

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The relationship between seasonal variation and urolithiasis attack is reported in several studies (1234). Urolithiasis incidence increases during summer and decreases during winter. It is generally attributed to the effect of seasonal variations in temperature on urinary volume, due to excessive perspiration and dehydration. Low urine volume is an important factor mostly of an environmental nature that directly increases the urinary saturation of stone-forming salts.
These studies on the effect of temperature on urolithiasis were usually based on data from a limited area of the country or on inadequate climatic data due to minimal temperature changes over 4 seasons. Seoul, the capital city of Korea, has 4 distinct seasonal changes and an average annual temperature of 13°C comparable to cities in Europe. The conditions are more acceptable in studying the association of climate and urolithiasis. Moreover, these studies were limited by assessment of temperatures only in summer or extreme conditions, and assessment of lag periods between exposure and outcome that may have missed significant delayed association between high daily temperatures and urolithiasis presentation. The precise relationship between temperature and urolithiasis thus remains uncertain.
The precise relationships between temperature and urolithiasis differ by region, age, and gender. It is critical to policies for preventing the health impacts of heat wave, as it is used as an indicator for initiating public health response actions to heat waves or issue heat wave warnings. The rate of increase of urolithiasis above temperature can also be used as an assessment of vulnerability and the evaluation of public health response (5). Heat-related urolithiasis was reported to increase steeply above a certain level, with similar outcomes for health impact. Nevertheless, the pattern of incidence of urolithiasis and its relationship with temperature have rarely been investigated in Korea.
Therefore, we tested the hypothesis that urolithiasis is etiologically influenced and/or determined by temperature trends in association to other meteorological factors. Additionally, we defined the overall cumulative exposure-response and the lag response relationships between daily temperature and urolithiasis presentation in Seoul.
MATERIALS AND METHODS
Emergency department (ED) database
This multicenter study used 9-year data (from January 2005 to December 2013) of the 4 hospitals. The 4 hospitals included Myongji Hospital, Chung-Ang University Hospital, Seoul Medical Center and Korean Electric Power Corporation (KEPCO) Hospital. The nearest meteorological observatory was Seoul weather observation station. These hospitals are located west, south, east, and north region of Seoul, respectively.
The records of the patients who visited the emergency department (ED) were retrieved from the database of each hospital. Using Korean Classification of Disease-6 (KCD) codes, based upon International Classification of Disease (ICD) 10th version, N20.0 (calculus of kidney), N20.1 (calculus of ureter), N20.2 (Calculus of kidney with calculus of ureter) or N20.9 (Urinary calculus, unspecified) among the patients who visited the ED, we obtained patients’ personal coding number, age, and visited date without other personal information. Repeated visits of the same coded patient within 7 days were regarded as the same stone and only the first visit was used for analysis.
Meteorological data acquisition
Meteorological data including daily temperature, relative humidity, wind, sea level pressure, and hours of sunshine were obtained from the website of Korean Meteorological Administration (www.kma.go.kr). The web site provides annual reports with monthly meteorological data of every observatory station. Therefore, we could search monthly meteorological data of Seoul observatory station of the applicable year. We used the daily mean temperature, relative humidity, wind, sea level pressure, and hours of sunshine.
Statistical methods
Inferential statistical analysis was performed in 2 progressive model stages. The response variable is the number of daily ED visits and its subgroup counts: females, males and males of specific age (younger than 40 years old, between 40 to 60 years old, and older than 60 years old). Several different covariates were included in the model: all climate covariates, daily mean temperature, relative humidity, wind, sea level pressure, and hours of sunshine, day of week (DOW1-Monday, 7-Sunday). We also included years, and months to control seasonal variations and trend.
The first stage was divided into 2 consequential procedures based on the construction of a simple Poisson generalized regression model (PGAM) applied to the time series, aimed to estimate, preliminary, the association of several meteorological covariates and the daily number ED visits. This procedure was conducted in a backward mode with all the climate covariates included and response variable, the number of daily accesses to ER visits. A natural cubic spline to control seasonal variations was included (time 7*9), and day of week (DOW). Finally, the Akaike Information Criterion (AIC) was used to find the best fit model.
As the second stage, we performed a time series study using distributed lag nonlinear models (DLNMs) to estimate the relationship between mean daily temperature and urolithiasis presentation (6). We evaluated two aspects of the association between temperature and urolithiasis presentation. First, we estimated the relative risk (RR) of urolithiasis presentation associated with daily mean temperatures for each day during a 20-day period after the temperature exposure (lag-response). RRs were estimated over the distribution of mean daily for each urolithiasis presentation relative to a mean daily temperature of 13°C, the mean temperature in Seoul. Second, we assumed the estimated risks for each lag day to estimate the cumulative RR for urolithiasis presentation associated with daily mean temperatures during the 20-day period after the temperature exposure (cumulative exposure-response relationship).
