

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In cases of rare and incurable neuromuscular disease (NMD) showing progressive muscular weakness, hypercapnia occurs due to hypoventilation arising from respiratory muscle weakening as the disease progresses (12345). This ventilatory failure is accompanied by respiratory complications such as pneumonia and atelectasis, which deteriorate patients' quality of life and ultimately lead to death (67). Applying appropriate ventilatory support using a ventilator and managing the ventilatory failure status of NMD patients through regular respiratory function evaluation and ventilatory status analysis can prevent respiratory complications and resultant death and contribute to improving quality of life (689101112).
To reduce the economic burden for patients with rare and incurable NMD due to medical expense in Korea, the government has provided a ventilator rental fee for patients who require a ventilator due to paralysis of respiratory muscles from progressive muscular weakness since 2001. However, there is no management system to provide patients with professional advice and counselling on the appropriate use of ventilators and respiratory failure symptoms other than regular inspection of the devices by ventilator rental companies, and thus the necessity of improving the management of the ventilator support project has been suggested (13).
As part of the Korean government's medical expense support project for patients with rare and incurable disease, this study examined the appropriateness of ventilator usage and respiratory care for patients with NMD who receive a ventilator rental fee based on phone interviews and in-person surveys.
MATERIALS AND METHODS
Study subjects
In Korea, the following NMD are designated as ‘rare incurable diseases requiring support for respiratory care': amyotrophic lateral sclerosis (ALS), spinal muscular atrophy (SMA), muscular dystrophy, myotonic dystrophy, congenital myopathy, mitochondrial myopathy, and other muscular disorders (hereditary ataxia, myasthenia gravis, multiple sclerosis, Charcot-Marie-Tooth disease, Guillain-Barre syndrome, mucopolysaccharidosis, Pompe disease, and Creutzfeldt-Jakob disease). These patients can request ventilatory support (financial support for the rental cost of a portable ventilator and mechanical insufflation-exsufflation device) when they have more than two symptoms of chronic hypoventilation (fatigue, sleep disorder, nightmare, morning headache, anxiety and dyspnoea) and their end-tidal CO2 exceeds 40 mmHg or partial pressure of carbon dioxide (pCO2) exceeds 45 mmHg on 2 serial examinations. The research subjects were 1,251 patients with rare and incurable NMD who had registered for ventilator rental fee support from the government between February 2011 and April 2012. Among them, 259 subjects (68 subjects who returned the ventilator or died, 5 who did not use the ventilator, 62 with incorrect contact information, 19 who refused to take the survey, and 105 who could not be contacted despite more than three phone call attempts) were excluded, and 992 subjects were finally included. Except who actually did not use home mechanical ventilator (who did not use the ventilator and who returned the ventilator or died), a survey response rate was 84% (992 of 1,178).
Methods
This study involved two phone surveys and home visit surveys from February 21, 2011 to January 17, 2013 (first survey period: February 21, 2011 to December 20, 2011; second survey period: April 18, 2012 to January 17, 2013).
Organization of the research team
For the care and management of patients using a ventilator, a respiratory rehabilitation expert team, consisting of a rehabilitation medicine specialist, social worker, and research assistant nurse, was established by the Korea Centers for Disease Control and Prevention. The rehabilitation medicine specialist was responsible for medical consulting and advice for patients during phone counselling and home visits and for educating the social worker and nurse on the methods of respiratory failure patient care and evaluation. The social worker performed phone counselling and surveys. The nurse performed phone counselling, home visits, and visit surveys.
