

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
During oxidative metabolism, mitochondria consume oxygen reducing it by sequential steps to water. A small proportion of this oxygen is converted to highly reactive and toxic derivatives known as reactive oxygen species (ROS). Such species include among others superoxide anions, hydrogen peroxide, lipid peroxides and hydroxyl radicals. Within limited concentrations, ROS play important roles as regulators of many cellular functions since they act as secondary messengers to activate specific transcription factors, and as mediators of signaling transduction pathways in cell growth, proliferation and apoptosis (1). However, when ROS production exceeds natural cellular levels, indiscriminate damage occurs involving cellular organelles and alteration of the structure of macromolecules such as membrane lipids, nuclear and mitochondrial DNA and proteins (2). Cytotoxicity occurs as a result of alteration in the expression of genes including those related to apoptosis (3). To combat the harmful oxidative effects of excessive ROS production, cells have evolved antioxidant enzymes which act to scavenge such species. These enzymes include a cytosolic Cu/Zn-superoxide dismutase and a mitochondrial Mn-superoxide dismutase which catalyse the conversion of superoxide anions to hydrogen peroxide. The generated hydrogen peroxide is then transferred to water by the activity of glutathione peroxidase (GPx) and catalase (CAT) (4). Glutathione peroxidases are a family of seleno-proteins which quench both hydrogen peroxide and lipid peroxides (5). They act by transferring the energy of reactive peroxides to reduced glutathione (GSH) thus forming oxidized glutathione (GSSG) which is then reduced back to GSH by glutathione reductase (GR) using NADPH as an electron donor (6). In addition to antioxidant enzymes, cells combat excessive ROS generation using non-enzymatic antioxidants. These include ascorbic acid, α-tocopherol, reduced glutathione, betacarotene, carotene, ferritin, ceruloplasmin, transferrin and the micronutrients selenium, copper, zinc and manganese (7). A delicate intracellular balance between ROS production and antioxidant activity is thus maintained leading to cellular homeostasis. When this balance is perturbed and shifts in favor of oxidative reactions and progressive generation of increased ROS, a state of oxidative stress (OS) happens which has been associated with numerous human pathologies that include atherosclerosis, hypertension, inflammation, cystic fibrosis, senescence, Parkinson's disease, Alzheimer's disease, and female reproductive diseases including pregnancy related disorders (789).
Recurrent miscarriage (RM), defined as three or more consecutive pregnancy losses before twenty four weeks of gestation, affects 0.5%-3% of women in the reproductive age group (710). Known causes of RM include chromosomal and metabolic abnormalities, uterine anatomic anomalies, immunologic disorders such as systemic lupus erythematosus or antiphospholipid syndrome, blood clotting disorders such as hyperho-mocystinemia, infectious diseases, endocrinopathies, polycystic ovary syndrome and sperm DNA fragmentation (7911). However, in 50%-60% of RM patients the causative agent cannot be identified and is classified as idiopathic (9). OS and loss of antioxidant capacity have also been implicated in playing a role in the etiopathogenesis of pregnancy related disorders including RM (791011). It is suggested that impaired placental development or degeneration of syncytotrophoblast in early pregnancy may be caused by oxidative stress that leads to RM (12). Biochemical markers of ROS-induced membrane damage such as lipid peroxidation products have been shown to increase before abortion (13). In addition, OS has been related to pregnancy loss and other pathological conditions of female reproduction (1213) including preeclampsia, intrauterine growth restriction, and RM (7914). Furthermore, RM has been related to the presence of inflammatory cytokines and high levels of ROS (15). Many studies have shown significantly decreased GPx and CAT activities and selenium (Se) levels as well as increased lipid peroxides and malondialdehyde (MDA) levels in serum and/or placental tissue of RM patients (131416171819). However, whereas one study indicated significantly decreased concentrations of plasma total thiols and erythrocyte GSH in RM patients (20), another (21), showed significantly higher plasma GSH levels in RM women compared to healthy pregnancies and non-pregnant women. In addition, another study (22) reported no significant differences in plasma lipoperoxide levels and erythrocyte GPx activity in RM women. Moreover, whereas two studies (2324), demonstrated no significant differences in Se plasma levels of control and RM patients, three other studies showed significantly lower Se levels and GPx activity in groups of other patients (252627).