We created Poisson regression models, allowing for overdispersion for each city as follows:
Yt - Poisson(μ) = α + βTt,l + S(RHt) + DOWt + montht + yeart
Where t represents the day of observation; Yt the observed stone counts on t; α, the intercept; l, the lag day; Tt,l the cross-basis matrix of temperature and lag: S(RHt), the cubic spline of relative humidity on day t; and DOWt the indicator variable for day of the week at day t to control for daily fluctuations in outdoor activities. Months and year were indicator variables to control for season, temperature trends and differences in the annual at-risk population. Statistical significance was defined as P < 0.05. Analyses were performed with R (version 3.0.1; R Project for Statistical Computing; http://www.r-project.org/) using the dlnm package.
Ethics statement
This study was approved by the institutional review board of Myongji Hospital (IRB No. MJH-15-051). Because this was a retrospective study on anonymous patients, we were waived in getting informed patient consent. However, the study was carried out in agreement with the Declaration of Helsinki.
RESULTS
Monthly urolithiasis presentation and meteorological data
During the 9 years, the population of Seoul ranged from 9.9 million to 10.1 million, which is 19.9%-20.6% of the total Korean population.
A total of 14,518 renal colic patients visited the ED of 4 hospitals due to urolithiasis. Male patients were 9,712 (66.9%) and female patients were 4,806 (33.1%). Of the male patients, 4,425 (30.5%) patients were younger than 40 years old; 4,143 (28.5%) patients were between 40 to 60 years old; and 1,144 (7.9%) patients were older than 40 years old. During the 9 years, the mean daily temperature was 12.6℃ (-14.5-27.7℃); relative humidity was 60.4% (20-97%) ; wind was 2.5 (0.7-7.5) m/sec; sun shine time was 5.7 (0-13.5) hours; and sea level pressure was 1,016.0 (993.1-1,038.1) hPa.
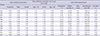
ED visits for urolithiasis were higher in July, August and September, the summer season in Seoul, and peaked in August, as compared to January and February, winter in Seoul. The same trend occurred according to gender and ages (Table 1). Temperature and relative humidity were prominently higher in summer than winter season; and the 9 years data showed a similar seasonal variation pattern (Table 1).
Table 1
Monthly meteorological variables and urolithiasis presentation
Poisson generalized regression model (PGAM)
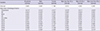
We constructed a statistical model of the PGAMs family (statistical stage 1) in the backward mode adjusted for time and calendar factors, by first including all meteorological covariates and then eliminating those with low significance. We observed an association of the temperature in all cohorts, and a negative association of the relative humidity in all patients, males, males less than 40 years old and males between 40 and 60 years old, whereas no significance was observed for other 3 parameters (wind, sea level pressure, and sun shine (Table 2). We included relative humidity in DLNMs because relative humidity showed a negative association with urolithiasis presentation. For a given temperature, when humidity is low and the air is dry, more water is lost through the skin, thus decreasing urine volume and increasing the supersaturation of calcium and uric acid in the urine.
Table 2
Poisson model with meteorological factors adjusted for seasonal and calendar before backward procedure
Overall cumulative exposure-response relationship
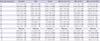
Associations between mean daily temperature and urolithiasis presentation were not monotonic, and there was variation in the shape of exposure-response curves and the strength of associations at different temperatures. However, in most cases RRs increased for temperatures above the reference value of 13°C except males more than 60 years old. RRs for urolithiasis presentation cumulated over a 20-day period associated with a mean daily temperature of 29°C, as compared with 13°C with 2.54 in all patients (95% confidence interval [CI], 1.67-3.87), 2.59 in males (95% CI, 1.56-4.32), 2.42 in females (95% CI, 1.15-5.07), 3.83 in males less than 40 years old (95% CI, 1.78-8.26), and 2.47 in males between 40 and 60 years old (95% CI, 1.15-5.34).
The temperatures over 10°C that showed statistically significant associations were first observed along the groups (Table 3). Heterogeneity was also noted at the limits of the temperature ranges. There were similar associations in male and female patients, but males less than 40 years showed higher RR compared to other groups. In the female group, RRs for urolithiasis presentation cumulated over a 20-day period associated with a mean daily temperature of -10°C, as compared with 13°C with 0.41 (95% CI, 0.19-0.91), (Table 3). Relative humidity was not a statistically significant predictor of the risk of urolithiasis presentation (data not shown).