Phone survey
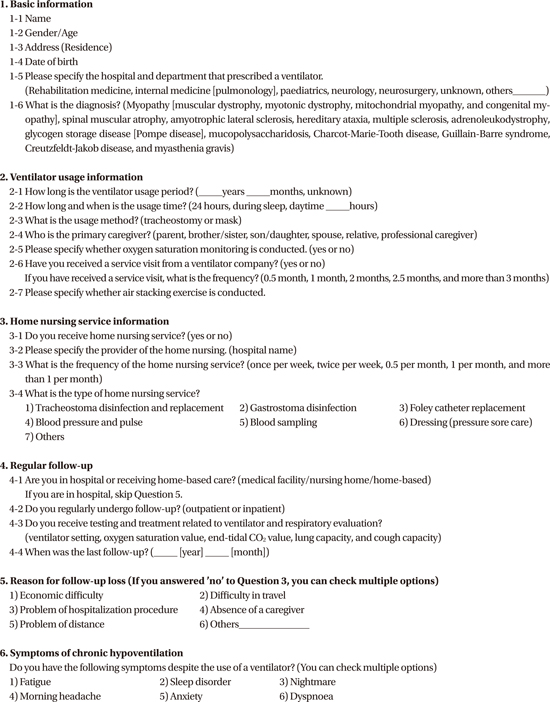
Ventilator usage information, regular follow-up observation, and chronic respiratory insufficiency symptoms were surveyed by phone (Appendix 1, visible online). Ventilator usage information included the ventilator usage period, method and the presence of oxygen saturation monitoring. For patients receiving home-based care at the time of survey, whether regular follow-up observation was conducted through hospital visits, and whether respiratory evaluation was conducted at follow-ups was examined. For patients receiving inpatient treatment, whether regular respiratory evaluation was conducted was examined. For patients receiving home-based care who did not receive follow-up observation, the reason for this absence of follow-up was also questioned. To assess the appropriateness of ventilator usage, the presence of fatigue, sleep disorder, nightmares, morning headache, anxiety, and dyspnoea, which are symptoms of chronic respiratory insufficiency, was examined, with patients able to list multiple symptoms.
Home visit
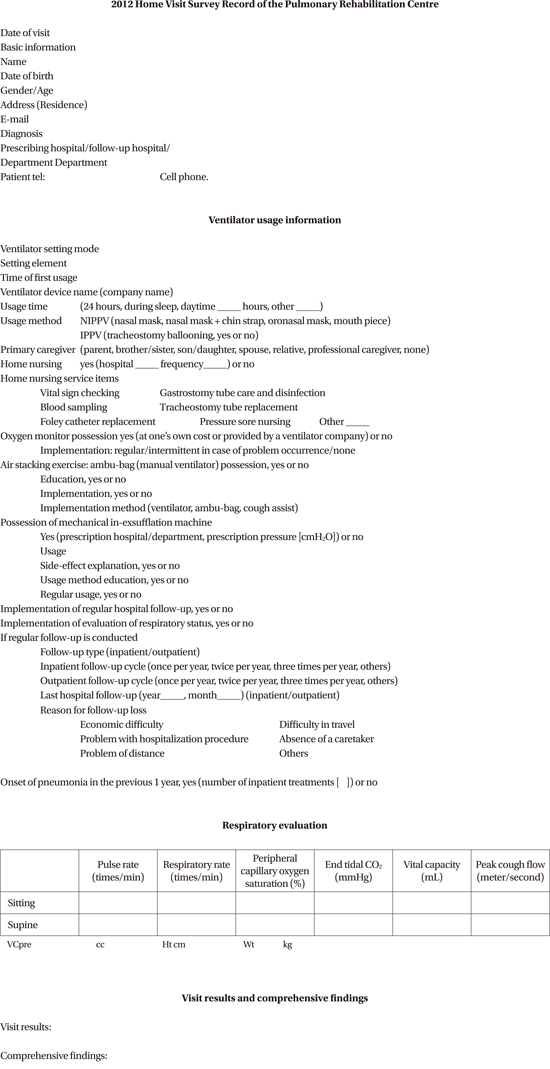
After the phone survey, a home visit was conducted for 343 subjects who required a medical assessment based on the judgment of the expert medical team (e.g., patients who had not received treatment for a long time and patients who had a limitation in prompt hospital treatment due to distance or difficulty in transportation, regardless of economic condition). During the home visit, the presence of abnormal ventilatory status was checked by conducting a respiratory evaluation, and a home visit survey record was made (Appendix 2, visible online).
Statistical analysis
Statistical analysis was performed by using of SPSS ver. 20.0 (SPSS, Chicago, IL, USA). The χ2 test or the Fisher exact tests depending on individual cell size was used to compare daily use time, type of ventilation of each disease, as well as abnormal ventilation status according to ventilator type or using time. P values < 0.05 were considered statistically significant.
RESULTS
Basic characteristics of subjects
Among total 992 subjects, 436 had ALS, 260 had muscular dystrophy, 161 had SMA, 34 had myotonic dystrophy, 34 had congenital myopathy, 23 had mitochondrial myopathy, 3 had unspecified primary muscular disorders, and 41 had other muscular disorders (hereditary ataxia, myasthenia gravis, multiple sclerosis, Charcot-Marie-Tooth disease, Guillain-Barre syndrome, mucopolysaccharidosis, Pompe disease, or Creutzfeldt-Jakob disease). There were 658 male subjects and 334 female subjects. Their mean age was 41.48 ± 21.83 years. Stratified according to disease diagnosis, subjects with ALS had the highest mean age (56.62 ± 11.29 years), and subjects with congenital myopathy had the lowest mean age (14.88 ± 13.83 years) (Table 1).