Due to the above conflicting results and the paucity of related studies, the status of oxidants and antioxidants in RM patients need to be further addressed. This study was undertaken to comprehensively investigate and relate GPx, CAT, SE and GSH activities and concentrations, to those of the corresponding oxidants including H2O2, lipid peroxides (monitored by measuring MDA and GSSG in plasma), whole blood and placental tissue of RM women.
MATERIALS AND METHODS
Subjects of the study
The study population was comprised of three groups of women, those classified as healthy pregnant women (HP) (n = 25), those who underwent RM (n = 25) and healthy non-pregnant controls (NP) (n = 15). HP and NP subjects of the study did not have a history of any reproductive disease. Subjects of all three groups were age-matched; HP, RM, and NP women had age means of 29 ± 5.21, 28.1 ± 4.63, and 28.6 ± 4.91 yr, respectively. The gestational age of RM patients at the time of abortion was 12.6 ± 3.40 weeks (range, 6-19), and had an average of 3.6 abortions (range, 3-5). Average hemoglobin values of 11.9 ± 1.38 g/dL (range, 8.62-13.9 g/dL), 13.3 ± 1.51 g/dL (range, 12.3-14.8 g/dL), and 14.2 ± 1.73 g/dL (range, 12.1-15.1 g/dL) were obtained for RM, HP, and NP women respectively. Blood and placental tissue samples were obtained from the HP and RM subjects just shortly post-delivery or at the time of abortion.
Sample collection and preparation
Venous blood samples were taken from subjects into chilled tubes conditioning EDTA for the assay of all studied parameters, or into polyethylene terephthalate tubes for Se determination. Plasma was immediately obtained by whole blood centrifugation at 4℃ and 3,000 g for 20 min, and samples were frozen at -80℃ until time of analysis. A blood cell suspension was prepared by mixing whole blood (3 mL), with cold 4℃ isotonic saline (3 mL, NaCl 9 g/L) followed by centrifugation at 1,000 g for 5 min. This procedure was repeated three times and the final cell wash was diluted 1:2 with isotonic saline. A blood hemolysate was prepared by adding deionized water (4 mL) to the cell suspension (1 mL), and the mixture was frozen and thawed three times in a solid CO2/ethanol mixture. Samples were then stored at -80℃ until time of analysis. Full depth placental tissue samples were collected, and the decidua basalis and the chorionic plate were trimmed off, leaving trophoblastic tissue. The tissues were then washed in 0.1 M phosphate buffered saline to remove maternal blood and immediately stored in liquid nitrogen at -80℃. Prior to analysis, placental tissue fragments (1.5 g), were homogenized in 0.1 M potassium chloride and centrifuged at 4℃ and 10,000 g for 10 min. Supernatants were used for different assays. Se, GSH and GSSG analysis required special sample preparations which are described below.
Enzyme assays
GPx activity in all samples was determined as described by us elsewhere (5). Briefly 1:10 diluted plasma (50 µL), whole blood hemolysate (50 µL) or placental tissue supernatant (50 µL), were added to the assay solution (800 µL) containing 50 mM tris-HCl buffer pH 7.6, 1 mM EDTA, 1 IU GR, 0.25 mM GSH and 0.2 mM NADPH. After a 5 min pre-incubation, the reaction was initiat ed by the addition of 15 mM H2O2 (100 µL). The decrease in absorbance was then monitored for 30 min at 340 nm. GPx activity was calculated as the amount of enzyme capable of catalysing the oxidation of 1 µmole or 1 nmole of GSH/minute. CAT activity in all samples was determined according to Aebi (28). The decomposition of H2O2 (µmole/mL or nmole/mg), was directly followed by monitoring the decrease in absorbance at 240 nm. The assay was initiated by the addition of sample or appropriately diluted H2O2 stock solution. GR activity in all samples was determined by a modification of the method of Carlberg and Mannervik (29). Sample (100 µL) was added to a reaction mixture (2 mL) containing 100 mM potassium phosphate buffer (pH 7.4), 80 mM EDTA, 2 mM NADPH, 0.3 mM flavine adenine dinucleotide, incubated for 2 min and the reaction initiated by addition of 7.5 mM GSSG. The reaction was then monitored at 340 nm for 2 min. One unit of GR activity was equal to the amount of enzyme required for the reduction of 1 µmole or 1 nmole of NADPH/minute at 25℃.
