

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Major mental disorders usually occur in early adulthood and often go through a chronic progression, so they result in large burdens for the society and country as well as patients and families (1). However, until the 1980s, the burden of mental disorders had been seriously underestimated because the disease burden was measured mainly with fatality (2). The first Global Burden of Disease Study in 1990 (GBD 1990) reported that neuropsychiatric disorders accounted for more than a quarter of all nonfatal burden, measured in years lived with disability (YLDs), and after that, mental, neurological, and substance use disorders emerged as major health problems in the public health area (3). According to the Global Burden of Disease Study 2010 (GBD 2010), the burden of mental and substance use disorders increased by 37% between 1990 and 2010 and became the leading global cause of all nonfatal burden of disease (4).
The burden of mental and substance use disorders is mainly composed of YLDs, and a crucial aspect in the calculation of YLDs is the disability weight (DW). Because the DW reflects the social preferences for the different nonfatal health states, it may vary across cultures, social groups, and periods (5). Therefore, it is important to apply country-specific and regularly updated DW when measuring the YLDs of mental and substance use disorders.
In previous studies in Korea (678), the burden of disease for mental and substance use disorders using Korea-specific DW has been estimated (9), and the studies reported consistent results with GBD studies (34): The burden in females was greater than in males and depressive disorders were the leading cause. However, more information about other mental disorders by gender and age groups was limited (67). One study estimating the Korean burden of disease focused on mental disorders and reported more disease-specific results by gender and age groups (8). However, the measurement was conducted only on mental and substance use disorders (it did not consider other diseases or injuries), so the relative burden of mental and substance use disorders compared to other diseases and injuries was not investigated. Furthermore, while the health care environment has widely changed in Korea, the Korea-specific DW has not been updated since the development in 2006.
Korea has a National Health Insurance System (NHIS), which is compulsory and required by Korean law, so it is available to estimate prevalence and incidence for all diseases and all populations (10). Since it is difficult to obtain epidemiological data about minor mental disorders (idiopathic intellectual disability, pervasive development disorders, conduct disorders, etc.) and childhood and adolescence at the national level, although the NHIS data includes only medical care utilization cases, it is a useful data source for a comprehensive burden of disease study.
The purpose of this study was to estimate the national burden of mental and substance disorders on medical care utilization in Korea using NHIS data and updated disability weight, as well as to explore the characteristics of this burden with respect to gender and age. This study was conducted as a part of the Korean Burden of Disease Study 2012 (KoBD 2012) (11), so we intended to investigate the relative burden of mental and substance use disorders compared to other diseases and injuries.
MATERIALS AND METHODS
In this study the burden of mental and substance use disorders on medical care utilization was measured using DALYs, an index of the burden of disease. DALYs are derived from the sum of years of life lost (YLLs) due to premature mortality and YLDs due to disability resulting from disease morbidity and injuries. The concept and approach were consistent with the original GBD study (12), with some modifications to make the study more suitable for the Korean population and comparable with other burden of disease studies.
Data and subjects
The Korean NHIS covers about 97% of the population and is supposed to contain complete medical records. We used NHIS data (10) to estimate the prevalence and incidence rates of mental and substance use disorders in medical care utilization. These morbidity data were analyzed to estimate YLDs. The residents registered with the Ministry of Interior in 2012 (13), 2012 causes of death statistics, and life expectancy tables from Statistics Korea (14) were used for calculating YLLs. The reference year for this study was 2012. To be consistent with previous Korean burden of disease studies, we divided the subjects into 9 age groups (0–9, 10–19, 20–29, 30–39, ... , 70–79, ≥ 80 years) to use as base cases.