Table 1
Gender and age index for each disease
Ventilator usage period and daily average usage time
The duration of ventilator usage is shown in Table 2. Five hundred fifty-five subjects used a ventilator for 24 hours, 194 subjects used it during their entire sleep and “partial daytime” (for a short time when necessary, less than 15 hours), 164 subjects used it only during sleep, and 79 subjects used it only during partial daytime. The proportion of full-day application was higher than that of part-time application in subjects with ALS, SMA, and mitochondrial myopathy; in contrast, the proportion of part-time application was higher in subjects with muscular dystrophy, myotonic dystrophy, and congenital myopathy. The proportion of full-day application was significantly high in ALS group (P < 0.001), while the proportion of part-time application was significantly high in muscular dystrophy and congenital myopathy group (muscular dystrophy P < 0.001, congenital myopathy P = 0.014). The proportional difference of full-time applying patients to part-time applying patients was not significant in other diseases. (Table 3, Fig. 1).
Table 2
Duration of ventilator use for each disease
Table 3
Average time of the daily ventilator use for each disease
Fig. 1
Percentage of time of the daily ventilator use for each disease.
ALS, amyotrophic lateral sclerosis; SMA, spinal muscular atrophy; †This group includes hereditary ataxia, myasthenia gravis, multiple sclerosis, Charcot-Marie-Tooth disease, Guillain-Barre syndrome, mucopolysaccharidosis, Pompe disease, and Creutzfeldt-Jakob disease.
*Statistically significant P value < 0.05;

Type of ventilator usage
Invasive respiratory support (invasive positive pressure ventilation, IPPV) via tracheostomy was implemented in 530 subjects (53.4%), and noninvasive respiratory support (NIPPV, noninvasive intermittent positive pressure ventilation) through a mask was implemented in 462 subjects (46.6%). ALS group and other group had significantly higher tendency of using IPPV (P < 0.001), whereas muscular dystrophy group had higher tendency of using NIPPV (P < 0.001) (Table 4, Fig. 2).
Table 4
Ventilator usage type for each disease

ALS, amyotrophic lateral sclerosis; SMA, spinal muscular atrophy; IPPV, invasive positive pressure ventilation; NIPPV, non-invasive intermittent positive pressure ventilator.
*This group includes hereditary ataxia, myasthenia gravis, multiple sclerosis, Charcot-Marie-Tooth disease, Guillain-Barre syndrome, mucopolysaccharidosis, Pompe disease, and Creutzfeldt-Jakob disease.
Fig. 2
Percentage of type of ventilator use for each disease.
IPPV, invasive positive pressure ventilation; NIPPV, non-invasive intermittent positive pressure ventilator; ALS, amyotrophic lateral sclerosis; SMA, spinal muscular atrophy.
*Statistically significant P value < 0.05; †This group includes hereditary ataxia, myasthenia gravis, multiple sclerosis, Charcot-Marie-Tooth disease, Guillain-Barre syndrome, mucopolysaccharidosis, Pompe disease, and Creutzfeldt-Jakob disease.

Possession of oxygen saturation monitor and implementation of air stacking exercise
Four hundred fifty-eight of 992 subjects (46.2%) had an oxygen saturation monitor, and 30.7% of subjects (n = 305) performed air stacking exercise. Seventy nine of 531 (14.9%) patients using IPPV via tracheostomy and 225 of 461 (48.8%) patients using NIPPV carried out air stacking exercise.
