

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Cataract is the leading cause of blindness in the world, accounting for half of blindness and affecting about 20 million people (1). Although cataract surgery is an effective method for restoring vision, individuals in developing countries have limited access to cataract surgery services. In addition, cataract is also one of the major socioeconomic and public health burdens, even in developed countries. This is because the volume of cataract surgery has increased due to an aging population and an increase in cataract surgery services (2). Hence, estimating the prevalence and clinical determinants of both cataract and cataract surgery is important for establishing a public health plan, identifying modifiable determinants, and minimizing the public health burden. Furthermore, investigating estimates of both cataract and cataract surgery simultaneously may provide clues for their association and unmet needs for health care. However, despite the socioeconomic and public health burden of cataract and cataract surgery, epidemiologic studies representing a nationwide population have been scarce.
Korea is one of the newly developed countries in Asia and one of the most populous countries in the world. As the issue of an aging population has been on the rise in Korea, as well as in other developed countries, several nationwide, government-led surveys have been conducted. The Korea National Health and Nutrition Examination Survey (KNHANES) is one of these national surveys; it was initiated in 1998 and publishes nationally representative estimates for approximately 50 million Koreans (3,4). Accompanying the 2008–2012 KNHANES, the Korean Ophthalmologic Society (KOS) conducted the 5-year Korean Ophthalmic Survey. The results of the 2008–2012 KNHANES and completed Korean Ophthalmic Survey were recently released. Hence, this study estimated the prevalence of, and investigated clinical determinants for, cataract and cataract surgery in Koreans using the large-scale, nationally representative 2008–2012 KNHANES database and the Korean Ophthalmic Survey.
MATERIALS AND Methods
Study design and population
This study analyzed the 5-year (2008–2012) KNHANES data, which included the completed five-year plan ophthalmic survey designed by the KOS. The KNHANES is an ongoing, population-based, cross-sectional survey in Korea conducted by the Korea Centers for Disease Control and Prevention, and the Korean Ministry of Health and Welfare (3456). The 2008–2012 KNHANES annually selected 3,840–4,600 households in 192–200 enumeration districts representing the civilian, non-institutionalized Korean population using rolling sampling designs and involving a complex, stratified, multistage, probability-cluster survey. A total of 45,810 subjects participated in the 2008–2012 KNHANES; the response rate in each year was 77.8%, 82.8%, 81.9%, 80.4%, and 80.0% in 2008, 2009, 2010, 2011, and 2012, respectively. The KNHANES database is a publicly available database in the KNHANES homepage (https://knhanes.cdc.go.kr/, accessed on 29 December 2014), and the KNHANES introduced the database detail regarding the characteristics and the way for data resource use (3).
Data collection and inclusion criteria
The KNHANES consisted of three components, which were the Health Interview Survey, Health Examination Survey, and Nutrition Survey (3456). We used data from the first two surveys, including medical histories, socioeconomic status, anthropometric measurements, blood tests, and ophthalmic surveys (4567). The data from a structured slit-lamp examination (BQ-900; Haag-Streit AG, Koeniz, Switzerland) determined the crystalline lens/cataract status as phakia without any cataract, phakia with cataract (i.e., nuclear, cortical, anterior subcapsular, posterior subcapsular, or mixed cataract using the Lens Opacities Classification System [LOCS] III (8) as the grading system) pseudophakia and aphakia. The quality of the ophthalmic survey was verified by the Epidemiologic Survey Committee of the KOS (4567). Participants aged ≧ 40 years with slit-lamp examination of at least one eye were included in the study.