Case definition
To be included, specific mental and substance use disorders had to meet the threshold for a case according to criteria described in the 6th Korean Classification of Diseases (KCD-6) based on the 10th revision of the International Classification of Disease (ICD-10). Compared to GBD 2010 (12), an expanded list of mental and substance use disorders was assessed. The GBD 4-level hierarchical structure was maintained, which included 20 level III–IV causes. We removed fetal alcohol syndrome, which was a level IV cause, due to its lack of relevance, and added borderline personality disorder, which was a level III cause, and atypical eating disorder, which was a level IV cause. Anxiety disorders, which were level III causes, were specified as 4 level IV causes: panic disorder, obsessive-compulsive disorder, posttraumatic stress disorder, and phobic anxiety disorders. This study also included 12 level III causes and 24 level III–IV causes attributable to mental and substance use disorders (Supplementary Table 1). Detailed information about the disease classification has been published elsewhere (11).
Estimation of years lived with disability
The incident-YLDs were calculated by multiplying the number of incident cases (I) at a certain age with a health outcome (x) by the duration of the health outcome (t) and the disability weight (DW) assigned to the health outcome x.

The prevalence cases were defined based upon main diagnosis by considering both hospitalization cases and outpatient clinic cases. The incident cases were extracted from the prevalent cases, having a wash-out period of 1–5 years from 2012 (from 2007 up until 2011). Through literature reviews and expert opinions, the final cases were defined depending on disease characteristics (Supplementary Table 2). The DisMod-II software program (15) was used to model duration and remission from estimates of prevalence, incidence, case fatality rates, and background mortality. The case fatality rates were driven by prevalent cases from NHIS data and death cases from causes of death statistics.
We used disability weights developed for the KoBD 2012. This study had 20 disability weights for mental and substance use disorders. Some level III causes, such as drug use disorders, anxiety disorders, and eating disorders, have a level IV cause, which has no disability weight, so the smallest of their sub-classification was applied. Also, other mental and behavioral disorders, level III causes, have no disability, so the smallest of the 20 disability weights, dysthymia, was applied. Detailed information about the disability weights for the method has been published elsewhere (16).
This study applied time discounting and age-weighting. Time discounting means that future life years are assigned less value than those lived today. A 3% discount rate was chosen to allow international comparisons and because this rate is recommended by the International Panel on Cost Effectiveness in Health and Medicine (17). Age-weighting was based on the existence of a broad social preference to value a year lived by a young adult more highly than a year lived by a young child or an older person. We used standard age-weighting (C = 0.1658, β = 0.04) according to the original GBD study.
Estimation of years of life lost to premature mortality
The YLLs due to premature death were calculated by summation of the number of fatal cases (d) due to health outcome (x) in a certain period multiplied by the residual expected life expectancy (e) at the age of death.

Life expectancy data came from Life Table for Korea (14)—which publishes age- and sex-specific Korean statistics annually—in 2012. According to this, the Korean life expectancy at birth was 77.95 years for males and 84.64 years for females. Age-weighting and time-discounting were applied as with the YLDs.
Ethics statement
This study was performed as a part of the KoBD 2012, funded by the Ministry of Health and Welfare. The study was approved by the institutional review board of Korea University (1040548-KU-IRB-13-164-A-1). More detailed information about the input data and methods can be accessed elsewhere (11).
RESULTS
The burden of mental and substance use disorders in Korea for 2012 was 945,391 DALYs, accounting for approximately 6.2% of the total burden of disease, which was found to be the 7th greatest burden of disease. Mental and substance use disorders accounted for 7.34% of all nonfatal burden, whereas it accounted for just 0.63% of all fatal burden.
It was found that YLDs accounted for 98.5% of all mental and substance use disorder burden, out of which the vast majority was nonfatal burden. In particular, among children and adolescents (under 19 years old), YLDs accounted for 100% of the burden. The burden of mental and substance use disorders occurred across all ages and was predominant in people in their 30s to 50s, showing an inverted U shape. DALYs in male individuals accounted for 44.2% of the burden. Male individuals accounted for 406,135 YLDs (43.6%) and 11,581 YLLs (82.1%). From the 20–29 age group onward, women had a greater burden from mental and substance use disorders than did men. On the other hand, in children and adolescents the burden was greater in males than it was in females, by 1.2 times for 10–19 years and 2.4 times for 0–9 years (Table 1).
