currently, only basic functions have been performed by the KSNM. Some alternatives to the national patient-radiation-dose management system can be considered: 1) the Radiation Safety Committees based on the Nuclear Safety Act, which are already established in each hospital, play a key role; 2) Government establishes a new foundation and delegates management; 3) Government delegates management to the Medical Radiation Safety Research Center. Cooperation among these entities and the tentative “Institute for Quality Management of Nuclear Medicine” is essential, because image quality and dose optimization is tightly linked.
CONCLUSION
Nuclear medicine practice is rapidly growing in Korea, so a rational management of medical exposure to radiation is needed more than ever. Radiological justification for and optimization of nuclear medicine practice in Korea has been implemented by evidence based referral guidelines and protocol survey that determine the dose for each radiopharmaceutical. Administered dose optimization is in progress considering image quality control. Radiological protection for caregivers and comforters after radionuclide therapy has been implemented by standard instruction to released patients. Although these implementation activities pursuit the ICRP recommendations, further efforts are required for optimization purposes. The development of patient-radiation-dose monitoring software, and a national registry and management system of patient-radiation-dose is needed to implement radiological optimization through diagnostic reference levels. This management system must work in agreement with the “Institute for Quality Management of Nuclear Medicine”, and must take into account the medical reality of Korea, such as low medicine fee, in order to implement reasonable radiological justification and optimization.
 XML Download
XML Download