Definition of variables
The prevalence of, and determinants for, two dependent variables were separately investigated as follows: 1) the presence of cataract and 2) the evidence of cataract surgery. The presence of cataract was defined as the existence of any cataract, pseudophakia or aphakia, in at least one eye in a participant. The evidence of cataract surgery was defined as the existence of pseudophakia or aphakia in at least one eye in a participant. Independent variables were defined and categorized as follows. For each variable below, the first category in each list was selected as the reference point for logistic regression analysis (LRA). Participants were divided into four age groups, which were 40–49, 50–59, 60–69, and ≥ 70 years. Smoking status was defined as never-smoker, ex-smoker, and current smoker. Household income status was divided into participants with > 50% household income and those with ≤ 50% household income according to the equivalized annual gross household income. Education status was divided into participants with at least a high school degree and those who had graduated from middle school or less. Occupation was categorized as blue collar (agriculture, forestry, fishery workers, craft and related trade workers, plant and machine operators and assemblers, and simple labor), white collar (managers, professionals, clerks, and service/sales workers), and inoccupation (unemployed, retired, students, and housewives). Residence was categorized into urban and rural areas based on participants’ addresses. Sun-exposure status was divided into participants with an average of < 5 hours/day and those with ≥ 5 hours/day. Co-morbidities were categorized into participants without a history of co-morbidities and those with a history of co-morbidities. Co-morbidities used in LRAs were as follows: hypertension, diabetes mellitus (DM), dyslipidemia, stroke, myocardial infarction (MI) or ischemic heart disease (IHD), osteoarthritis (OA) or rheumatoid arthritis (RA), pulmonary tuberculosis, and asthma. Participants were categorized into two groups by body mass index (BMI), the ratio of weight (kg) to height2 (m2): those with BMI < 25 kg/m2 and those with BMI ≥ 25 kg/m2. Waist circumference (WC) was measured to the nearest 0.1 cm at the narrowest point between the lower borders of the rib cage and iliac crest after normal expiration. Participants were divided into those with WC < 90 cm in men or WC < 80 cm in women and those with WC ≥ 90 cm in men or ≥ 80 cm in women. Hemoglobin was measured with an XE-2100D (Sysmex, Kobe, Japan), and participants with a hemoglobin level < 13 g/dL in men or < 12 g/dL in women were designated anemic.
Statistical analysis
The data were analyzed with SAS, version 9.2 (SAS Institute INC., Cary, NC, USA) using PROC SURVEY procedures. We used the KNHANES sample weight adjusted for oversampling, non-response, and the Korean Population in 2008–2012 (3,4). The standard errors of estimates were calculated. Characteristics of participants included and excluded from the study were compared.
The prevalence of cataract and cataract surgery, including age group- and sex-specific prevalence, was estimated. Differences in the prevalence between sexes were estimated by the chi-square test. Simple LRAs were conducted to investigate associations between cataract and a set of independent variables. Age-group-, sex-, and smoking-status-adjusted (ASS-adjusted) LRAs were subsequently performed. Covariates with a P value < 0.100 in each ASS-adjusted LRA were chosen for the multiple LRA. Age group, sex, and smoking status were always included in the multiple LRA, regardless of P values. The same set of analyses was also conducted for cataract surgery by estimating prevalence and determinants compared to 1) participants without any cataract surgery and 2) participants having a cataract in at least one eye but without any cataract surgery. Odds ratio (OR) and 95% confidence interval (CI) values were calculated for all LRAs. P values < 0.05 were considered statistically significant.
Results
A total of 20,419 eligible subjects aged ≥ 40 years (8,777 men and 11,642 women) participated in KNHANES during the study period. Of these participants, 19,953 participants had slit-lamp examination data regarding the cataract state of at least one eye. Comparisons between participants with and without the examination data are provided in Supplementary Table S1.
Prevalence of cataract and cataract surgery
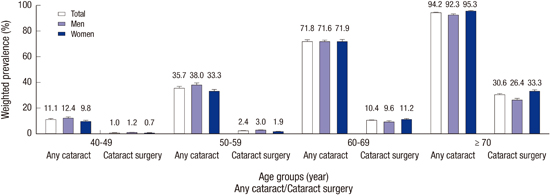
The overall prevalence of cataract was 42.28% (95% CI, 40.67–43.89); 40.82% (95% CI, 38.97–42.66) for men and 43.62% (95% CI, 41.91–45.33) for women (P = 0.606). The overall prevalence of cataract surgery was 7.75% (95% CI, 7.30–8.20); 6.38% (95% CI, 5.80–6.96) for men and 9.01% (95% CI, 8.41–9.61) for women (P < 0.001). Detailed sex- and age group-based prevalence can be seen in Table 1 and Fig. 1.