Implementation of regular follow-up observation and respiratory evaluation
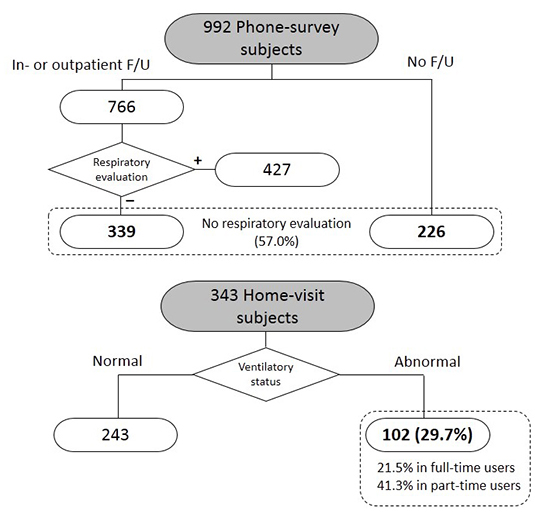
Among the 992 subjects, 605 subjects (61.0%) received follow-up in outpatients, 161 subjects (16.2%) received treatment in a hospital and 226 subjects did not receive follow-up observation. Among the 605 subjects underwent follow-up observation as outpatients, 375 subjects received regular respiratory evaluation during follow-up observation and 230 did not. Among the subjects receiving inpatient treatment, regular respiratory evaluation was implemented in only 52 of 161. In summary, 427 (43.0%) underwent respiratory evaluation during hospital visits and 565 patients (57.0%) did not (Fig. 3).

Reason for the omission of follow-up observation
For the 226 subjects who did not receive follow-up observation, the reason for the absence of follow-up was also questioned. The most common reason was difficulty in travel (172 subjects, 76.1%), followed by distance (12 subjects, 5.3%), economic difficulty (11 subjects, 4.9%), absence of a caregiver (1 subject, 0.4%), and other reasons (30 subjects, 13.3%) such as not feeling the necessity of visiting a hospital due to lack of knowledge of the disease.
Presence of chronic hypoventilation symptoms
In the phone survey of 992 subjects, 169 subjects complained of chronic hypoventilation symptoms and reported a total of 229 symptoms. The symptoms include fatigue (n = 7), sleep disorder (n = 126), nightmare (n = 2), morning headache (n = 58), anxiety (n = 1), and dyspnoea (n = 35).
Abnormal ventilatory status
Among the 343 subjects with home visit, 102 (29.7%) demonstrated abnormal respiratory status (end-tidal CO2 partial pressure over 40 mmHg or oxygen saturation under 94% with ventilator using). Among these 102 subjects, 43 demonstrated abnormal status of ventilation in spite of using a ventilator for 24 hours (Fig. 4).

In the first survey period (February 21, 2011 to December 20, 2011), we found 54 patients with abnormal ventilator status. Follow up observation of 47 subjects who could be contacted (excluding six subjects who passed away and one who could not be contacted) was done in the second survey period (April 18, 2012 to January 17, 2013). Thirty nine patients (83%) changed their type of ventilator usage by visiting a hospital upon the recommendation of the research nurse following the home visit.
Among the 343 patients, 3 patients were not evaluated due to ventilator malfunction. Out of 207 patients on pressure-preset mode, 55 patients (26.6%) were presented with respiratory failure. Out of 133 patients on volume-preset mode, 47 patients (35.3%) showed respiratory failure. Respiratory failure did not show significant difference among different ventilator preset mode (P = 0.091). Out of 206 patients under IPPV, 50 patients were presented with respiratory failure (24.3%). Meanwhile, out of 137 patients under NIPPV, 52 patients (38.0%) showed respiratory failure. Respiratory failure was noticed significantly more in patients under non-invasive mode compared to those under invasive method (P = 0.007).
DISCUSSION
The present study reveals high rates of chronic respiratory insufficiency symptoms, abnormal ventilator status, and low rates of regular follow-up, indicating that financial support does not help achieve sufficient ventilator care for NMD patients. These findings suggest that a new method such as the establishment of a home visit service is needed for the continuous care of patients for whom hospital treatment is difficult.
In our study, overall follow-up rate of total patients was 77.2%. This was similar to the follow up rate of Canada National survey which studied whole population under home mechanical ventilator use (CaNuVENT Group) (14). However, the survey results showed that 339 (44.3%) of the 766 subjects who received follow-up observation did not receive respiratory evaluation. Including the subjects who did not receive follow-up observation, more than half of all subjects (n = 565, 57.0%) did not receive regular respiratory evaluation. Overall, 38.0% of the subjects who received home-based care and implemented follow-up observation as outpatients (230 of 605 subjects) and 32.3% of hospitalized subjects (52 of 161 subjects) did not receive regular respiratory evaluation. Thus, a high proportion of subjects did not receive respiratory evaluation regardless of home-based care or hospitalization.
