

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Life expectancy of male in Korea has a tendency of increase; 14.5, 11.1, and 8.2 years were estimated in an age of 70-, 75-, and 80-year respectively in 2014 (1). Because the incidence of prostate cancer increases with advancing age, it can be anticipated that the prevalence of prostate cancer in elderly men will continue to increase. Recent data shows that 64% of new cases of prostate cancer were diagnosed in men aged older than 65 years, whereas 23% were diagnosed in men aged older than 75 years (2). Nevertheless, most studies investigating optimal treatment have focused on men aged younger than 75 years (3).
Although most guidelines for prostate cancer recommend curative treatment for patients with a life expectancy of more than 10 years (456), most elderly men do not undergo radical prostatectomy (RP) regardless of their life expectancy (78). When estimating life expectancy in these patients, careful consideration should be given to their biological rather than chronological age, focusing on their general health status and the presence of comorbidities. Radical treatment may also be appropriate for elderly healthy men because this group is more likely to be diagnosed with high-risk prostate cancer and to have lower overall and cancer-specific survival rates (9101112). Several authors have shown that RP can be feasible and efficacious in carefully selected elderly patients (13141516). However, many urologists still find it difficult to advocate RP for patients aged 75 years or older because of the risks associated with surgery. Therefore, we studied whether RP was an appropriate treatment in this group of patients.
MATERIALS AND METHODS
Study design/population
We retrospectively reviewed the medical records of consecutive patients who underwent RP for prostate cancer at 6 institutions from 2005 to 2012. We evaluated the functional and oncologic outcomes for patients aged 75 years or older who underwent RP and compared them with the outcomes of patients aged 65–69 years. Most reports of age-related outcomes for prostate cancer have used cutoff ages of either 70 or 75 years (31315161718), making it difficult to categorize men aged between 70 and 75 years as either younger or older for the purpose of study. Therefore, this analysis excluded patients aged 70–75 years to avoid potential ambiguity and facilitate comparison of the outcomes. We defined the older group as those aged 75 years or older and the younger group as those aged 65–69 years. The younger group was chosen because the incidence of prostate cancer is high in that group, but there is a significant age gap compared with the older group.
Data collection and variables
We compared the following variables between the two groups: patient ages; preoperative serum prostate-specific antigen (PSA) levels; pre- and postoperative Eastern Cooperative Oncology Group (ECOG) performance statuses; underlying diseases; previous treatments; pre- and postoperative tumor characteristics; peri- and postoperative complications with functional outcomes such as urinary continence and erectile function; and postoperative treatments. The 2010 American Joint Committee on Cancer/tumor, node, metastasis (TNM) system was used for pathologic staging, and Gleason system was used for tumor grading. First postoperative serum PSA measurement was performed 1 month after RP; if the first postoperative PSA showed a nadir, routine follow-up and PSA measurement were performed every 3 months for the first year, biannually from the second to fifth years, and annually thereafter. Patients with postoperative follow-up of less than 12 months were excluded. Biochemical recurrence was defined as a serum PSA ≥ 0.2 ng/mL. We checked the ECOG performance status postoperatively at 3–6 months. Urinary continence was defined as the need for either one safety pad or no incontinence pad daily. Postoperative erectile dysfunction was diagnosed when a patient complained of new-onset difficulties in achieving an erection for intercourse.
Statistical analysis
Comparisons between groups were made using the Mann–Whitney U test for continuous variables and either the χ2 test or Fisher exact test for categorical variables. Multivariable logistic regression analysis was performed for predictors of the duration of postoperative urinary incontinence. The biochemical recurrence-free survival rates were evaluated using Kaplan–Meier survival analysis and log-rank test. All analyses were performed using IBM SPSS 18.0 (IBM Co., Armonk, NY, USA), and statistical significance was set at P value < 0.05.
RESULTS
Descriptive statistics
We reviewed the medical records of 270 consecutive patients who underwent RP for prostate cancer at 6 institutions from 2005 to 2012. Of these, we included 168 patients in the younger (65–69 years) group and 89 patients in the older (≥ 75 years) group. Surgery was conducted using an open retropubic (n = 226), laparoscopic (n = 18), or robotic (n = 26) approach, and bilateral pelvic lymph node dissection was performed in all cases with high-risk prostate cancer. Table 1 shows comparisons between patient and tumor characteristics between the two groups.