Table 1
Burden of mental and substance use disorders by gender and age groups in Korea, 2012
Within the mental and substance use disorders group, unipolar depressive disorders accounted for most DALYs, followed by schizophrenia, anxiety disorders, and bipolar affective disorder. Idiopathic intellectual disability, pervasive development disorders, and conduct disorders (which were assessed for the first time in Korean estimates) contributed about 3.7% of DALYs from mental and substance use disorders (Table 2). The distribution of causes contributing to YLDs was similar to DALYs but differed from YLLs. For YLLs from mental and substance use disorders, alcohol use disorders accounted for the majority, with 85.8%, followed by schizophrenia, drug use disorders, eating disorders, and other mental and behavioral disorders. Only these five causes contributed to fatal burdens, while another six causes had nonfatal burdens only (Fig. 1).
Table 2
The estimated burden of mental and substance use disorders in Korea

Fig. 1
Proportion of YLDs, YLLs, and DALYs explained by each mental and substance use disorder group in Korea, 2012. (A) Proportion of YLDs. (B) Proportion of YLLs. (C) Proportion of DALYs.

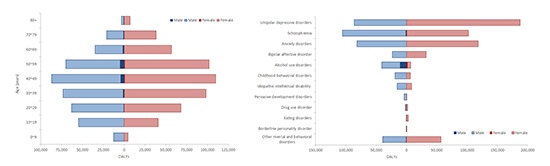
Fig. 2 shows the age distribution of DALYs for each mental and substance use disorder by gender. The burden associated with schizophrenia rose abruptly in adolescence (ages 10–20 years) and peaked in early adulthood (ages 20–40 years). The burden associated with unipolar depressive disorders and anxiety disorders rose in more early ages (0–9 years) and peaked in middle adulthood (ages 40–59 years); females especially increased more steeply than males. For alcohol use disorders, the largest burden occurred in males aged 40–59 years, and for childhood behavioral disorders, the largest burden occurred in males aged 10–19 years.
Fig. 2
Disability-adjusted life years (DALYs) for each mental and substance use disorder in Korea, 2012, by age. (A) DALYs of each mental and substance use disorders for male. (B) DALYs of each mental and substance use disorders for female.

Fig. 3 shows the ranking by gender and age for the burden of mental and substance use disorders. Females accounted for more DALYs in most mental disorders, except for schizophrenia, childhood behavioral disorders, idiopathic intellectual disability, and pervasive development disorders, where males accounted for more DALYs. Males also accounted for more DALYs than females in alcohol use disorders by 5.8 times. Females had greater DALYs from unipolar depressive disorders in all age groups, except the 0–9-year group, where childhood behavioral disorders accounted for more DALYs, and the 20–29-year group, where schizophrenia accounted for more DALYs (a more detailed result by age group for female is provided in Supplementary Table 3). Males had greater DALYs from schizophrenia in ages 20–40. From 50 years old onward, males had a greater burden from unipolar depressive disorders, whereas males under age 19 had a greater burden from childhood behavioral disorders (a more detailed result by age group for male is provided in Supplementary Table 4).
DISCUSSION
The KoBD 2012 was conducted to measure the burden of disease on medical care utilization based on NHIS claims data. It measured the loss of health caused by 345 level IV disease causes for individuals of all ages and both sexes in terms of DALYs. In 2012, the Korean burden of mental and substance use disorders was 1,860 DALYs per 100,000 people and accounted for 6.2% of the total burden of disease. These diseases were the 7th greatest contributor and were more responsible for the total burden of disease than were digestive diseases, transport injuries, HIV/AIDS, and tuberculosis (11).
