

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Back pain is a common problem that afflicts 70%-85% of people in their lifetime and 15%-45% annually (1). Patients hesitate to undergo surgery; in addition, surgical treatment is recommended to only indicated patients due to various sources of pain and inconstant surgical results (23). These causes increased use of nonsurgical and conservative treatment such as spine intervention to avoid surgery. Many interventional procedures such as epidural steroid injection, facet joint block, medial branch block, nerve root block, and sacroiliac joint injection are used to relieve back pain (4).
Most interventional procedures use X-ray to identify imaging landmarks and confirm the precise location for percutaneously inserted needle under fluoroscopy or C-arm guidance (5). “As low as reasonably achievable (ALARA)” principles should be respected when X-ray is used because excessive radiation to a patient or a physician can cause radiation injury or stochastic effect such as neoplasm and genetic mutation (67). Several articles reported radiation dose for spine intervention (89101112) and some revealed factors that affect radiation dose; however, no study has investigated the effect of the fluoroscopy unit controller. Either the physician or radiographer can control the fluoroscopy unit in fluoroscopy-guided procedures. The aim of this study was to evaluate a difference of fluoroscopy time and radiation dose depending on medical staff operating the fluoroscopy unit. We also evaluated other factors related to radiation dose in spine interventions including patients’ body habitus, a type of procedure, and image magnification.
MATERIALS AND METHODS
We performed 500 spine interventional procedures in the same fluoroscopy unit at our institution between June and December, 2014. This study included the three most common interventional procedures of nerve root block, medial branch block, and facet joint block performed at the lumbar spine; however, we excluded procedures without a proper dose report or two or more different types of procedures done simultaneously. Eventually 268 procedures in 220 patients were included in this study; 86 procedures were performed on 78 men and 182 procedures on 142 women. The mean age of patients was 63 years with range of 22-93 years and the mean body mass index (BMI) was 24.5 kg/m2 with range of 16.5-39.5 kg/m2.
All procedures were performed by two physicians with three-year (physician A) and one-year experience (physician B). When physician A performed the procedures, the fluoroscopy unit was controlled by a radiographer in the control room according to the physician’s instructions; however, physician B controlled the unit directly without assistance in the examination room. They used the same fluoroscopic unit (Axiom Artis, Siemens Healthcare, Erlangen, Germany). Procedures at two or more levels of the lumbar spine were done simultaneously on some patients and some patients underwent procedures several times.
We recorded treatment related factors such as multiplicity of treated region, procedure type, and physician who performed the procedure. We collected radiation dose data measured by the built-in dose area product (DAP) meter and fluoroscopy time from radiation dose reports generated by the fluoroscopy unit. We also reviewed the fluoroscopic images of all procedures to evaluate if X-ray beam collimation or image magnification was used. Treatment responses for procedures were collected from medical records to evaluate outcomes. A lack of detailed medical records on pain assessment required that treatment responses be divided into improvement or no improvement in symptoms. Our institution does not use spot images for spine intervention; therefore, the number of spot images was not recorded.
Descriptive statistics including median, range and interquartile interval of fluoroscopy time and DAP (Gy∙cm2) were calculated. We used nonparametric analysis as the data did not approximate a normal distribution. Spearman correlation test assessed the correlation of radiation dose and patient’s BMI as well as radiation dose and fluoroscopy time. We classified all procedures into two groups by the performing physician; Group A and B by physician A and B, respectively. A χ2 test compared the frequency of several factors between two groups. A Mann-Whitney U test compared fluoroscopy time and radiation dose between two groups as well as analyzed differences in fluoroscopy time and radiation dose according to multiplicity of the treated regions, response after treatment in each group, and a difference in radiation dose according to magnification. A Kruskal–Wallis H test compared differences of fluoroscopy time and radiation dose among the type of procedures. A P value < 0.05 was considered statistically significant.
RESULTS
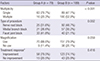
We analyzed 268 procedures by physician A (n = 79) and physician B (n = 189). The most common procedure was a nerve root block. Physician B performed significantly more procedures at multiple levels of the spine. Pain relief was indicated for 181 procedures, no pain relief for 58 procedures, and no medical records of treatment response for 29 procedures. There was no significant difference in frequency of symptom improvement between two groups (P = 0.416). Table 1 summarizes the number of procedures according to multiple factors.
Table 1
Treatment related factors in lumbar spine interventions in each group
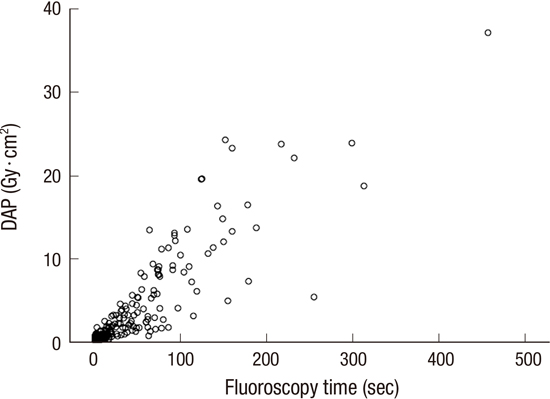
The mean DAP and fluoroscopy time of all procedures were 3.3 ± 5.4 Gy∙cm2 (range, 0.05-37.01 Gy∙cm2) and 39.1 ± 59.08 seconds (range, 1-457 seconds), respectively. In all procedures, fluoroscopy time was significantly and positively correlated to radiation dose (correlation coefficient = 0.886, P < 0.001) (Fig. 1). BMI, known to affect radiation dose, did not show a significant correlation to radiation dose (correlation coefficient = 0.108, P = 0.143).
Fig. 1
Patient radiation dose versus fluoroscopy time. Scatter plots show a relationship between radiation dose and fluoroscopy time. There is a positive correlation between fluoroscopy time and radiation dose (correlation coefficient: 0.886, P < 0.001).