Table 1
Weighted prevalences and frequencies of participants with any cataract (including cataract surgery) in at least one eye and participants with cataract surgery in at least one eye in the Korean population aged ≥ 40 years during the 5-year study period (2008–2012)
![]()

Clinical determinants of cataract
Results of the simple LRA are provided in Supplementary Table S2. Variables with a P value < 0.100 in ASS-adjusted LRAs were age group, household income, education, occupation, hypertension, DM, dyslipidemia, and OA or RA. In multiple LRA, cataract were associated with older age (P < 0.001), men (P = 0.032), lower household income (P = 0.031), lower education (P < 0.001), hypertension (P < 0.001), and DM (P < 0.001). Detailed demographic results for each variable, ASS-adjusted LRAs, and multiple LRA are provided in Table 2.
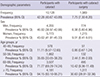
Table 2
Comparison of characteristics of participants with cataracts (including cataract surgery) and without cataracts in at least one eye and its clinical determinants using logistic regression analyses (LRAs) from the 5-year data of the KNHANES (2008–2012)

KNHANES, Korean National Health and Nutrition Examination Survey; Unadjusted, unadjusted simple logistic regression analysis; Adjusted, age groups, sex, and smoking status-adjusted logistic regression analysis; OR, odds ratio; CI, confidence interval; Never, never-smoker; Ex, ex-smoker; Current, current smoker; DM, diabetes mellitus; MI, myocardial infarction; IHD, ischemic heart disease; OA, osteoarthritis; RA, rheumatoid arthritis; Tb, tuberculosis; BMI, body mass index; WC, waist circumference; HBsAg, hepatitis B surface antigen; NA, Not Applicable.
![]()
Clinical determinants of cataract surgery
Participants with cataract surgery vs. participants without any cataract surgery
Results of simple LRA are provided in Supplementary Table S2. Variables with a P value < 0.100 in ASS-adjusted LRAs were age group, sex, smoking status, occupation, residence, sun exposure, hypertension, DM, dyslipidemia, MI or IHD, OA or RA, asthma, and anemia. In multiple LRA, cataract surgery was associated with older age (P < 0.001), occupation (P < 0.001), hypertension (P = 0.011), DM (P < 0.001), OA or RA (P = 0.044), asthma (P = 0.030), and anemia (P < 0.001). Detailed demographic results for each variable, ASS-adjusted LRAs, and multiple LRA are provided in Table 3.
Table 3
Comparison of characteristics of participants with or without cataract surgery in at least one eye and its clinical determinants using logistic regression analyses (LRAs) from the 5-year data of the KNHANES (2008–2012)

KNHANES, Korean National Health and Nutrition Examination Survey; Unadjusted, unadjusted simple logistic regression analysis; Adjusted, age groups, sex, and smoking status-adjusted logistic regression analysis; OR, odds ratio; CI, confidence interval; Never, never-smoker; Ex, ex-smoker; Current, current smoker; DM, diabetes mellitus; MI, myocardial infarction; IHD, ischemic heart disease; OA, osteoarthritis; RA, rheumatoid arthritis; Tb, tuberculosis; BMI, body mass index; WC, waist circumference; HBsAg, hepatitis B surface antigen; NA, Not Applicable.
![]()
Participants with cataract surgery vs. participants with cataract but without any cataract surgery
Variables with a P value < 0.100 in ASS-adjusted LRAs were age group, sex, smoking status, occupation, residence, sun exposure, hypertension, DM, dyslipidemia, MI or IHD, OA or RA, asthma, and anemia. In multiple LRA, cataract surgery was associated with older age (P < 0.001), occupation (P < 0.001), DM (P < 0.001), dyslipidemia (P = 0.049), asthma (P = 0.044), and anemia (P = 0.007). Detailed demographic results for each variable, ASS-adjusted LRAs, and multiple LRA are provided in Table 4.
