

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Restless legs syndrome (RLS) is one of the most common diagnoses in sleep medicine and is characterized by the urge to move the legs, which increases at night and is usually relieved by movement. RLS causes sleep disturbance. The exact pathogenesis of RLS is unknown (1). RLS patients especially have difficulty falling asleep or maintaining sleep (12). Criteria for the diagnosis of RLS were first introduced by the International Restless Leg Syndrome Study Group (IRLSSG) in 2003 (2). According to these, the urge to move the legs, worsening of symptoms with rest or inactivity, improvement with movement and impairment during evening or night hours compared to daytime are the diagnostic indicators of RLS (2). RLS is idiopathic in nature in most cases, but can be secondary to conditions such as diabetes mellitus (DM), renal failure, and iron deficiency anemia. The estimated prevalence of RLS in the general population ranges from 7% to 10% (1).
Urticaria is a common skin condition which is characterized by pruritic, pink or pale swellings (3). Chronic spontaneous urticaria (CSU) is defined as the persistent symptoms of urticaria for six weeks or more (34). CSU is a disorder of unknown etiology associated with nocturnal awakenings and difficulty falling asleep (35). Sleep deprivation has been shown to have harmful effects on behavioural, physiological and psychological functioning. Skin disorders may be associated with sleep disturbance and sleep deprivation, some associated with specific sleep disorders. There is very little literature focused on the frequency of sleep problems in the context of skin disorders (3). However, a study on this subject is not available so far in the literature.
In this study, we aimed to determine the frequency of RLS in patients with CSU and to explore the association between RLS and CSU.
MATERIALS AND Methods
Study population
In this cross-sectional study, 130 consecutive patients with CSU and 100 age and sex-matched healthy controls who were referred to the Dermatology and Venereology outpatient clinic between July, 2013 and September, 2015 were included in this study. Patients with CSU associated with an underlying disease (systemic lupus erythematosus, malignancy, renal or hepatic insufficiency, blood dyscrasia, malabsorption, hypertension, diabetes, allergic rhinitis or bronchial asthma, chronic infection, drug or alcohol abuse and other systemic disease), patients with physical urticaria, and urticaria due to medications or other known etiology, were excluded from the study. Healthy controls had no symptoms or history of urticaria, NSAID/aspirin hypersensitivity and any other causes of symptomatic RLS including uremia, anemia, diabetes, pregnancy, polyneuropathy, rheumatoid arthritis, and any other patients with abnormal findings on neurological examination or with accompanying neurological disorder. Healthy controls and patients with chronic non-steroidal anti-inflammatory drug (NSAID)/aspirin intake who took NSAIDs daily for at least 3 months were excluded from the study. Patients reported the severity of pruritus and disease duration.
Measurements
The urticaria activity score (UAS)
The UAS was calculated according to EAACI/GA2LEN/EDF guidelines (6). The UAS was estimated according to the number of wheals and pruritus intensity, applying the following scheme: no wheals/24 hr = 0, 20↓ wheals/24 hr = 1, 20-50 wheals/24 hr = 2, 50↑ wheals/24 hr = 3 and pruritus intensity: no pruritus = 0, mild (present but not annoying or troublesome) = 1, moderate (troublesome but does not interfere with normal daily activity or sleep) = 2, intense (severe pruritus, which is laborious enough to interfere with normal daily activity or sleep) = 3. UAS scores: daily (minimum = 0; maximum = 6). The UAS was classified as follows: 0-2 (mild), 3-4 (moderate) and 5-6 (severe) (6). Chronic urticaria patients were required to document their CU symptoms once daily for 4 weeks using a diary.
Visual analogue scale (VAS)
The VAS referring to overall urticaria severity during the preceding 2 weeks was completed by the patient at each follow-up appointment. The scale ranged from 0 to 10, 0 indicating no disease and 10 indicating very severe urticaria.
Evaluation of RLS
All patients and control subjects were interviewed about their general demographic characteristics, medications, and four essential criteria for RLS, as described by the International Restless Legs Syndrome Study Group (IRLSSG) (7). Patients with all diagnostic criteria of IRLSSG were diagnosed with RLS. The IRLSSG defined four criteria to allow a better recognition and standardization of this diagnosis: (i) RLS consists of an urge to move the legs in association with some paraesthesias and disagreeable sensations, such as crawling, aching or burning in the legs; (ii) the RLS sensations are relieved by movement (iii) the symptoms have circadian rhythmicity and are worse at night; and (iv) the symptoms are also worse during periods of rest, especially long periods of inactivity. International RLS Rating Scale (IRLS) (designed by the IRLSSG) was used to determinate the severity of RLS in patients with RLS (8).