Table 3
RR (95% CI) of urolithiasis presentation cumulated over a 20-day lag period associated with mean daily temperature (°C) relative to 13°C based on data from residents of Seoul, 2005-2013
Lag response
We estimated bimodal increases in the RR of urolithiasis presentation for days in which temperature were 27, 29, and 31°C relative to days with mean temperatures of 13°C. The strongest association between urolithiasis presentation and daily mean temperatures of 27, 29, and 31°C versus 10°C was estimated for lags less than 5 days; and higher temperature showed higher RRs during 5 days (Fig. 1A). The RRs after hot days at 10-20 days lag were heterogeneous in males. A trend of increased risk was found in males less than 40 years old, and in males more than 60 years old showed a decreased risk, whereas in males between 40 and 60 years old varied around null after 10 days (Fig. 1A).
Fig. 1
Lag-response association at different temperatures and exposure-lag response surface. (A) Lag response between 27, 29, and 31°C (mean) day and urolithiasis presentation relative to 13°C over a 20-day period in all patients, males, females, males younger than 40 years old, males between 40 and 60 years old, and males older than 60 years old in Seoul from 2005 to 2013. For each group, the estimated RRs of urolithiasis presentation in association with a daily mean temperature of 27, 29, and 31°C (relative to 13°C) for each lag day form temperature exposure during a 20-day are shown. (B) Risk of urolithiasis presentation relative to 10°C along temperature and a 20-day lag period in all patients, males, females, males younger than 40 years old, males between 40 and 60 years old, and males older than 60 years old in Seoul from 2005 to 2013. The 3-dimentional relationships include temperature (x-axis), lag (z-axis), and RR of urolithiasis presentation (y-axis). The point estimate of the relative risk (RR) of urolithiasis presentation at each point in the temperature range and lag window is shown using 13°C as the reference temperature.

RR along exposure-response curve and lag
We constructed 3-dimensional graphs to demonstrate simultaneously the relationships along temperature and lag (Fig. 1B). Consistent trends of increasing RR of urolithiasis presentation were observed within 5 days of high temperatures across all groups. However, confidence intervals cannot be represented in these figures, and therefore the precision of the estimates could not be appreciated.
DISCUSSION
Our study identified the effect of seasonal variation of urolithiasis presentation. Mean daily temperature and relative humidity were significant factors associated with urolithiasis presentation among the climate parameters. We observed that as daily temperatures increased to > 13°C, the risk of urolothiasis presentation over next 20 days also increased in all groups except males older than 60 years old. The lag between high daily temperatures and the risk of urolithiasis presentation was short, with the maximum risk occurring within 5 days of temperature exposure. Our estimations suggested that there is a graded increase and that time between hot days and urolithiasis presentation is short.
We hypothesized that the estimated RRs of urolithiasis presentation across a range of temperatures represent patients presenting with calcium-based urolithiasis, the most common type of stones in Korea and other developed countries. Dehydration, the proposed casual mechanism through which high temperatures would act, increases the supersaturation of calcium and uric acid, thus promoting calcium stone formation on the apatite deposits. Modeling and laboratory experiments suggested that stones grow over a span of hours in the proper urinary environment and that growth rates are dramatically increased by increasing urinary supersaturation of calcium (78).
There were 4 main findings in our study. First, the existence of an association was confirmed between relative humidity, and the number of urolithiasis presentations, however it did not exist in the overall cumulative exposure-response relationship. The hypothesis supports that dry climate increases in urolithiasis formation is mainly dependent on dehydration. There are conflicting reports on whether humidity correlates with urolithiasis formation and presentation rate (1356). Acute disruption of skin from environments with relative humidity as low as 10%, produce an initial increase in transdermal water loss (TEWL) (910). Cravello and Ferri (11) exposed human subjects to variable ambient temperature and relative humidity to determine the dependency of each variable on average skin temperature. They showed a greater influence on skin temperature by ambient temperature with a minor contribution by relative humidity. Furthermore, TEWL was more dependent on ambient temperature than relative temperature in the temperature range. The limited variation of humidity of Seoul might explain why temperature overwhelms humidity in distributed lag nonlinear models. Moreover, it would be interesting to examine not only the role of climate but the role of a specific location in relation to climate and time spent outdoors.