Ventilatory status of NMD patients undergoes sustained changes due to progressive weakness of respiratory muscles. Notably in the case of young patients, ventilation status also changes due to growth. The survey of home-visit subjects indicated a high rate of abnormal ventilatory status (29.7%). This rate is consistent with previous study showing home mechanical ventilator failure in 30%. However, this was due to incorrect use rather than equipment failure. If the setting of a ventilator is based on a single evaluation, effective ventilatory support would be difficult and get worse as time passes. Therefore, continuous and regular respiratory evaluation and relevant care (e.g., changing the ventilator setting and usage time) are essential and the system that checks and manages appropriate ventilator use through regular respiratory evaluation, rather than simply prescribing a ventilator, is needed.
Survey results indicated that 556 of the total 992 subjects (56%) used a ventilator for 24 hours, indicating high dependence. Oxygen saturation monitoring, which can detect symptoms of a ventilator problem, is especially important when ventilator dependence is high. However, only 458 subjects (46%) had an oxygen saturation monitoring device. In addition, air stacking exercise is known to reduce respiratory complications by significantly increasing maximal insufflation capacity and assisted peak cough flow (1516). It also improves the quality of life of terminal NMD patients who use a noninvasive ventilator by delaying the time to conversion to an invasive ventilator through tracheostomy or intubation. However, this exercise was implemented by only 305 subjects (31%). Thus, it appears that education on the importance of oxygen saturation monitoring and air stacking exercise and additional care for patients were insufficient, suggesting that a management system that can provide advice and counselling on respiratory failure symptoms as well as the use and management of a ventilator is required.
Among the 992 subjects who participated in this study, 831 (83.8%) received home-based care, and 231 (23.3%) had used a ventilator for more than 5 years. This finding was similar to previous reports on long term use of ventilator among patients with neuromuscular diseases (1718). For most NMD patients who require long-term respiratory support, ventilator support can improve the quality of life of patients and caregivers and reduce unnecessary medical expense, because patients need not receive inpatient treatment simply for the use of a ventilator. However, the results of this study indicate that sufficient respiratory care was not achieved simply through the voluntary hospital visits of patients. We recommended the subjects with abnormal ventilatory status to take a proper care for appropriate use of the ventilator when we found them through the home visit in the first survey period. In the second period, we checked them again. Consequently, 83% of them changed their ventilator setting appropriately by visiting a hospital. In other words, simply providing economic support for ventilator usage was insufficient for achieving appropriate respiration in patients, while a comprehensive management system could ensure that more patients receive proper treatment.
The percentage of patients under IPPV varied among different countries. The percentage of patients under IPPV in Eurovent study was 24% and was only 18% in Sweden, whereas in Germany it was 50%, and 35% in Denmark (18). In Australia and New Zealand, the percentage was only 3% (19). In this study, the percentage of patients under IPPV was 53.4%, higher than in any other previous studies. Eurovent study explains that these differences most likely reflect local and national practices. Adding to this, we suggest that the different proportion of neuromuscular diseases among countries may affect the different percentage of patients under IPPV. Patients with ALS showed higher proportion of those under IPPV, consistent with findings in the study from CaNuVENT group (14). Unlike other neuromuscular diseases, bulbar dysfunction develops in ALS as the disease progresses. Once reaching the critical level, tracheostomy is inevitable for non-invasive muscle aids become inadequate (2021). On the other hand, patients with muscular dystrophy revealed higher proportion of those under NIPPV. This is also consistent with previous studies, which have already shown that tracheostomy is unnecessary in these patients (2223). Since our study shows higher proportion of ALS than other neuromuscular diseases, we could guess that the proportion of patients under IPPV is high as well.
We would also like to stress on importance of frequent pulmonary evaluation. Higher tendency of respiratory failure was noticed among patients under NIPPV compared to those under IPPV in this study. Ironically, NIPPV is known to enable oral diet, speech, and improve quality of life (2425). Thus we recommend getting more frequent monitoring when maintaining NIPPV.
The major limitation of this study is that not all patients were evaluated at home. However, survey response rate was 84%, similar to that of previous studies. It was 79% in Eurovent survey (18), 89% in CaNuVENT survey (14), and in 82% in Australia and New Zealand (19). Unlike previous studies, however, this study is unique in that 1/3 of the patients were visited and evaluated by medical team.
In the future, the effects of the operation of the central management centre on patient status should be surveyed based on the currently established cohort. An efficient method for improving patients' hospital access also requires further study.
In conclusion, the efficiency of the ventilator support project could be maximized, and the social and medical cost reduced, by the implementation of a management system that can link monitoring of the appropriateness of ventilator usage, counselling and advice, and home visits for patients who receive ventilator support to establish proper treatment.
 XML Download
XML Download