Table 1
Basic characteristics of patients according to age group

Between-group comparisons
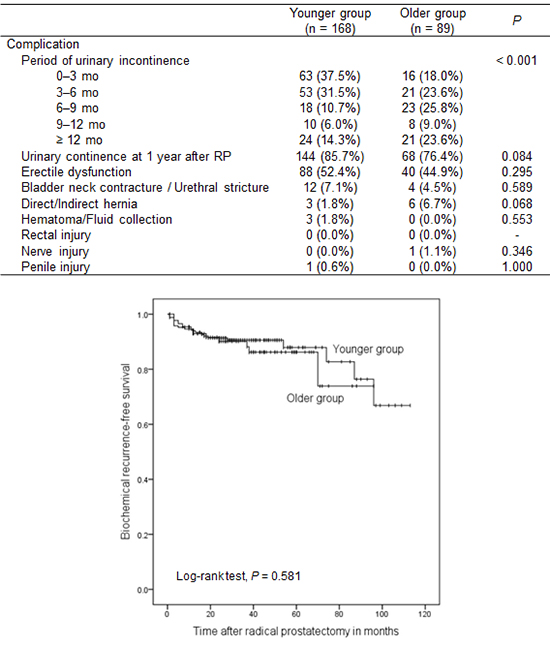
The median ages of patients undergoing RP were 67 years (IQR [inter-quartile range], 65–68) and 76 years (IQR, 75–77) in the younger and older groups, respectively. Compared with the younger group, the older group had significantly higher preoperative ECOG grade, prevalence of hypertension, and Gleason score at biopsy and RP. In addition, the older group had a higher median preoperative serum PSA level. However, there were no significant differences in the rates of diabetes mellitus, hyperlipidemia, coronary artery disease, hormone therapy, radiotherapy, and clinical or pathological stage. The peri- and postoperative clinical factors in the two groups are shown in Table 2. The median follow-up periods after RP were 36 months (IQR, 25–51) and 40 months (IQR, 24–55) in the younger and older groups, respectively. Postoperative ECOG performance status was significantly different between groups. However, except for urinary incontinence, no statistically significant differences were seen in peri- and postoperative complications (erectile dysfunction, bladder neck contracture or urethral stricture, hernia, hematoma or fluid collection, and rectal or nerve or penile injury) between groups. At 3 months after RP, 37.5% in the younger group and 18.0% in the older group were continent; by 12 months, these figures reached 85.7% and 76.4%, respectively (P < 0.001).
Table 2
Perioperative and postoperative clinical factors according to age group

Multivariable and survival analyses
In multivariable logistic regression analysis, the following factors affected urinary incontinence beyond 3 months after RP: age ≥ 75 years (Odds ratio [OR] 2.35, P = 0.016), preoperative ECOG grade ≥ 1 (OR 7.01, P < 0.001), and postoperative erectile dysfunction (OR 1.95, P = 0.031). No other factors like preoperative serum PSA level, underlying diseases (diabetes mellitus, hypertension, hyperlipidemia, and coronary artery disease), neoadjuvant hormone therapy, and pathologic stage or RP Gleason score were shown to be a predictor for urinary incontinence (Table 3).
Table 3
Multivariable analysis for predicting the duration of postoperative urinary incontinence (≥ 3 vs. 0–3 months)
Fig. 1 shows the Kaplan–Meier curves for biochemical recurrence-free survival. In the log-rank test, there was no significant difference in biochemical recurrence-free survival (P = 0.581).

DISCUSSION
We aimed to prove that RP was feasible for elderly men with prostate cancer by assessing the complication rates and functional and oncologic outcomes in comparison with a younger cohort. To this end, we found no significant differences between the younger and older groups in the rates of either general perioperative complications or postoperative erectile dysfunction. Moreover, although urinary incontinence was more common in the older group, multivariable regression analysis demonstrated that preoperative ECOG grade ≥ 1 (OR 7.01, P < 0.001) was more relevant to the development of urinary incontinence at 3 months than was patient age 75 years or older (OR 2.35, P = 0.016). These results suggested that a biological rather than chronological age in the general health status and the presence of comorbidities, was more important factor to predict the urinary incontinence. In addition, the urinary continence rates at 1 year after RP were comparable (85.7% for the younger group vs. 76.4% for the older group at 12 months, P = 0.084), despite slower recovery of urinary continence among the older group, which was probably related to the differences in ECOG performance statuses (Table 2). Finally, biochemical recurrence-free survival rates were comparable between the groups despite higher preoperative PSA levels and Gleason scores. Thus, our data support curative surgery by RP in patients aged 75 years or older.
There is ongoing discussion as to how aggressively prostate cancer should be treated in the elderly. For attempted curative treatment strategies, most authorities recommend that patients have a life expectancy of at least 10 years (456). Consequently, age has become an important factor influencing treatment decisions, with older patients less likely to receive curative treatment (19). Alibhai et al. (20) argued that the age may be improperly weighed when treating men with localized prostate cancer, reporting that younger patients with shorter life expectancies (because of serious comorbidity) tended to be offered curative treatment, whereas men older than 70 years with good life expectancy were not offered similar treatment. The National Comprehensive Cancer Network guidelines (version 1. 2015) for the treatment of localized prostate cancer recommend the use of Social Security Administration tables for the assessment of life expectancy. This provides for an adjustment of 50% upwards for elderly men in the best quartile of health, producing a life expectancy of 15.89 years for a healthy man aged 75 years. Given that life expectancy is increasing, it seems logical that the age at which patients can receive curative therapy should also be higher.