Se assay
The Se assay procedure required special preparation of samples. All samples were freeze-dried at -45℃ and pulverized. Samples were digested with ultra-pure nitric acid (0.5 mL, 68%) and H2O2 (0.2 mL, 35%). Clear and colorless digests were appropriately diluted using ultra-pure water and assayed for Se by Inductively Coupled Plasma Mass Spectrometry (ICP-MS, HP 4500, Yokokawa Electric Co., Japan) as described by Osada et al. (30). Analytical accuracy was examined using standards purchased from the National Institute of Standards and Technology, Gaithersberg, MD, USA.
Lipid peroxidation
Lipid peroxidation was measured by determining the level of MDA using thiobarbituric acid (31). In brief, plasma (150 µL), whole blood hemolysate (150 µL) or placental tissue supernatant (1 mL), were added to trichloroacetic acid (1 mL, 17.5%) and thiobarbituric acid (1 mL, 0.6%). The mixture was incubated at 100℃ for 15 min and allowed to cool. Trichloroacetic acid (1 mL, 70%) was then added to the mixture, left standing at room temperature for 20 min and centrifuged at 2,000 rpm for 15 min. The supernatant was removed and the absorbance measured at 535 nm. MDA concentration was calculated using an extinction coefficient of 1.56×105/M/cm.
GSH and GSSG
GSH and GSSG determination in whole blood required special sample preparation. Whole blood was collected into EDTA tubes using a butterfly needle to prevent oxidation and hemolysis. Blood (30 µL), was then centrifuged and GSH was released from cells by protein precipitation and cellular disruption using 5-sulphosalicylic acid (33.3 µL, 1 g/mL). Samples were then diluted using sodium phosphate buffer (pH 7.5, 936.7 µL), centrifuged at 13,000 rpm for 5 min and supernatants stored at -80℃ until analysis. The GSH level in all samples was measured by the glutathione reductase-DTNB (5,5 dithiobis-2-nitrobenzoic acid) recycling procedure as documented elsewhere (32). The assay mixture contained 100 mM sodium phosphate buffer (150 µL, pH 7.4), 8 mM EDTA (50 µL), DNTB solution (50 µL), and 2 mM NADPH (100 µL). GSH standards (20-80 µM) and samples (25 µL) were then added and the tubes incubated at 37℃ for 3 min. Finally glutathione reductase (25 µL) was added and absorbance was monitored at 410 nm. For the GSSG assay the reaction mixture was the same as described above and additionally contained triethanolamine to prevent a high local pH and oxidation, and 2-vinyl pyridine for GSH derivitisation. GSSG standards (0-10 µM) were then run in parallel.
H2O2 assay
The H2O2 level in all samples was determined by a modification of the procedure described by Zhou et al. (33). In the presence of peroxide, the Amplex Red Reagent (ARR, 10-acetyl-3,7-dihydrophenoxazine) reacts with H2O2 to form the red fluorescent oxidation products resorufin. Reaction mixtures containing peroxidase dissolved in Kreb's Ringer buffer (10 U/mL, 100 µL), sodium phosphate reaction buffer (50 mM, pH 7.4) and appropriately diluted standards and samples (50 µL), were incubated for 30 min at room temperature. The reaction was initiated by addition of ARR (10 mM, 50 µL) and fluorescence was measured using an excitation λ of 530 nm and an emission λ of 530 nm and an emission λ of 590 nm. Standard H2O2 solutions ranged in concentration from 0-15 µM.
