

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The detection rate of early gastric cancer (EGC) is increasing due to improvements in diagnostic methods. EGC is defined as a lesion confined to the gastric mucosa or submucosa, without risk of regional lymph node metastasis (1). While advanced gastric cancer (AGC) has a 5-year survival rate of around 30%-60%, EGC has a good prognosis with a survival rate greater than 90% (2). Therefore, missing the presence of a synchronous cancer is more important for patients with EGC than AGC.
Two or more malignant cancer lesions in the stomach are often diagnosed during upper gastrointestinal endoscopy and are known as synchronous multiple gastric cancer (SMGC). Recently, the incidence of multiple gastric cancer is increasing due to development of endoscopic technology and the increasing use of a more detailed pathologic examination. SMGC is reported more commonly in association with EGC than with AGC, and SMGC associated with EGC is reported to account for 5%-15% of all gastric cancer cases (3456). Minimally invasive resection procedures such as endoscopic resection and laparoscopic surgery have been widely used in patients with EGC because of the desire to increase the quality of life (78). Therefore, SMGC is a very important issue to the clinician because there is a possibility of missing the presence of a cancer in the remnant stomach after minimal resection.
In particular, small lesions of SMGC can easily be overlooked. Patients with an overlooked cancer miss their chance for early diagnosis and treatment, and the gastric cancer is then allowed to progress to advanced cancer. For this reason, it is important to clarify the association between main and minor lesions in synchronous multiple early gastric cancer (SMEGC) that could lead to missing lesions or recurrence. However, no studies have investigated the characteristics and association of the main and minor lesions of SMEGC. Therefore, the aim of this study was to elucidate the clinicopathologic characteristics of and the association between the main and minor lesions of SMEGC.
MATERIALS AND METHODS
Study population
We retrospectively reviewed the medical records of patients who were diagnosed with EGC and were treated by endoscopic resection or surgical resection between April 2008 and May 2013 at Gachon University Gil Medical Center, Incheon, Korea. This study targeted patients who underwent initial treatment of EGC, and focused on main and minor lesions that were discovered during the first treatment of EGC. Informed written consent with adequate explanation was obtained from each patient before the treatment, and each treatment had been undertaken with curative intent.
Clinicopathologic characteristics
The location, macroscopic type, and the histological findings of the gastric cancers were categorized according to the Japanese Gastric Cancer Association criteria (9). In this system, the longitudinal location of the stomach is anatomically divided into three portions, the upper third (UT), middle third (MT), and lower third (LT). The cross-sectional circumference of the stomach is divided into four equal parts: anterior wall (AW), lesser curvature (LC), posterior wall (PW), and greater curvature (GC). The macroscopic type of tumor was divided into three types: (i) elevated (I, IIa and IIa + IIb); (ii) flat (IIb); (iii) depressed (IIc, IIc + III and III). The maximum diameter of the cancer lesion was measured as the tumor size.
The histological types were grouped as either differentiated types (papillary adenocarcinoma, well and moderately differentiated tubular adenocarcinomas) or undifferentiated types (poorly differentiated tubular adenocarcinoma, signet-ring cell carcinoma, and mucinous adenocarcinoma).
Definition
While solitary EGC was defined as a single malignant focus in a patient with EGC, SMEGC was defined as having two or more malignant foci. SMGC was defined according to Moertel’s criteria as follows (10): 1) each lesion is a pathologically proven malignancy; 2) each lesion is clearly separated from the others by microscopically normal gastric wall; and 3) the possibility that one of the lesions represents a metastatic tumor or a local extension must be ruled out.
The main and minor lesions of gastric cancer were also defined, in accordance with Moertel’s criteria, as follows: 1) if the depth of invasion of two or more lesions is equal, the one with the greatest diameter is regarded as the main lesion (also known as major lesions), with other lesions regarded as minor lesions (also known as accessory lesions) (10); and 2) if the depths of invasion are different in two or more lesions, the one with the greatest depth of invasion is regarded as the main lesion, with other lesions regarded as minor lesions. When there are more than three EGC lesions, the secondary main lesion is regarded as the minor lesion.
Procedure
The type of surgery (subtotal or total gastrectomy) and the extent of lymphadenectomy were determined by the attending surgeon depending on the location of the cancer and the intraoperative conditions of the patient. Curative R0 resection and D2 lymph node dissection according to the Japanese Gastric Cancer Association were performed when possible. As previously reported, endoscopic submucosal dissection was performed accordance to standard methods (1112). All of the patients underwent computed tomography with/without endoscopic ultrasonography before treatment.
Statistical analysis
Statistical analysis was performed using SPSS 12.0 software (IBM SPSS Statistics, IBM Corporation, Armonk, NY, USA) for MS Windows®. Categorical variables are presented as absolute numbers or percentages, whereas continuous variables are presented as means ± standard deviation (SD). Continuous data were analyzed using the independent t-test, and other categorical data were analyzed using the χ2 or Fisher’s exact test. We used a linear by linear association and correlation analysis to determine the interrelationship between main and minor lesions in patients with SMEGC. P values < 0.05 were considered statistically significant.