In the GBD 2010 study (4), the Korean burden of mental and substance use disorders was 2,178 DALYs per 100,000 persons; this figure is 17% higher than the comparable figure in our study. Much of this difference can be ascribed to differences in epidemiological data. The GBD 2010 study used community survey data, and if epidemiological data were not available for a country or region, imputation was used (4). In contrast, we used epidemiological data from health care records for all populations. Because treatment rates for people with mental and substance use disorders are low (1), the results of our study were smaller than the GBD 2010. Also, there were methodological differences in estimating the YLDs. In the GBD 2010 study, prevalent-based YLDs were estimated without age-weighting and time-discounting. In contrast, this study estimated incident-based YLDs with age-weighting and time-discounting. These methodological differences would have an influence on the difference in the results between the GBD 2010 and this study. Despite the differences in the methodology and data sources, gender differences in the burden of mental and substance use disorders remained consistent: Males accounted for more DALYs from mental disorders occurring in childhood, schizophrenia, and substance use disorders, whereas more DALYs were attributed to females for all other disorders. In the GBD 2010 study, the burden of substance use disorders accounted for 20% or more, but in our study, it was only 5%. Because treatment rates for substance use disorders are particularly low, this was reflected in the results. For example, the one-year prevalence of alcohol use disorders was 6.6% in the 2011 survey data (1), while it was 0.5% in the 2012 NHIS data. Therefore, further research is needed using more reliable data and methods to estimate the burden of substance use disorders.
In the KoBD 2002 (6), which was the first Korean burden of disease study, the burden of mental and substance use disorders was estimated based on NHIS data, using Korean disability weights. Comparing our results with the KoBD 2002, the burden of mental disorders increased by about twice as much between 2002 and 2012. Much of this increased burden can be explained by changes to disability weights and medical care utilization for mental disorders. In the KoBD 2002, 12 disability weights for mental and substance use disorders were developed, and most of these (schizophrenia, autism and Asperger’s syndrome, borderline personality disorder, obsessive–compulsive disorder, panic disorder, substance use disorder, eating disorders, posttraumatic stress disorder, and attention-deficit/hyperactivity disorder) have been increased, whereas only three disability weights (mental retardation, bipolar disorder, and unipolar major depression) have been decreased. This reflects how the Korean social preference toward mental and substance use disorders has been somewhat exacerbated, and it increased the burden of mental and substance use disorders. According to an epidemiological survey of mental disorders in Korea (1), the medical care utilization rate for mental disorders rose from 8.9% in 2001 to 15.3% in 2011. That also had an impact on increasing the burden of medical care utilization for mental and substance use disorders. According to the GBD 2010 (4), demographic changes have a greater impact on the changing burden of mental disorders than changes in disease epidemiology. Over the past decade Korea has experienced demographic changes: As a result of falling fertility rates and rising life expectancy, the Korean population is aging more rapidly (18). Such a demographic change would contribute to the increase in the burden of mental and substance use disorders in Korea.
More than 98% of DALYs were from YLDs, meaning that the number of years of living with disabling mental disorders is long. Mental and substance use disorders cause not only psychological, social, and economic burden but also increase the risk of physical disorders (19). Comorbidity is common among those with mental disorders (20), and the comorbidity of mental and physical disorders is on the rise, presenting a main challenge to medicine in the 21st century (21). Therefore, it is necessary that the burden of mental and substance use disorders be addressed from a more comprehensive aspect related to other diseases.
The burden of disease in women was greater than that in men, but the burden in boys aged less than 19 years old was greater than that in girls. These gender differences were consistent with results from previous studies (4678). In childhood (0–9 years old), the burden of mental and substance use disorders of girls was less than half that of boys; however, in adolescence (10–19 years old), girls’ burden of mental and substance use disorders greatly increased by six-fold, whereas boys’ burden increased by three times. In childhood, the leading cause of the burden of mental and substance use disorders was childhood behavioral disorders; however, the burden caused by childhood behavioral disorders was very small in girls. Therefore, in children and adolescents the burden in males was greater than it was in females. These results can be used as a basis for selecting priority diseases and high-risk groups in the mental health area(s) to which resources should be concentrated.