Other assays and statistical analysis
Total protein content of samples (20 µL) was assayed according to Bradford (34). Drabkin's reagent was used to measure hemoglobin concentration in blood hemolysates using the assay kit MAK 115 purchased from Sigma-Aldrich (St. Louis, MO, USA). Ferricyanide oxidizes the iron in hemoglobin thereby changing it to methemoglobin which binds with potassium cyanide to form cyanmethemoglobin that absorbs light at 540 nm.
Statistical analysis was performed using the computer based package of statistical product and service solution (SPSS version 9.0). Sample analysis was run in duplicate for all investigated parameters and results presented as means±SD. Values of the activities and concentrations of individual parameters were compared between different groups of the study subjects using one-way analysis of variance (ANOVA) followed by the post hoc Tukey-HSD test for multiple comparisons. Values of P<0.05 were considered to be statistically significant.
Ethics statement
The study protocol was ethically approved by the institutional review board of the College of Medicine and King Khalid University Hospital, King Saud University (project # E-13-920 and approval letter # 14/4001/IRB dated 1st June 2014). Written informed consent was obtained from each of the subjects of the study.
RESULTS
GPx, CAT and GR activities and Se levels in plasma, whole blood and placental tissue of NP, HP, and RM women
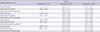
As evident from Table 1 data, GPx plasma and whole blood activities in HP women were slightly lower (0.82±0.11 U/L and 18.1±2.11 U/g Hb respectively), and much more significantly lower in RM patients (0.71±0.10 U/L and 11.2±1.48 U/g Hb respectively), when both were compared to the enzyme activities documented for NP women (0.9±0.12 U/L and 19.6±2.38 U/g Hb respectively, P<0.05 and P<0.001). Furthermore, whereas, GPx plasma activity was significantly lower in plasma of RM patients (0.71±0.10 U/L) when compared to that in HP women (0.82±0.11 U/L, P<0.001), it was much more significantly lower in whole blood of the same patients when compared to HP women (11.2±1.48 against 18.1±2.11 U/g Hb, P<0.001). A similar reduction in the enzyme's activity in placental tissue of RM patients was noted on comparison with that obtained in HP women (0.14±0.02 against 0.26±0.03 U/mg protein, P<0.001). Similar to GPx, CAT plasma and whole blood activities in HP women were slightly significantly lower (1.45±0.16 U/L and 29.6±3.18 U/g Hb, respectively), and much more significantly lower in RM patients (1.29±0.15 U/L and 15.8±2.19 U/g Hb respectively), when both were compared to the enzyme's activities noted for NP women (1.58±0.16 U/L and 31.8±3.24 U/g Hb respectively, P<0.05 and P<0.001). In addition, whereas CAT plasma activity was significantly lower in plasma of RM patients (1.29±0.15 U/L) when compared to its activity in HP women (1.45±0.16 U/L, P<0.001), its activity in whole blood of RM patients (15.8±2.19 U/g Hb) was much more significantly lower compared to that noted in HP women (29.6±3.18 U/g Hb, P<0.001). Similarly placental tissue CAT activity of RM patients (0.34±0.05 U/mg protein) was very significantly lower when compared to that of HP women (0.57±0.06 U/mg protein, P<0.001). As also evident from Table 1, plasma and whole blood GR activities in HP women underwent moderate decreases (1.83±0.26 U/L and 38.8 U/g Hb, respectively), and much more significant decreases in RM patients (1.59±0.20 U/L and 25.0±3.26 U/g Hb respectively) when both were compared to the activities recorded for NP women (2.05±0.29 U/L and 42.6±6.31 U/g Hb respectively, P<0.05 and P<0.001). In addition, whereas GR plasma activity was significantly lower in RM patients (1.59±0.20 U/L) when compared to that in HP women (1.83±0.26 U/L, P<0.001), it was much more significantly lower in whole blood of the same patients when compared to HP women (25.0±3.26 against 38.8±5.28 U/g Hb, P<0.001). A similar reduction in placental tissue GR activity of RM patients was noted on comparison with that obtained for HP women (0.36±0.05 against 0.75±0.10 U/mg protein, P<0.001).