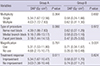
There were significant differences in radiation dose and fluoroscopy time between two groups. Group A, by physician A who did not control the fluoroscopy unit, showed a significantly longer fluoroscopy time and higher radiation dose than Group B (P < 0.001) (Table 2). There was significant difference in fluoroscopy time according to type of procedure in Group A; however, there was no difference in radiation dose in both groups. Magnification caused a significantly higher radiation dose in Group B. There was no significant difference in radiation dose in each group according to multiplicity of treated regions and treatment response. Table 3 and 4 summarizes fluoroscopy time and radiation dose (= DAP) according to all evaluated factors in two groups.
Table 2
Comparison of fluoroscopy time and dose area product (DAP) according to variables

| Time & dose | Group A* | Group B* | P value |
|---|---|---|---|
| Fluoroscopy time (sec) | 72.0 (33.8-114.5) | 6.0 (3.0-20.3) | < 0.001 |
| DAP (Gy·cm2) | 5.31 (1.72-11.28) | 0.59 (0.26-1.33) | < 0.001 |
Table 3
Comparison of fluoroscopy time (sec) according to variables in two groups
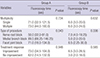
Table 4
Comparison of DAP (Gy∙cm2) according to variables in two groups
DISCUSSION
The routine use of X-ray in fluoroscopy-guided minimally invasive procedures has made radiation dose exposure an important issue. Analysis in this study indicated that fluoroscopy time and radiation dose were significantly decreased when the physician controlled the fluoroscopy unit directly comparing with when the physician supervising the radiographer controlling the fluoroscopy unit. Additionally radiation dose increased when image magnification is applied.
The results showed significant differences in fluoroscopy time and radiation dose between two physicians that corresponded to those of a previous study (8). However, a previous study indicated that more radiation dose and more fluoroscopy time were recorded for physicians who had less procedural experience. In our study, the less experienced physician (physician B) used less X-ray for procedures than the more experienced physician (physician A). An important difference between two groups was that different personnel controlled the fluoroscopy unit. Physician A allowed a radiographer to control the unit and physician B controlled the unit without assistance. When a physician controlled the fluoroscopy unit, they could immediately turn on or off the machine without delay and fluoroscopy time could be shortened. Our study showed the direct control of the fluoroscopy unit by a physician was more influential in decreasing fluoroscopy time than the physicians’ experience. It is also important to note that physician B performed procedures properly and that there was no difference in treatment responses between two groups.
Two physicians seemed to have different level of awareness about radiation exposure that made a potent difference in fluoroscopy time and radiation dose. This supposition was supported the fact that most images during physician A's procedures contained the physician’s hands and those during physician B's procedures did not. It is imperative that physicians who conduct fluoroscopy-guided examinations make efforts to prevent radiation from directly contacting their hands. Awareness about radiation exposure itself was well-known as an important factor to decrease radiation dose (1314).
Procedures with image magnification caused a significantly higher radiation dose than without magnification in Group B. This result showed that magnification caused more radiation exposure. Magnification is necessary when a small area is examined and a detailed structure is required; however, image magnification should be used selectively. Unlike Group B, there was no significant difference in Group A for radiation dose in examinations with or without magnification. It could be explained by that fluoroscopy time had a stronger effect than magnification on the radiation dose for Group A.
Fluoroscopy time was different according to type of procedure in Group A, but radiation dose was similar. A precise comparison of the results of our study and previous studies was impossible as previous studies included different procedures (812); however, the results suggest a commonality in the type of spine intervention that helps determine fluoroscopy time. A difference in fluoroscopy time could be explained by the familiarity or difficulty of the procedures.
Radiation exposure from spot images is distinct and additional to that from fluoroscopy; therefore, spot images during fluoroscopic procedures increased radiation exposure. Prior efforts have been made to reduce radiation dose by the use of last image hold in other fluoroscopic examinations (1516). In our institution, a spot image was not taken from all spine interventions. The experience in our institution indicated that preferable outcomes could be obtained after spine interventional procedures without spot images. We believed that common spine interventional procedures should be performed without spot images if the fluoroscopy unit has a last image hold function.
Our study has several limitations. First, we could not perform a cross comparison due to the retrospective design of this study. There is a possibility that differences between two physicians might be caused by individual preferences; however this is doubtful due to the significant differences between the two methods of a fluoroscopy unit controlled by physician directly and that controlled by another medical staff. Second, only two physicians performed all interventional procedures. Individual skill and experience could relate to radiation dose and fluoroscopy time rather than awareness. The physician who used fluoroscopy for a longer time had more experience and indicated no difference in treatment response; therefore, it seemed more reasonable that fluoroscopy time and radiation dose differences were due to the physician’s habit and awareness. Third, we could not evaluate the effect of X-ray collimation to radiation dose due to the small number of procedures that used a not-collimated X-ray beam.
In conclusion, there is a significant difference of radiation dose depending on whether a physician or a radiographer operates the fluoroscopy unit. This can be explained by that direct control of the fluoroscopy unit can lead to shorten fluoroscopy time. In addition, image magnification increases radiation dose. The selective use of fluoroscopy and non-use of magnification does depend upon the physician, therefore, physicians should perform procedures using fluoroscopy carefully in order to minimize radiation exposure.
 XML Download
XML Download