Older men are more likely to be diagnosed with high-risk prostate cancer and to have lower overall and cancer-specific survival rates (9101112). Some authors have shown that patients who receive watchful waiting for prostate cancer have increased disease-related mortality in the presence of high-grade tumors (21). The mortality from prostate cancer in men aged 70–74 years increases with the Gleason scores; from 7% for a Gleason score of 2–4 to 60% for a Gleason score of 8–10 (21). Some reports have found that more than 15% of men older than 75 years with high-risk prostate cancer were undertreated, and that most did not receive curative therapy (78). This is striking when we consider that with careful patient selection for curative local therapy, comparable gains in life expectancy can be achieved for patients up to 75 years old with Gleason scores of 5–7 and those up to 80 years old with Gleason scores of 8–10 disease (922). Therefore, high-risk prostate cancer in the elderly should be considered suitable for curative therapy.
In a previous observational study, patients with prostate cancer aged 75 years or older were more likely to be treated with primary hormone therapy (41%), external beam radiation therapy (EBRT) (21%), watchful waiting (19%) or brachytherapy (14%) rather than RP (3%) (3). For older patients with prostate cancer who are offered treatment, less invasive therapies also tend to be discussed in preference over radical surgery because of the perceived morbidity related to surgery (2324). However, radiotherapy also has important adverse effects, being shown to induce gastrointestinal and genitourinary complications, whereas hormone therapy can increase the likelihood of cardiovascular events, particularly in older men (25262728). Although RP alone and EBRT plus androgen deprivation therapy (ADT) provided similar long-term cancer control (systemic progression and cancer-specific mortality) for patients with high-risk prostate cancer, the risk of all-cause mortality was greater after EBRT plus ADT than after RP (HR 1.60, P < 0.001) (29). Thus, elderly patients with prostate cancer need not avoid RP if they can tolerate general anesthesia.
Several reports have compared the clinical outcomes of elderly people with prostate cancer after RP with those of younger patient groups. Pfitzenmaier et al. (13) evaluated the survival in patients < 70 years and ≥ 70 years who had prostate cancer and underwent RP, reporting the following 10-year survival rates: PSA-free survival of 51.8% and 57.4%, respectively; disease-specific survival, 92.3% and 97.6%; metastasis-free survival, 86.9% and 89.7%; and overall survival, 78.1% and 71.2% (P value for all the parameters > 0.05). They concluded that in a selective healthy elderly population, survival outcomes were no worse than in younger patients, and they advised that curative treatment should be recommended (13).
Similarly, Malaeb et al. (15) compared survival rates for patients aged < 50 years, 50–70 years, and ≥ 70 years and reported 5-year PSA progression-free estimates of 82%, 82%, and 65%, respectively (P = 0.349), with comparable overall and cause-specific mortalities. They suggested that the radical retropubic prostatectomy could be considered a standard treatment option for men aged ≥ 70 years with localized prostate cancer (15). Finally, Poulakis et al. (18) compared the safety and efficacy of extraperitoneal laparoscopic RP between patients aged < 60 years and those aged > 70 years. In their study, operative time, analgesic requirements, hospital stay, convalescence, and complication rates were comparable, but urinary continence at 6 months was significantly worse in the older group (91% vs. 67%, P < 0.001) (18). In our study, the older group also showed a slow recovery, but the urinary continence rates were comparable to those in the younger group by 1 year.
There were several limitations in our study. First, the arbitrary choice of an age cutoff was an important problem that is shared with other reports of age-related outcomes for prostate cancer. Usually, such reports divide patients into younger and older groups at cutoffs of 70 or 75 years. Therefore, to avoid ambiguity and aid comparison, we excluded patients aged 70–75 years. Second, the older group in our study was relatively small size when compared with the younger group. This was an inevitable problem because under current guidelines, this group is less likely to receive such treatment. Third, we did not use uniform criteria for patient selection because of the retrospective and multi-institutional design. Lastly, the average follow-up periods were relatively short (i.e., 36 and 40 months in the younger and older groups, respectively) for the investigation of survival. However, biochemical recurrence usually develops during the first 2 years of follow-up (30); therefore, should have limited influence on the validity of our data.
In conclusion, RP is a suitable treatment option associated with few complications and excellent outcomes for selected healthy Korean men aged 75 years or older. Although the rate of urinary incontinence is higher in this patient group, the complication rates and outcomes are comparable to those of patients aged 65–69 years. Further studies using age-matched controls are necessary to compare the outcomes for RP against those for watchful waiting or hormone treatment in healthy elderly men with prostate cancer.
 XML Download
XML Download