Concurrent with the above lowered GPx, CAT and GR activities, reductions in Se plasma, whole blood and placental tissue levels were noted (Table 1). Whereas the plasma and whole blood Se levels of HP women were slightly lowered (87.6±12.6 and 115.2±14.1 µg/L, respectively), the levels were much more significantly lowered in RM patients (75.3±11.2 and 74.8±9.91 µg/L, respectively) when both were compared to those documented for NP women (96.3±13.5 and 125.8±15.7 µg/L respectively, P<0.05 and P<0.001). Furthermore, although plasma Se levels were significantly lower in RM patients (75.3±11.2 µg/L) when compared with those in HP women (87.6±12.6 µg/L, P<0.001) the whole blood Se levels of RM patients (74.8 ±9.91 µg/L) were much more significantly lower than those for HP women (115.2±14.1 µg/L, P<0.001). Similarly the placental tissue Se levels of RM patients were very significantly lower (9.67±1.32 nmole/g) when compared to those obtained for HP women (15.5±1.91 nmole/g, P<0.001).
H2O2 and MDA levels in plasma, whole blood and placental tissue of NP, HP, and RM women
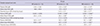
It is clear from Table 2 data that H2O2 levels were slightly increased in plasma and whole blood of HP women (6.70±0.70 and 8.51±0.91 pM, respectively), and much more significantly in RM patients (7.40±0.70 and 13.1±1.72 pM, respectively) when compared to those obtained for NP women (6.20±0.70 and 7.90±0.90 pM respectively, P<0.05 and P<0.001). In addition although plasma H2O2 levels were significantly increased in RM patients (7.40±0.70 pM) when compared with those in HP women (6.70±0.70 pM, P<0.001), the whole blood H2O2 levels of the same patients were much more significantly increased (13.1±1.72 pM) when compared to HP women (8.51±0.91 pM, P<0.001). Similarly, the placental tissue H2O2 generation rates of RM patients (3.94±0.53 nmol/min/mg tissue) were very significantly increased when compared to those obtained for HP women (2.20±0.30 nmol/min/mg tissue, P<0.001). Table 2 data also show that the levels of MDA production, were slightly increased in plasma and whole blood of HP women (5.12±0.81 and 7.31±1.10 pM, respectively, and underwent much more significant increases (5.95±0.91 and 11.4±1.56 pM respectively), in RM patients when both were compared with those noted for NP women (4.58±0.79 and 6.61±0.94 pM respectively, P<0.05 and P<0.001). Furthermore, although the plasma MDA levels were significantly increased in RM patients (5.95±0.91 pM) when compared to those in HP women (5.12±0.81 pM, P<0.001), the whole blood levels of the same patients were much more significantly increased (11.4±1.56 pM) when compared again with HP women (7.31±1.10 pM, P<0.001). In a similar fashion, the placental tissue MDA levels of RM patients (358±46.3 nmol/g wet weight), were very significantly increased when compared to those obtained for HP women (230±34.2 nmol/g wet weight; P<0.001).
GSH, GSSG levels and the GSH/GSSG ratio in plasma, whole blood and placental tissue of NP, HP, and RM women
As evident from Table 3 data, plasma and whole blood GSH levels underwent slight decreases in HP women (2.23±0.23 and 414±63.4 µM, respectively), and much more significant decreases in RM patients (2.02±0.19 and 351±52.0 µM respectively), when compared with those obtained for plasma and whole blood of NP women (2.43±0.26 and 459±68.6 µM, respectively, P<0.05 and<0.001). The data also shows that although plasma GSH levels were significantly lower in RM patients compared to HP women (2.02±0.19 against 2.23±0.23 µM respectively, P<0.001), whole blood GSH levels were more significantly lower in the same patients when compared to those of HP women (351±52.0 against 414±63.4 µM, respectively, P<0.001). Similarly placental tissue GSH levels in RM women (5.80±0.77 nmol/mg tissue), were very significantly lower than those noted for HP women (6.70±0.71 nmol/mg tissue, P<0.001). In contrast, Table 3 data show that plasma and whole blood GSSG levels underwent slight increases in HP women (0.048±0.006 and 69.4±8.88 µM respectively), and much more significant increases in RM patients (0.054±0.006 and 83.1±11.1 µM, respectively) when compared with those obtained for plasma and whole blood of NP women (0.043±0.005 and 63.4 ±8.16 µM respectively, P<0.05 and P<0.001). In addition, although plasma GSSG levels were significantly higher in RM patients compared to HP women (0.054±0.006 against 0.048± 0.006 µM, respectively, P<0.001), whole blood GSSG levels were more significantly higher in the same patients compared to those of HP women (83.1±11.1 against 69.4±8.88 M, P<0.001). Similarly placental tissue GSSG levels in RM patients (0.18±0.023 nmol/mg tissue) were very significantly higher than those obtained for HP women (0.12±0.016 nmol/mg tissue, P<0.001).