Table 4
Comparison of characteristics of participants with cataract surgery in at least one eye to participants with cataracts but without any cataract surgery using logistic regression analyses (LRAs) from the 5-year data of the KNHANES (2008–2012)

KNHANES, Korean National Health and Nutrition Examination Survey; Unadjusted, unadjusted simple logistic regression analysis; Adjusted, age groups, sex, and smoking status-adjusted logistic regression analysis; OR, odds ratio; CI, confidence interval; Never, never-smoker; Ex, ex-smoker; Current, current smoker; DM, diabetes mellitus; MI, myocardial infarction; IHD, ischemic heart disease; OA, osteoarthritis; RA, rheumatoid arthritis; Tb, tuberculosis; BMI, body mass index; WC, waist circumference; HBsAg, hepatitis B surface antigen; NA, Not Applicable.
![]()
Discussion
This study provided detailed estimates regarding the prevalence and clinical determinants of cataract and cataract surgery based on a nationally representative database of over 20,000 participants aged ≥ 40 years. The KOS completed the five-year ophthalmic survey project in 2012, accompanying the 2008–2012 KNHANES, and the present results are reported on behalf of the KOS. Since previous epidemiologic studies for cataract and cataract surgery vary considerably across regions, racial/ethnic groups, population structures, economic status, and healthcare systems (910111213), the results of this study are expected to provide a meaningful stepping stone for future investigations and establishing a public health plan.
The prevalence of cataract in participants aged ≥ 40 years in Korea was 42.28%, but in those aged ≥ 70 years, it was > 90%. Age was the most significant determinant for cataract even in the multiple LRA, as in all previous studies (11,12,14,15). Without appropriate cataract surgery, the effect of cataract on vision in an aged population can be easily guessed (1). Historically, the association between sex and cataract has not been consistent, showing either no association (11) or a higher incidence in women (13). Differences in ethnicity, public health states, childbearing rates, and socioeconomic status may play a role in these various associations (11,12,1415161718). Interestingly, household income and education were associated with cataract, and occupation also had a marginal association (P = 0.070) with cataract. Although the underlying mechanism remains unknown, these socioeconomic determinants have also been associated with cataract in previous studies (111516). The determinants of household income, education, and occupation may be surrogate markers for nutrition status, lifestyle, and living conditions. A recent report from the Physicians’ Health Study (PHS) II showed that daily multivitamin use decreased the risk of cataract in well-nourished men of high social position (19), suggesting nutrition affects the development of cataract. Lastly, like many other studies (171820), the present study also found that hypertension and DM had a positive association with cataract. Hypertension and DM are modifiable risk factors and should be better controlled to lessen the socioeconomic and public health burden of cataract.
The current study also estimated cataract surgery in Korea. The prevalence of cataract surgery in participants aged ≥ 40 years was 7.75%, increasing to 30.63% in those ≥ 70 years. Before comparing the prevalence of cataract surgery between countries, it should be noted that Korea has several remarkable factors/barriers affecting cataract surgery, such as medical resource availability, health insurance, costs, and healthcare utilization. First, Korea has had universal health insurance coverage since 1989 (21); Koreans have paid only 30% or less of their total medical fees, including cataract examination and surgery. In addition, the National Health Insurance provides health checkup programs to all Koreans every two years, including a vision test and referral system. Second, Korea has a relatively large number (approximately 3,000) of certificated ophthalmologists, and there are over 1,100 clinics/hospitals serving small-incision cataract surgeries. Cataract surgery is the most frequent surgery in Korea, reaching 335,915–425,473 cases annually during the study period of 2008–2012. The corresponding cataract surgical rate was 7,000–8,900/million persons/year, which was one of the highest level in the world, especially considering the population structure of Korea (2223). All these statistics were from the Korean Statistical Information Service (http://kosis.kr, accessed on 1 March 2014). Lastly, in Korea, the medical fees for hospital/clinics and physicians are set by the government for cost containment (21), and Korea has one of the cheapest medical fees (approximately 1,300 USD in 2012) for cataract surgery in the world (24). Based on these characteristics, Korea is assumed one of the countries that has minimized unmet needs and barriers for cataract surgery, and the prevalence of cataract surgery should be interpreted in light of these characteristics.