Depressive disorders were the leading cause of total burden from mental and substance use disorders; however, compared to a previous study (6), the proportion of depressive disorders decreased from 49% in 2002 to 29% in 2012. In the past (8), depressive disorders were the leading cause in all gender and age groups, except for males aged 10–29 years old, but in 2012, depressive disorders were the leading cause only in males aged 50 years old and over and females aged 30 years and over. In childhood (0–9 years) and male adolescence (10–19 years), childhood behavioral disorders were the leading cause, and in male youth (20–49 years old) and female youth (20–29 years old), schizophrenia was the leading cause. These results indicate that the composition of the burden of mental and substance use disorders has become diversified. Therefore, the health care plan for mental and substance use disorders should be designed in various ways depending on the disease characteristics.
Anxiety disorders accounted for 21% of the burden of mental and substance use disorders, which was found to be the 3rd greatest burden. This is first time revealing anxiety disorders as one of the major diseases because in previous studies anxiety disorders were not included (67) or were only partially included (8). In a previous study (8), panic disorder, obsessive–compulsive disorder, and posttraumatic stress disorder were included as anxiety disorders, whereas in this study, extended anxiety disorders, which added phobic anxiety disorders (F401, F402, F408, F409, F411, F412, F413, F418, F419, F430, F432, F438, F44), were assessed. The burden of phobic anxiety disorders accounted for 73% of the total burden from anxiety disorders, indicating that the burden of anxiety disorders has not identified their considerable number. Also, in the GBD 2010, the Korean burden of anxiety disorders was the 2nd greatest burden from mental and substance use disorders (4). This result demonstrates how the burden of disease due to anxiety disorders has increased significantly in Korea recently; therefore, anxiety disorders should be considered important.
Alcohol use disorders accounted for most YLLs, with 85.8%, and most occurred in males aged 40–59. The burden from alcohol use disorders accounted for 5.1% in our study, whereas it accounted for 11% in another domestic study (8) and 11.1% in the GBD 2010 (4). The burden of drug use disorders accounted for 10.8% in the GBD 2010, whereas it accounted for only 0.5% in our study. The measured burden from substance use disorders varied significantly across studies; therefore, there is a need for more research in order to more accurately measure the burden from substance use disorders in Korea.
The strengths of this study areas follow: First, this study applied updated disability weights for measuring YLDs. Since the Korea-specific disability weights were developed for KoBD 2002, these disability weights were used in most domestic studies. However, social preferences are reflected in disability weights and, thus, are likely to change over time; therefore, updates were required. Recent Korea-specific disability weights made this study more reliable and valid than it might otherwise have been. Second, we investigated relative burden of mental and substance use disorders compared to other diseases and injuries. This helps to determine the public health priority for mental and substance use disorders. Third, we expanded the list of mental and substance use disorders. Korea NHIS is compulsory and required by Korean law, and the information on medical care utilization for all people is recorded in the NHIS database. Diagnoses were coded using KCD-6 according to ICD-10; thus, it was possible to extract the incidence or prevalence of all the diseases defined by ICD-10. Consequently, NHIS data are used in many public health researches. Taking advantage of the NHIS data, idiopathic intellectual disability, pervasive development disorders, conduct disorders, and phobic anxiety disorders were assessed for the first time in a domestic study. However, this study did not include neurological diseases such as Alzheimer’s disease or Parkinson’s disease. Still, there is a disadvantage of using NHIS data: Because the treatment rates for mental and substance use disorders are low, the prevalence rates used in this study were low compared with the prevalence rates from another community survey (1), whose rates were greater than in our study by 1.25–29 times Therefore, the burden from mental and substance use disorders might be relatively low compared with other chronic diseases in the KoBD 2012. However, this result reflects the current state of medical care utilization due to mental and substance use disorders in this country as it is.
Mental and substance use disorders contribute to a significant proportion of the Korean burden of disease for medical care utilization despite their low treatment rates. Across the globe the burden of mental and substance use disorders has increased, and this change is largely due to population growth and changing age structure (4). Korea is also experiencing such a demographic change, and it will lead to increases in the burden of mental and substance use disorders. Therefore, mental and substance use disorders need to be embraced by mainstream health care, with resources commensurate with the burden.
 XML Download
XML Download