Consequent to the above results and as shown in Table 3, the plasma and whole blood GSH/GSSG ratio was slightly lower in HP women (48.3±5.99 and 6.01±0.78 respectively), and much more significantly lower (42.1±5.86 and 4.21±0.56 respectively) in RM patients when compared to the corresponding ratios seen in NP women (52.5±6.77 and 6.64±0.87 respectively, P<0.05 and P<0.001). The results also indicate that although the plasma GSG/GSSG ratio was significantly lower in RM patients compared to HP women (42.1±5.86 against 48.3±5.99, P<0.001), the whole blood and placental tissue ratios were more significantly lower in the same patients when compared to those of HP women (4.21±0.56 and 30.8±4.31 respectively against 6.01±0.78 and 49.8±6.12 respectively, P<0.001).
DISCUSSION
It is evident from data of the present study that there were moderate decreases in plasma and whole blood GPx, CAT, and GR activities, as well as Se and GSH levels of HP women when compared to NP women (P<0.05). These decreases however were more significant (P<0.001) in plasma, and very highly significant (P<0.001) in whole blood and placental tissue of RM patients when compared to both HP and NP women. Concurrent with the above decreases in antioxidant capacity, there were increases exactly equal in significance and similar in magnitude in plasma, whole blood and placental tissue levels of corresponding oxidants including H2O2, lipid peroxides, (measured by monitoring MDA) and GSSG in the same RM patients when compared with HP or NP women. Although all the above findings are in the broad agreement with many previously documented by other workers (161718192025262735), the latter reports investigated individual oxidants or antioxidants and mostly examined their levels in either plasma or placental tissue and rarely in whole blood. Furthermore, results were usually compared between HP and RM subjects and less often between HP, RM, and NP controls. Hence, this study is comprehensive in the sense that we investigated the levels of a large number of antioxidants representing general antioxidant capacity and their corresponding oxidants in plasma, whole blood and placental tissue of HP, RM, and NP women. What further characterizes our study is that the pattern and degree of the observed decreases in antioxidant capacity, and the increases in the rates of the corresponding oxidant formation, were always highly consistent and extremely statistically significant (P<0.001), in whole blood and placental tissue of RM patients when compared to HP women, and in plasma and whole blood of the same patients when compared to NP women.
Antioxidant and oxidant levels have been previously postulated to be useful in estimating the risk of oxidative injury (3789). Results of this study indicate that the fine balance normally maintained between ROS production and antioxidant activity, whether in plasma or intracellularly in whole blood erythrocytes and placental tissue, has shifted in favor of oxidative reactions thus causing mild tolerated OS in HP women, and a marked one in RM women. To this end, it was more recently shown that OS index levels were increased, and total antioxidant capacity was decreased in serum of RM women compared to controls (36). Although physiologic ROS levels have been shown to regulate various signaling transduction pathways in folliculogenesis, oocyte maturation, corpus luteum and uterine function and fetoplacental development (1), OS can cause cell damage and dysfunction (79). Related to this, lipid peroxidation levels have been shown to attain very high levels prior to abortion (13) leading to pregnancy loss (79). Moreover, OS has been shown to cause impairment in the development or degeneration of placental tissue leading to RM (12). Thus results of our study, as well as those mentioned above, provide sound evidence that OS must have been a major causative agent that leads to miscarriage in the patients investigated here.