In addition, this study investigated clinical determinants for cataract surgery by comparing participants in two ways. Similar to the determinants of cataract stated above, age, occupation, and DM consistently had an association with cataract surgery in both two analyses. Interestingly, in addition to these covariates, cataract surgery was consistently associated with anemia and asthma, which are novel determinants for cataract surgery found in the present study. Anemia may be associated with aging, as a pro-inflammatory state accompanies aging and may give rise to anemia (25); moreover, inflammation is the second-most cause of anemia and accounts for one-third of anemia in older persons (2627). As inflammation plays an important role in the development of cataract, it partially explains the association between anemia and cataract surgery. Inflammation may also explain, at least partially, the association between asthma and cataract surgery; this is because increased systemic inflammation is common in asthmatics (2829). In addition, inhaled corticosteroids are the recommended, preferred long-term therapy in asthma patients of all ages (30), and corticosteroids, even inhaled corticosteroids, are causally involved in cataract pathogenesis, especially in posterior subcapsular opacities, which often require early surgical treatment (31). Cataract surgery was also associated with OA or RA when analyzing all participants in the first analysis. The effect of OA or RA on cataract surgery might have been caused by the use of anti-inflammatory drugs (15). However, some studies have shown conflicting results for the association between cataract surgery and anti-inflammatory drugs (3233). Lastly, in addition to DM, hypertension and dyslipidemia were associated with cataract surgery, as they had been for cataract. Both physicians and public health experts must pay attention to these modifiable clinical determinants, including cardiovascular diseases, anemia, and asthma.
However, although it was assumed that Korea has minimized barriers and unmet needs for cataract surgery, inevitable unmet needs for cataract surgery and/or lead time bias may affect the prevalence of and determinants for cataract surgery. The patients with OA or RA, asthma, or cardiovascular diseases may be more familiar with healthcare use, resulting in earlier detection of and intervention for cataract. In addition, the results indicating lower household income and lower education were positively associated with cataract, but not with cataract surgery, suggesting the presence of possible unmet needs for cataract surgery due to socioeconomic status. Although the present study, a cross-sectional study using a pre-existing database, did not examine a causal relationship, the results of this study provide directions for further investigations into unmet needs and socioeconomic determinants for cataract surgery. Further investigations, including longitudinal and qualitative studies, are warranted.
The present study has several limitations. The KNHANES did not included institutionalized individuals, and participants with no information on cataract status were excluded. This may cause selection bias in analyzing determinants for cataract and cataract surgery, as well as underestimating the prevalence of cataract and cataract surgery. The results should be interpreted under consideration of these limitations (4). In addition, this study did not provide cataract type-specific analyses, as classified by the LOCS III, for estimating the prevalence and determinants of cataract. Since small-incision cataract surgery, which has become commonly used in Korea and developed countries, reduces the importance of the cataract subtypes and its determinants. In addition, a recent study using the three-year data of the 2008–2010 KNHANES has already reported the cataract-type specific prevalence and risk factors for each cataract subtype (34).
In conclusion, the prevalence of cataract and cataract surgery was 40.28% and 7.75% respectively in Koreans aged ≥ 40 years, suggesting 9.4 million individuals with cataract and 1.7 million individuals with cataract surgery in at least one eye. In addition to the nationally representative estimates of cataract and cataract surgery from this populous Asian country, the current study also provides clinical determinants for cataract and cataract surgery. Since cataract has emerged as a public concern and the cost burden for cataract surgery has increased with an aging population, it is expected that the present study will form a cornerstone for further investigations and the establishment of a public health plan.
 XML Download
XML Download