RESULTS
Patient characteristics
A total of 963 Korean patients who underwent endoscopic or surgical resection were diagnosed with EGC. Among these patients, 37/963 (3.8%) patients diagnosed with SMEGC were included in this study. The mean age of the SMEGC patients was 64.3 ± 9.6 years, and 33 (89.2%) patients were men. Among the 37 patients, 20 received surgery as their first treatment. Thirty-five patients had no lymph node metastasis, and two had lymph node metastasis. Twenty-eight patients had two lesions and nine patients had more than three lesions.
Correlation between main and minor lesions of patients with SMEGC
In patients with SMEGC, the mean size of the main and minor lesions was 28.0 ± 23.0 mm and 12.3 ± 7.5 mm, respectively. The main and minor lesion size showed a significant moderate positive correlation (r = 0.533, P = 0.001), as the size of the minor lesion increased when the main lesion increased in Fig. 1.
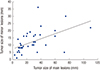 | Fig. 1Correlation of tumor size in main and minor lesions of SMEGC.
The line indicates a moderate linear relationship of tumor size between the main and minor lesions of SMEGC (r = 0.533, P = 0.001). SMEGC, synchronous multiple early gastric cancer.
|
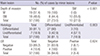
The comparison of characteristics between the main and minor lesions of SMEGC is summarized in Table 1. The main and minor lesions of SMEGC were mostly located at LT of the stomach, 64.9% and 46.0%, respectively. When the main lesion was at UT of the stomach, 83.3% of the minor lesions were also at UT, and when the main lesion was at MT of the stomach, 85.7% of the minor lesions were also at MT. Similarly, when the main lesion was at LT, 62.5% of the minor lesions were also at LT. When the main lesion was at AW, GC, PW, or LC of the stomach, 37.5%, 66.7%, 57.1%, and 84.6% of the minor lesions were found at the same location, respectively. The main and minor lesions of SMEGC showed the same vertical and horizontal locations in 70.3% and 64.9% of cases (P = 0.002 and P = 0.002), respectively.
Table 1
Comparison of characteristics between main and minor lesions of SMEGC
UT, upper third; MT, mid third; LT, low third; AW, anterior wall; GC, great curvature; PW, posterior wall; LC, lesser curvature.
![]()
As for macroscopic types, 50% of the minor lesions were the elevated type when the main lesion was elevated, 58.3% of the minor lesions were the flat type when the main lesion was flat, and 82.4% of the minor lesions were the depressed type when the main lesion was depressed. The association of macroscopic type was statistically significant at 67.6% for both the main and minor lesions of SMEGC to share the same type (P < 0.001).
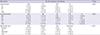
The other comparisons of characteristics between the main and minor lesions of SMEGC are summarized in Table 2. When the main lesion was a differentiated type, 90% of the minor lesions were differentiated, an association that was statistically significant (P = 0.003). When the main lesion did not have lymphovascular invasion (LVI), 93.9% of the minor lesions did not have LVI, and although 6.1% of the minor lesions had LVI, this did not reach statistical significance. Close to half (48.6%) of the main lesions were submucosal (SM) cancer, and when the main lesion was SM cancer, 55.6% of the minor lesions were also SM cancer (P < 0.001).
Table 2
Comparisons of additional characteristics of main and minor lesions in SMEGC
![]()
The matching characteristics of the main and minor lesions
The main and minor lesions were mainly differentiated types (both 81.1%). The main and minor lesions were the same differentiated types in 83.8% of cases. Twenty-six out of 37 (70.3%) showed both identical differentiation and LVI. Three microscopic characteristics, differentiation, LVI, and invasion of depth, were the same in both main and minor lesions in 62.2% of cases. Both the three microscopic characteristics and the type were matched in 43.2%, and 27% of cases had all six factors matched in Fig. 2.
 | Fig. 2The matching characteristics between the main and minor lesions of SMEGC.
The main and minor lesions had the same differentiation in 83.8% of cases. Three microscopic characteristics, including differentiation, LVI, and depth of invasion, were the same in 62.2% of the main and minor lesions. Both the three microscopic characteristics and the type were matched in 43.2%. All six factors matched in 27.0%, including the three microscopic characteristics, macroscopic type, and vertical and horizontal location. SMEGC, synchronous multiple early gastric cancer; LVI, lymphovascular invasion; VL, vertical location; HL, horizontal location.
|
DISCUSSION
SMEGC detected in the gastric mucosa after endoscopic resection or minimally invasive surgery is a major problem. Attention to the possibility is always required, because if not detected during initial treatment, early treatment opportunities may be lost because SMEGC will only be detected at an advanced stage.