Se, which is essential to GPx activity, functions as an integral part of the enzyme's protein active site. In the present study, highly significant (P<0.001) decreases in plasma, whole blood and placental tissue Se levels were observed in RM patients when compared to HP and NP women. This was coupled with a parallel drop in GPx, CAT, and GR activities of equal statistical significance and a concurrent increase in H2O2 and MDA levels of very similar magnitudes (Table 2). The effect of Se-deficiency observed here could have been a causative factor of the demonstrated decreases in GPx activity. Another contributing factor causing these highly significant decreases of GPx and all other studied antioxidant enzymes in RM patients, could have been an alteration in gene expression levels of these enzymes. In a recent separate study conducted in our laboratory (data submitted for publication), we were able to illustrate a 50% down-regulation rate in the gene expression levels of GPx, CAT, SOD, and GR in the placental tissue of RM patients when compared to HP women. Whether caused by Se deficiency or lowered gene expression levels or both, the drop in GPx and CAT activities subsequently lead to very significant increases in H2O2 and MDA levels, thus inflicting OS in blood and placental tissue of RM patients.
It is well known that the ability of cells to recycle GSH makes the redox cycle a focal antioxidant defense mechanism that maintains intracellular homeostasis and redox balance, and prevent lipid peroxidation and depletion of cellular thiols (69). In this cycle, GSH is used as co-substrate by Se-dependent GPx to decompose H2O2 as well as lipid peroxide (37) resulting in their reduction to water and the production of GSSG. GSSG is then reduced back to GSH by GR; a reaction that requires NADPH generated by glucose-6-phosphate dehydrogenase. Consequently the GSH/GSSG ratio normally maintained at a high value, represents the major cellular redox buffer and serves as an index of redox environment of cells (38). Our results indicated very significant decreases in GSH (P<0.001) and parallel increases equally significant in GSSG levels in the plasma, whole blood and placental tissue of RM patients compared to HP and NP women (Table 3). In addition, results exhibited very significant decreases of equal magnitude in GR activity of all RM patient samples when compared to HP and NP women (Table 1). These findings are in general agreement with some literature reports (2035). The presently noted decreases in RM patient's GSH levels are likely a result of the marked decreases in GR activity, or could have happened as a result of GSH reacting directly with oxidants like H2O2 which was excessively generated in all patient samples thus leading to increased GSSG formation. GSH levels are also regulated by its de novo synthesis catalysed by γ-glutamate cysteine ligase and glutathione synthetase (39), and hence the observed drop could have been a result of decreased activities of these enzymes. The activities and gene expression levels of both enzymes need to be investigated in placental tissue of RM patients. As a consequence of the above variations in GSH and GSSG concentrations, GSH/GSSG ratios were significantly lowered in plasma of RM patients (P<0.001), and much more significantly lowered (P<0.001) in whole blood and placental tissue of the same patients compared to HP and NP women (Table 3). The accumulation of ROS including H2O2, lipid peroxides and GSSG, as well as the drop in GSH/GSSG ratios, all illustrated in this study clearly indicate prevalence of enhanced OS that could have caused toxicity and alteration in the expression of genes related to antioxidants and apoptosis in RM patients thus leading to miscarriage. In a recent study, the association of polymorphism in OS-related genes with idiopathic RM has been reported (40).
In conclusion, this study has provided evidence in support of the occurrence of an imbalance between antioxidant levels and ROS generation (OS), which could be responsible for the start and progression of pathological processes related to RM. However, more studies that look into details of antioxidant expression as well as the biochemical and molecular mechanism of antioxidant capacity in RM are needed. Although reports suggest that the use of antioxidant supplements is beneficial in vitro fertilization (1), studies related to their use in preventing miscarriage are very scarce. However, since results of this study indicate enhanced OS in blood and placental tissue of RM patients, supplementary antioxidant therapy including Se, Zn, Cu, Mn, ascorbate, GSH and α-tocopherol may be beneficial to such patients during pre-conception and the first trimester post-conception.

 XML Download
XML Download