Secondary, a heterogeneous influence of temperature was demonstrated according to patient age, in that variations of temperature were less effective in males older than 60 years old. With adjustment by the population number of age group, the rate of stone incidence was the highest in the 60-69 years old in Korea. The research had some limitations since it would be necessary to consider other potential etiological factors in addition to the meteorological variables in the statistical model. This is thought to be due to the fact that males less than 60 years old engage in outdoor activities more frequently than any other groups, and thus are more exposed to environments with high temperature. Moreover, a diet rich in animal protein is possibly associated with increased urinary calcium excretion and a decreased excretion of citrate (121314). Metabolic syndrome had also been considered an independent risk factor in the onset of urolithiasis in Korea (1516). Moreover, old people have comorbidities such as hypertension and diabetes that are well-established risk factors for urolithiasis. Meterological factors might less affect old people due to their other lithogenic factors.
Third, the association with temperature was more accurate in females than males; and at below -10°C, the risk of urolithiasis presentation over the next 20 days decreased. Thus, females appear to have greater temperature variation. In general, females show greater variability in physiologic variables, including systolic blood pressure and relative plasma volume due to lower lean body mass (1718). The higher variability in physiologic variables seen in females suggests an overall physiology that may be more adaptable to changing circumstances. An alternative hypothesis is that female have a lower incidence of chronic diseases and males consistently have a greater prevalence of urolithiasis than females.
Fourth, the lag between high temperature and urolithiasis was short such that the risk of increasing RR of urolithiasis presentation was observed within 5 days of high temperatures. The observed lag response is strikingly similar to other studies. Tasian et al. (6) reported that the lag response was short, with the maximum risk occurring within 3 days of exposure and persistently of a mild elevated RR at 10-20 days in Philadelphia; and Fletcher et al. (19) reported at case-crossover study in which the maximum odds for admission for nephrolithiasis after high daily temperature were also observed at 3 days. Within 7-10 days of the temperature exposure, we observed that the increased RR of urolithiasis presentation was immediately followed by decreases in RR. We attributed this phenomenon to “harvesting” of urolithiasis cases in subjects who would have had urolithiasis at a future time, but for whom heat caused the event to occur earlier. Harvesting of susceptible cases possibly reflects the causal mechanism of urolithiasis formation and explains the short lag between hot days and urolithiasis presentation. In patients who are predisposed to urolithiasis formation, low urinary volume resulting from sweating on hot days may result in spontaneous urolithiasis nucleation, and/or small asymptomatic urolithiasis, and/or small asymptomatic stones that enlarge enough to become symptomatic.
RR can be fundamental to making decisions related to investing resources and implementing policies to prevent urolithiasis in a region or a population group, or in deciding when to issue a heat warning. RR can be helpful in determining vulnerable groups. In this study, the incidence of urolithiasis increased according to the temperature rise in females and males less than 60 years old. Such a trend can be changed by preventive action and management, besides un-modifiable factors such as gender and age. Therefore, preventive and management policies against heat-related urolithiasis can be evaluated based on RRs.
One of the limitations of this study was that ED visits are not representative of all urolothiasis cases in Seoul. In Korea, most patients usually visit the urology outpatient clinic and not the ED during the day, except patients with very severe pain. Therefore, patients who visited ED were a sub-group of all the urolithiasis patients. However, we controlled this confounding factor by adjustment of the day of week, and selected 4 hospitals located in the west, east, south, and north regions of Seoul. Further study on the entire population using the health care department data is expected. We acknowledge an additional limitation to this study. Temperature-dependent models presume an accurate understanding of current urolithiasis prevalence; however, such data are problematic for a variety reasons. Urolithiasis occurs intermittently and is not always readily apparent. Many patients harbor undiagnosed asymptomatic urolithiasis, whereas others require repeated hospitalizations for recurrent urolithiasis events. Consequently, true urolithiasis prevalence is difficult to determine and is likely to be routinely under estimated and occasionally overestimated. And subanalysis of stone size on CT scan was not evaluated in this study. Actually in the retrospective study, reviewing stone size on CT scan is difficult. Therefore, prospective multicenter study is necessary.
Despite these limitations, the results of our study suggested that specific periods of temperature exposure might be associated with an increased risk of urolithiasis. Additional research is needed to demonstrate whether an intervention such as increasing fluid intake among patients with increased risk for urolithiasis can reduce the frequency of urolithiasis episodes. Further research is needed to confirm these results and access potential intervention strategies during the periods of increased climate associated risk.
Urolithiasis presentation increased with high temperature with higher daily mean temperatures, with the strongest associations estimated for lags of only a few days, in Seoul, a metropolitan city in Korea. These findings further support the adverse effect of high temperature on urolithiasis.
 XML Download
XML Download