Evaluation of sleep quality
Pittsburgh Sleep Quality Index (PSQI) is the most commonly used retrospective self-report questionnaire that measures sleep quality over the previous month. This self-reported questionnaire assesses sleep quality and contains 19 self-rated questions yielding seven components: subjective sleep quality (SSQ), sleep latency (SL), sleep duration (SD), habitual sleep efficiency (HSE), sleep disturbances (SDis), use of sleep medications (USM), and daytime dysfunction (DD). Each component is scored from 0 to 3, yielding a global PSQI score between 0 and 21. A high PSQI score indicates poor sleep quality. A global PSQI score greater than 5 identifies patients with poor versus good SQ with 89.6% sensitivity and 86.5% specificity (9). The Turkish version of the PSQI has been validated by Ağargün et al (10).
Statistical analysis
A power analysis demonstrated that 40 patients would be required in each group to detect significant differences in both groups with a power of 80% and a level of significance of α = 0.05. Statistical analyses were performed by SPSS 18.00 (Statistical Package for Social Sciences, SPSS inc, Chicago, IL, USA). Demographic characteristics and sleep quality of the patients and control groups were compared. Urticaria groups with RLS and without RLS were compared in terms of the demographic characteristics, disease duration, UAS, VAS scores and frequency of sleep disorders. PSQI scores of patients with RLS and non-RLS were compared. Normality of data was tested by Shapiro-Wilk test. Nominal variables were compared by Chi-Square tests. Numeric values were compared using Mann- Whitney test or Student t test. Spearman's nonparametric correlation test was used to evaluate the correlation between the parameters of PSQI scores and age, education level, RLS score, UAS and VAS score.
Ethics statement
This study protocol was reviewed and approved by the institutional review board of Akdeniz University School of Medicine (number 70904504/320) and was conducted according to the ethical standards of the Helsinki Declaration of 2000. All subjects submitted signed written informed consent.
RESULTS
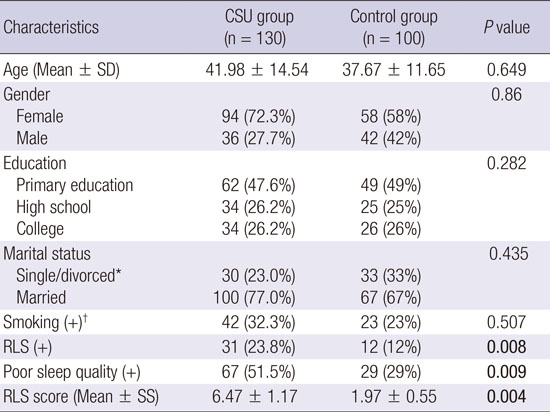
A total of 130 CSU patients with mean age 41.98 ± 14.54 and a control group consisting of 100 healthy individuals with mean age 37.67 ± 11.65 were included in the study. RLS was diagnosed in 31 (23.8%) of 130 patients with CSU and 12 (12%) of 100 healthy individuals. The number of patients with RLS in the CSU group was significantly more frequent than the control group (P = 0.008). The frequency of poor sleep quality and RLS score in the CSU group were significantly higher than the control group (respectively P = 0.009, P = 0.004). The demographic and clinical features of patients and the control group are shown in Table 1.
Table 1
Sociodemographic and clinical features of CSU group and control group
CSU, chronic spontaneous urticaria; RLS, restless legs syndrome.
*Only four divorced persons in CSU group and two divorced persons in control group,
†
Current smokers and former smokers
![]()
When we compared the demographic and clinical features of the patients with and without RLS in the CSU group, there was no significant difference between them in terms of VAS, UAS and poor sleep quality; but the mean ages of patients with RLS was higher than without RLS (P = 0.032) (Table 2). All PSQI scores of patients with CSU were significantly higher than the control group (Table 3). When we compared PSQI scores of patients with RLS and without RLS in the CSU group, subjective sleep quality (SSQ), sleep latency (SL) and habitual sleep efficiency of patients with RLS was higher than without RLS (respectively P = 0.016, P = 0.0097, P = 0.035) (Table 4). The frequency of poor sleep quality in the CSU group without RLS was higher than the control group (P = 0.001). Similarly, the frequency of poor sleep quality in the CSU group with RLS was higher than the control group (P = 0.001). Total PSQI scores in the CSU group were correlated with VAS, UAS and RLS scores (Table 5). There was no correlation between CSU and RLS (P = 0.377, r = 0.107) (Fig. 1).