Therefore, we investigated characteristics within the lesions of SMEGC, in order to increase the possibility of finding another lesion and decrease the number of missed gastric cancers. In particular, this study focused on EGC to compare the characteristics of the initial carcinogenic process. SMEGC studies focusing mainly on the associations between main and minor lesions, such as this study, are rare. In addition, this study used a strict definition of SMEGC, and unlike other studies (71314), targeted SMEGC that were concurrently treated with multiple EGC during initial treatment.
This study was conducted on 37 (3.8%) of 963 EGC patients. The prevalence of the disease was lower than has been reported in previous studies, 5%-15% (3456). The reason for the low prevalence in this study is thought to be due to several factors. First, the definition of SMEGC differs among the previous studies, and in some studies, it is defined to include any second lesion that has occurred within a year (71314). However, in this study it was strictly defined to be limited to multiple EGC that were detected during initial treatment. Secondly, the difference in prevalence may be due to the difference in race and region. Similar to this study, other studies held in South Korea have reported SMEGC prevalence of 3%-8% (1516).
In this study, the main lesion was significantly larger than the minor lesion, and there is an association in that as the main lesion becomes larger so does the minor lesion. Macroscopic types were identical type in 25/37 (67.6%), and the vertical and horizontal location in 17/37 (50%) were simultaneously identical. Finally, 12/37 (32.4%) showed both identical macroscopic type and location at the same time. This result shows that in over 1/3 of SMEGCs, the gross appearance of both main and minor lesions is similar and they have similar locations. These results correspond to previous studies of gastric cancer (514). They support the “collision tumor phenomenon” theory where the main and minor lesions occur adjacent to each other. However, it must be taken into account that regardless of the characteristics of the main lesion, the proportion of the minor lesions being located at UT and MT, and the occurrence of flat types are high (17).
For the microscopic findings, the similarity of invasion depth, presence of LVI, and the level of differentiation between the main and minor lesions were shown to be high: 29/37 (78.4%), 31/37 (83.8%), and 31/37 (83.8%), respectively. In 23/37 (62.2%), these three factors were identical. These results support the “field carcinogenesis” hypothesis, where the entire gastric mucosa has an identical carcinogenic background. According to this hypothesis, the risk factors and precancerous lesions such as Helicobacter pylori infection, atrophic gastritis, and intestinal metaplasia occur mainly in the distal stomach. The main and minor lesions of this study all occurred in the distal stomach as well.
The strength of this study lies in its elucidation of the ratio of identical characteristics present in the macroscopic and microscopic findings of main and minor lesions in SMEGC having statistical significance. In the case of multiple gastric cancers occurring within the same individual, the genetic and environmental backgrounds as well as the level of exposure to carcinogens is considered to be uniform across the entire mucosa of the stomach.
According to the results of this study, the identical characteristics between the main and minor lesions showed that microscopic findings were more similar than macroscopic findings that included location and gross appearance. Even if carcinogenesis begins, environmental factors that could be changed by continuous stimuli such as Helicobacter pylori, intestinal metaplasia, and life style, can affect the outcome of macroscopic appearance.
In molecular biology, it is known that gastric cancer has a high rate of genetic diversity, which is the base of its molecular phenotype (1819). These molecular phenotypes primarily contribute to histologic features and determine clinical diversity. Many mechanisms other than environmental factors are inter-connected. As further study is required on the effects of molecular phenotypes on morphological clinical characteristics, our results could contribute to encourage a focus on molecular and biologic analysis of SMEGC.
Because the development of endoscopic techniques is increasing the diagnostic rate of EGC, minimal invasive treatment is becoming more important. In addition, because it is known that the concurrence rate of SMGC in EGC is higher than that of AGC, the characteristics of minor lesions are clinically important (14). Therefore, it is critical to accurately detect SMEGC initially. Once an endoscopist has detected an EGC, a more meticulous endoscopic examination should be considered to identify a second EGC lesion. If the matching properties between the main and minor lesions are not overlooked when EGC is first detected or during follow-up, the possibility of missing cancers will be reduced.
The predisposing conditions of SMGC were reported in several previous studies: male, elderly people and intestinal types of gastric cancer were more likely to be susceptible (7). Most multiple gastric cancers are found in the MT and LT rather than the UT. SMGC is more likely to occur in association with well to moderately differentiated tumors than poorly differentiated ones (41420). Therefore, based on our results, clinicians should pay careful attention to finding other lesions in patients with these characteristics.
In conclusion, the main and minor lesions of SMEGC share similar clinicopathologic characteristics. If synchronous EGC is overlooked, the risk of recurrence will increase and prognosis will be poor. Therefore, when EGC is detected, the possibility of SMEGC should not be neglected, taking into account our understanding of the characteristics of the main and minor lesions.
 XML Download
XML Download