Table 2
Clinical and demographic features of RLS (+) patients and RLS (-) patients in the urticaria group
RLS, restless legs syndrome; UAS, urticaria activity score; VAS, visual analog scale for severity of itch; BMI, body mass index.
![]()
Table 3
PSQI scores of CSU and control groups
CSU, chronic spontaneous urticaria; SSQ, subjective sleep quality; SL, sleep latency; SD, sleep duration; HSE, habitual sleep efficiency; SDis, sleep disturbances; USM, use of sleep medications; DD, daytime dysfunction; PSQI, Pittsburgh sleep quality index.
![]()
Table 4
PSQI scores of RLS (+) patients and RLS (-) patients in the urticaria group
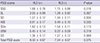
PSQI, Pittsburgh sleep quality index; RLS, restless legs syndrome; SSQ, subjective sleep quality; SL, sleep latency; SD, sleep duration; HSE, habitual sleep efficiency; SDis, sleep disturbances; USM, use of sleep medications; DD, daytime dysfunction; Total PSQI score, total Pittsburgh sleep quality index score.
![]()
Table 5
Correlation between RLS score and demographic/clinical parameters with PSQI scores
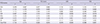
RLS, restless legs syndrome; PSQI, Pittsburgh sleep quality index; UAS, urticaria activity score; VAS, visual analog scale for severity of itch; SSQ, subjective sleep quality; SL, sleep latency; SD, sleep duration; HSE, habitual sleep efficiency; SDis, sleep disturbances; USM, use of sleep medications; DD, daytime dysfunction; Total PSQI score, total Pittsburgh sleep quality index score.
*Spearman’s correlation coefficient.
![]()

DISCUSSION
In this study we showed that the prevalence (23.8%) of RLS in the CSU group was significantly higher than the control group (12%). The frequency of poor sleep quality and RLS score in the CSU group were significantly higher than the control group. Also, total PSQI scores in the CSU group were correlated with VAS, UAS, and RLS scores.
RLS is classified into the sleep disorders according to the international classification of sleep disorders. RLS is associated with nighttime sleep disturbance and subsequent daytime fatigue and sleepiness (111213). Its prevalence in the general population is estimated between 5% to 15% (1). In our study, the prevalence of RLS in the CSU group was increased approximately 2-fold while it was similar to the general population in the control group. Also, RLS scores and poor sleep quality in CSU group were higher than in the control group. These results suggest that sleep quality and RLS severity are affected by the presence of CSU. This may also be through the effect of pruritus.
A study on the quality of sleep of CSU patients is not available so far in the literature. We showed that the number of patients with poor sleep quality in the CSU group was higher than in the control group. Maurer et al. (14) reported that almost all patients with CSU suffer somewhat from sleep disturbances three nights per week. The pruritus is one of the cardinal symptoms and the most important reason for sleep disturbances of patients with CSU. The pruritus severity is significantly associated with impaired sleep quality in patients with CSU (51516). We also found that the pruritus severity has been correlated with PSQI, VAS and RLS scores in patients with CSU (1718). We believe that the reason for this increase of RLS score in patients with CSU is pruritus.
In our study, subjective SQ and sleep latency scores of the patients with RLS were higher than the patients without RLS. RLS and CSU may be a potentiating effect on the sleep.
The pathophysiology of RLS is still unclear; nevertheless, the following mechanisms have been claimed: iron-related mechanisms, including reductions in iron and ferritin levels in the cerebrospinal fluid (CSF); genetic factors associated with altered brain iron levels; and altered microvascular flow in the legs (19). Some neurotransmitters are speculated to play an important role in specific types of urticaria (19). Monoaminergic dysfunction, especially involving the dopaminergic system, is also thought to play a role in the pathophysiology of RLS (20). As the dopamine is a prerequisite for the synthesis of noradrenaline, dopaminergic dysfunction in RLS affects noradrenergic neurotransmission as well (20). It can be argued that there is a vicious cycle between them while the exact the cause-and-effect relationship is unknown. While this association between RLS and CSU may have a biological explanation based on the abnormal monoaminergic neurotransmission system, the findings call for a more careful approach to CSU patients in order to improve their quality of sleep and their well-being.
We specify that our study also had a number of limitations. First, we surveyed a small sample of patients with urticaria. As such, our results may not be representative of patients with urticaria. Second, we did not perform any form of sleep monitoring, so our analysis was based on self-reported symptoms.
We claim that pruritus of urticaria may decrease the quality of sleep in patients with RLS and it may trigger and worsen the restless legs syndrome. Furthermore RLS and CSU may share common etiology. More comprehensive prospective studies are needed in this regard.
 XML Download
XML Download